
Abstract
Study design:
Three-dimensional kinematic analysis and surface electromyography (EMG) of 10 male adults with complete spinal cord injury (C7 to L2).
Objective:
To examine movement patterns and muscular demands in individuals with spinal cord injury (SCI) during posterior transfers.
Setting:
Pathokinesiology Laboratory at a Rehabilitation Centre, Montreal, Canada.
Methods:
Kinematic variables that described the positions and angular displacements of the head, trunk, shoulder and elbow were obtained by videotaping markers placed on the subject segments. EMG data were recorded for the biceps, triceps, anterior deltoid, pectoralis major, latissimus dorsi and trapezius muscles of the dominant upper extremity during posterior transfers using surface electrodes. To quantify the muscular demand, the EMG data recorded during the transfers were normalized to values obtained during maximal static contractions (EMGmax). The mean muscular demand was calculated for every muscle during the lift phase of the transfers. The lift phase was determined by pressure-sensitive contacts.
Results:
All subjects were able to execute the posterior transfers on an even surface, whereas nine subjects completed at least one of the transfers to the elevated surface. A forward-flexion pattern at the head and trunk was observed when either one or two hands remained on the lower surface, whereas a lift strategy was seen when both hands were placed on the elevated surface. Transferring to the elevated surface with hands on the lower surface required inferior electromyographic muscular utilization ratio (EMUR) than the transfer on the even surface for all muscles. The lowest EMUR were calculated for the transfer to the elevated surface with hands on the lower surface (triceps (18%), pectoralis major (53.8%), trapezius (66%) and latissimus dorsi (24.5%)) while performing the same transfer with hands on the elevated surface generated the highest EMUR (triceps (40.2%), anterior deltoid (73.2%), trapezius (83.6%) and latissimus dorsi (55.3%)).
Conclusions:
Subjects presented different movement characteristics and muscular demands during the posterior transfers. It is suggested that the forward-flexion pattern improves the dynamic trunk stability and reduces the muscular demand required to transfer. High muscular demand developed when hands were positioned on the elevated surface might be due to increased postural control demands on the upper limb and reduced angular momentum.
Similar content being viewed by others


Introduction
Despite the importance of achieving an optimal level of independence during transfer activities, it is surprising that the ability to transfer independently has not been studied extensively and that only limited biomechanical knowledge is available. Since the trunk and upper extremities act as the primary motor components during transfer activities in individuals with spinal cord injury (SCI), it is believed that better understanding of the kinematic patterns and electromyographic activity at the trunk and upper extremities would contribute to evidence-based practice in spinal cord rehabilitation.
Some studies1,2,3,4,5,6,7,8,9 have analyzed movement patterns and measured muscular demand (MD) during weight-relief and transfer activities in individuals with SCI. Reyes et al1 have shown that people with paraplegia primarily used their pectoralis major and latissimus dorsi with the triceps to simultaneously elevate the trunk and extend the elbows when performing a weight-relief raise. Further, it was suggested that paralysis of the triceps might not limit the ability to extend the elbow during a raising maneuver since individuals with C5 and C6 tetraplegia solicit to a larger extent their pectoralis major and anterior deltoid to compensate the triceps action.2 Recent biomechanical studies hypothesized that this involvement of the anterior deltoid and the upper pectoral muscles facilitate the generation of the shoulder flexor moment needed to extend the elbow during weight-shift maneuvers (closed kinetic chain) among individuals with SCI.3,4 These results were found to be in accordance with the muscular demand measured at the anterior deltoid and pectoralis major during closed kinetic chain elbow extension among healthy subjects.5 Perry et al have analyzed transfers from wheelchair to a mat platform (level surface) in subjects with low-level paraplegia. Their results revealed that moderate to high muscular demand was required at the upper extremity muscles to accomplish the task.6 The highest demand was observed during the depression strategy that solicited the serratus anterior in the arm contralateral to the direction of displacement and the stemal pectoralis major in the leading arm. Recently, it was demonstrated that individuals with high-level SCI presented significantly higher muscular demands at the pectoralis major, trapezius, anterior deltoid and biceps than low-level SCI participants during a posterior transfer on a level surface.7,8 Unexpectedly, but in agreement with the results of Perry et al, the long head of the triceps demonstrated consistently low level of activity throughout the posterior transfer. Lastly, lateral transfers have been studied by Allison et al.9 These authors found that, in the frontal plane, lateral transfer initiated from a long sitting position was achieved with either a translational strategy (head and pelvis move simultaneously in the same direction) or a rotational strategy (head moves in opposite direction to the pelvis) while, in the sagittal plane, a forward-flexion or a lift technique was observed. Although it is not clear as to which factors determine the movement strategy during the lateral transfer, the observed pattern suggests that individuals with stronger triceps might select the forward-flexion technique to optimize their relative arm lengths or the position of the center of mass relative to the hands. Similarly, individuals with poor eccentric trunk control might prefer the lift technique since it provides a safer option in term of equilibrium and balance.
To compensate for the lack of postural muscle control affecting the ability to transfer, individuals with SCI gradually develop new patterns of postural control that are starting to be investigated.10,11 Recent studies confirmed the contribution of the latissimus dorsi, trapezius, pectoralis major and serratus anterior in maintaining and restoring sitting balance among individuals with SCI subjects.10 In addition, these compensatory muscle strategies were more important for individuals with high level of lesion since the residual sensorimotor potential was the most limited.11 As a result, preliminary work to increase trunk stability during transfer activities through the use of a prototype trunk orthosis and orthotic device to facilitate transfers has been initiated.12,13
Individuals with SCI often have to transfer toward an elevated surface (eg bed transfers, car transfers, floor to wheelchair transfers using a push-up technique, climbing up stairs using a push-up technique). It is suggested that transferring toward an elevated surface might be more challenging than transferring on an even surface for individuals with SCI because of the mechanical disadvantages associated with this particular task. It is also hypothesized that limited trunk stability and reduced strength at the trunk and the upper extremities will influence the movement strategies and the muscular demand used by each subject during transfer activities towards an elevated surface. The objective of this study was to compare the movement strategies and the muscular demand of six muscles during posterior transfers on an elevated surface from three initial hand positions and to compare them to a posterior transfer on an even surface. It was hypothesized that, in comparison to the posterior transfer to an even surface, the transfers toward the elevated surface, will produce different movement patterns at the head, trunk and upper limbs and will generate higher demands on the active muscles. We also suspected that some subjects with a high lesion of the spinal cord will not be successful in performing some of the tasks towards the elevated surface.
Methods
Subjects
A group of 10 males (volunteers) with spinal cord injury (SCI) of various levels (C7–L2) participated in this study. Their mean (SD) age was 39.2 (9.3) years and their mean time post-injury was 15.1 (11.7) years (Table 1). The inclusion criteria consisted of a muscle strength score of the triceps brachii higher than 3/5 when evaluated by manual muscle testing14 and a degree of impairment of A or B according to criteria for neurological classification.15 All participants presented no clinical evidence of musculoskeletal disorders affecting the upper extremities or any other condition limiting their abilities to perform the posterior transfers. Ethical approval was obtained from the Research Ethics Committee. All subjects reviewed and signed a written informed consent before entering the study.
Clinical evaluation
All subjects underwent a clinical evaluation that included a neurological examination (dermatomes, myotomes and spasticity) and an assessment of the level of function. The evaluation of dermatomes and myotomes was performed according to the Standards for Neurological and Functional Classification of SCI as proposed by American Spinal Injury Association15 to determine sensory and motor index scores, respectively. A sensory score of 224 defines normal sensation, whereas a maximum value of 100 can be reached for the motor score. The spasticity index16 measured the Achilles tendon reflex, the passive resistance to dorsiflexion and the amount and duration of the clonus at the ankle. The total spasticity index score ranges from 0 (no spasticity) to 16 (severe spasticity). The Functional Independence Measure (FIM) was used to determine the functional capacity of all participants.17 The FIM consists of 18 items graded on an ordinal scale ranging from 1 (dependent) to 7 (independent) for a maximum possible score of 126 points.
Dynamometric assessment
The dynamometric assessment was performed to evaluate the strength of several muscle groups acting at the shoulder girdle and to determine the maximum electromyography (EMG) values of six shoulder muscles. Subjects were seated on the chair of the dynamometer (Biodex Medical System Inc., Shirley, NY, USA). The backrest was positioned to allow 80° of hip flexion, while the lower extremities were supported to form an angle of 90° at the knees. An optimum level of stabilization (external fixation and manual stabilization) was provided to the shoulder girdle, trunk, pelvis and lower extremities. The axis of the dynamometer was aligned with the axis of the shoulder or elbow joint. The maximal torque in flexion and extension at the elbow, in flexion, extension, adduction at the shoulder and in depression at the shoulder girdle were assessed. The tests were randomly performed on the dominant side. The joint positions selected for these tests corresponded to the joint positions used by the subject during the experimental tasks.
During these efforts, maximum EMG values (EMGmax) of six muscles on the dominant side of the subjects were recorded using surface electromyography. Muscles tested included: the long head of the biceps brachii, the long head of the triceps brachii, the anterior fibers of the deltoid, the clavicular part of the pectoralis major, the latissimus dorsi and the lower fibers of the trapezius. Active bipolar surface electrodes (Delsys Inc., Boston, MA, USA) (model DE-2.1) were placed perpendicular to the direction of the muscle fibers following skin preparation and were then connected to a multichannel acquisition system. The analog myoelectric signals were amplified by a Nihon Kohden module AP-621G (Nihon Kohden America inc., Foothill Ranch, CA, USA) and an AM System differential AC amplifier 1700 EMG (A-M Systems Inc., Sequim, WA, USA) with overall gains of 1000 with low and high cutoff frequencies set at 20 and 500 Hz, respectively. Analog EMG signals were digitized and collected at a sampling rate of 1200 Hz. The digital EMG signals were full-wave rectified and smoothed with a low pass filter of 3 Hz to obtain linear envelopes across the transfer activities.
During the maximal static contractions, subjects were encouraged to progressively increase their efforts to their maximum strength levels and to maintain this level for a minimum of 1 s. The protocol included three static contractions for every movement tested and 2-min rest periods between repetitions. The torques were corrected for the effects of gravity created by the weight of the upper limb and the accessories to which it was attached. The mean value of the three maximal efforts determined the maximal static strength in a specific direction (elbow flexion and extension, shoulder flexion, extension, adduction and shoulder girdle depression) as well as the EMGmax activity of each muscle studied (biceps, triceps, anterior deltoid, latissimus dorsi, pectoralis major and trapezius). The EMG electrodes remained in place for the biomechanical analysis of the transfers.
Transfer assessment
All individuals with SCI were invited to perform two different posterior transfers (Figure 1). The first transfer was a backward movement from a long sitting position on an even surface with hands placed symmetrically alongside the body (even task). In the second transfer, subjects had to raise themselves sufficiently from a long sitting position on a low surface to land on an elevated surface (height=10 cm; width=90 cm; depth=30 cm) with a backrest angled at 70° (elevated task). For the elevated tasks, subjects were instructed to perform the transfer using three distinct hand placement strategies: both hands on the lower surface, both hands on the elevated surface and one hand on each of these surfaces. The first and second hand positions were symmetrical. In one case, both hands were placed on the mat platform (lower surface) while hands were positioned on the elevated surface in the second case. In the third case, hand positions were asymmetrical: the dominant hand (tested upper extremity) was on the elevated surface, while the nondominant hand remained on the lower surface. The posterior transfer on the even surface was performed using only standardized initial hand placement position: hands symmetrically placed on each side of the body on the mat platform (lower surface). After a familiarization period, subjects performed a minimum of three trials for each task using their normal movement strategies. Posterior displacement distance and speed of movement were not standardized across subjects but were held constant for all trials executed by a given subject Rest periods between transfers were planned to prevent fatigue. The posterior transfers were divided into three phases for analysis: prelift, lift and postlift. The start and end of the transfer lift phase were identified by the initial and final vertical pressure variations detected with pressure-sensitive contacts placed under the ischii of the subjects. Periods of 1 s before and after the lift phase described the prelift and postlift phases, respectively. The three phases were time normalized to 100% to generate a total of 300% for the complete analysis of the transfer task.

Schematic representation of the posterior transfers on an even and elevated surfaces. Three initial hand placements were tested with the posterior transfers toward the elevated surface
Kinematics
An estimate of direct linear transformation parameters within the experimental volume was completed using a rigid three-dimensional (3D) calibration frame. First, a static anatomical calibration was performed for each participant using 21 reflective markers. The subjects were asked to maintain a long sitting position with the tested shoulder (dominant side) in a neutral position and the tested elbow in full extension midway between pronation and supination. Then, six markers were removed and a set of 15 reflective markers (Figure 2) defining the head, trunk, arm and forearm segments were used to estimate the 3D position and displacement of these segments during the posterior transfers. The movement patterns were recorded at 60 Hz using a two-camera video technique to capture the trajectories of the markers. The x, y and z coordinates of each marker were digitized using a Peak Performance system (Peak Performance Technologies, Inc., Englewood, CO, USA). The coordinates were smoothed with a second-order digital filter using a cutoff frequency between 2 and 8 Hz. Following analysis of the kinematic data using a custom-made MatLab 5 program (The MathWorks Inc., Natick, MA, USA), movement patterns and angular displacements of the head, trunk, arm and forearm around all axes of movement as well as the relative angular displacements at the elbow and shoulder were calculated. Three-dimensional kinematics and EMG data were synchronized by means of common electric impulses sent to each acquisition system to outline the movement pattern and muscular demand associated with the transfer activities.

This illustration shows the location of the three noncollinear markers used to define the segments of the model (head, trunk, arm and forearm). Markers not attached to the triads defining the segments were used for anatomical calibration and were removed during the experiment
Muscular demand
The muscular demand was estimated using the electromyographic muscular utilization ratio (EMUR).18,19 This ratio allowed to determine the level of effort generated by each muscle during the posterior transfers. The EMUR was obtained by dividing the EMG recorded at any given time during the transfer by the EMGmax obtained from maximal effort done on the dynamometer. The result was multiplied by 100 to provide a percentage. The EMUR increases with the level of effort up to a theoretical value of 100%, which indicates that the subject has fully activated the muscle. EMURs for the muscles studied have been computed for all phases of the transfer and mean values were only calculated for the lift phase since most of the EMG activity observed was generated during this phase.
Descriptive statistics were calculated for relevant subject characteristics and clinical variables. Since subjects used various strategies during the transfers (reference and experimental tasks), only descriptive statistics will be reported with emphasis placed on the range of values of angular displacement and EMUR.
Results
Clinical evaluation and dynamometric assessment
The results of the clinical evaluation are presented in Table 1. The ASIA motor score ranged from 27 to 58 with a maximum attainable score of 100, whereas the ASIA sensory score ranged from 79 to 163 out of a possible 224 points. The mean (SD) spasticity score measured at both ankles reached 11.9 (5.3) thereby revealing the presence of mild spasticity among the subjects. The mean (SD) score of the FIM (total score) reached 119 (4.4) out of 126 thereby indicating an elevated functional capacity of the subjects. The results of the dynamometric assessment are presented in Table 2. The mean (SD) normalized strength values revealed that the shoulder adductor and flexor muscles are the strongest muscles among most of the participants. A total of six subjects generated their highest torque values during the adduction movement (pectoralis major), whereas another three participants developed their maximum values during the shoulder flexion movement (anterior deltoid).
Movement strategies and kinematic assessment
All subjects completed the posterior transfer on an even surface without difficulty. For the elevated surface, one subject (subject #3) was unable to perform the posterior transfers despite the three different initial hand placement strategies assessed. Data for this subject were excluded from the kinematic and electromyographic analyses. Seven subjects (#2, 4, 6, 7, 8, 9 and 10) successfully completed the transfer using both hands on the lower surface, five subjects (#1, 6, 8, 9 and 10) were able to execute it with one hand on each surface and only three subjects (#4, 5 and 7) performed the transfer with both hands on the elevated surface.
The mean head, thorax, shoulder and elbow movement patterns observed in flexion/extension are presented in Figure 3. In general, similar movement patterns were observed during the posterior transfer on the even surface as compared to the elevated surface. An exception to this observation was the posterior transfer toward the elevated surface using both hands on the elevated surface. During the prelift phase (0–100 of the normalized time), overall, the head was maintained in an almost neutral alignment with the trunk and a minimal forward flexion of the upper trunk was observed while a minimal shoulder extension, combined with a minimal elbow flexion, was measured at the upper extremity. The only exception was observed when both hands were positioned on the elevated surface. In this case, the head was leaning forward and shoulder extension was greater compared to the other posterior transfers.

This figure illustrates the mean angular displacements at the head and the trunk relative to the vertical as well as the relative angular displacement at the shoulder and elbow during the posterior transfers. Upward values indicate flexion (head, trunk and shoulder) and extension (elbow). The start and end of the prelift, lift and postlift phases are identified by the vertical dotted lines. The angular displacements presented are not necessarily similar to the ones found in Table 3 because of the normalization of the duration of the lift phase
Most of the angular displacements needed to perform the transfer activities were generated during the lift phase (Table 3). During this phase (100–200 of the normalized time), a near-full extension of the elbow followed by a flexion of the head, upper trunk and shoulder were observed for the even surface and elevated surface transfers. In general, the magnitude of angular displacement for the transfers on the elevated surface was found to be comparable to that obtained during the transfer on the even surface. A reduction of head and trunk flexion was measured when using both hands on the elevated surface (Table 3), as opposed to the other hands positions. It was also observed that a biphasic movement pattern clearly occurred at each joint during the transfers that used both hands on the elevated surface. This biphasic movement involved: head flexion preceded extension, shoulder extension appeared before flexion and elbow flexion was followed by an extension.
EMUR
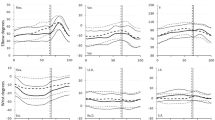
The patterns of the mean muscular demand (MD) measured for the biceps brachii, the triceps brachii, the pectoralis major, the anterior deltoid, the trapezius and the latissimus dorsi are illustrated in Figure 4. These patterns clearly show that the highest EMURs were observed during the lift phase (100–200 of normalized time) for all muscles, whereas a low EMUR was required during the pre- and postlift phases for all transfers. The magnitude of the EMUR for the triceps brachii, the pectoralis major, the anterior deltoid and the latissimus dorsi tended to be different between the transfer on the even surface and the transfers on the elevated surface, whereas the levels of activity of the biceps and the trapezius muscles were similar for all transfers. In the transfer executed with both hands on elevated surface, most of the muscles studied (biceps, triceps, pectoralis major and latissimus dorsi) reached their highest EMUR during the first part of lift phase (100–150 of the normalized time), whereas in other transfers, the EMG appeared gradually during the lift phase to reach a maximum and decreased after, except for the latissimus dorsi muscle.

This figure illustrates the mean EMUR of the muscles studied during the posterior transfers. The start and end of the prelift. lift and postlift phases are identified by the vertical dotted lines. The EMUR presented are not necessarily similar to the ones found in Table 4 because of the normalization of the duration of the lift phase
The mean (SD) EMUR calculated during the lift phase of all transfers (Table 4) suggested that MDs are high (>50%) in the anterior deltoid, pectoralis major and trapezius during all posterior transfers. The muscular demands of the biceps and the latissimus dorsi were moderate (25–49%) during the transfers on an even surface and during the transfers on the elevated surface using either the hands on the low surface or one hand on each surface. However, the transfer with both hands on the elevated surface solicited high EMUR (>50%) of the latissimus dorsi. Moderate EMUR was found at the triceps when transferring to the elevated surface using one hand or two hands on the elevated surface. The muscular demand of the triceps was low (<25%) only when both hands remained on the lower surface and reached a moderate level (25–49%) when at least one hand was positioned on the elevated surface. The highest mean EMUR for the biceps was obtained when the transfer activity was initiated with both hands on the lower surface, whereas the transfer with hands on each surface produced the highest mean EMUR in the pectoralis major (Table 4).
The mean EMURs obtained during the transfers on the even surface (reference task) were not the lowest ones. Mean EMURs for anterior deltoid, pectoralis, trapezius were high and surpassed some of the values obtained for the transfers on the elevated surface (experimental task). The transfer on the elevated surface executed with both hands on the lower surface showed the lowest mean EMUR values for all muscles except the biceps (34.5%) and anterior deltoid (56.6%). Meanwhile, using both hands on the elevated surface tended to increase EMURs for all muscles except the biceps (15.7%) and pectoralis major (55.5%).
Discussion
The purpose of this study was to examine the movement patterns and muscular demands required to perform posterior transfers on an even surface and on an elevated surface (10 cm) among individuals with SCI. In addition to a clinical assessment, the study integrated dynamometric, electromyographic and kinematic analyses of the transfer activities.
We expected that some individuals with SCI would not be able to accomplish posterior transfers toward an elevated surface. In fact, one subject (#3, level of lesion T2) failed to achieve all transfers to the elevated surface. The clinical evaluation revealed that this subject was the heaviest among all participants while the dynamometric assessment suggested that his strength, normalized to body weight, was comparable to many other participants even though he demonstrated the highest normalized elbow extension strength (triceps). Moreover, when he attempted the transfer with one hand on each surface, supramaximum mean EMUR values were recorded at the trapezius (303.2%) and the pectoralis major (145.4%), thereby suggesting that this subject solicited the maximum potential of these muscles. The mean EMUR for the triceps (21.7%) was the lowest suggesting that its strength should not be considered a clinical indicator for posterior transfers. Other factors such as excessive body weight, length of the arm and muscle weakness of other muscle groups might have accounted for the reduced ability to transfer.
The transfer with both hands on the lower surface appeared to be the preferred method of transfer toward the elevated surface since seven subjects out of 10 were able to execute the transfers. The forward flexed posture observed when both hands were kept on the low surface may have displaced the center of mass anteriorly to the ischial tuberosities within the base of support. This may have resulted in improved dynamic trunk stability throughout the task and reduced the risk of falling backward thereby providing a safer option for participants. In fact, the center of mass of the head, arm and trunk, located in front of the 11th thoracic vertebra and just below the xyphoid process, is lowered and kept anterior to the ischial tuberosities when the trunk is flexed forward.20,21,22 Conversely, the placement of both hands on the elevated surface (n=3) required a large amplitude of shoulder extension and might have limited forward flexion of the trunk during the lift phase. In addition, this important amplitude of extension required at the shoulders may create further musculoskeletal stress at the shoulder when placing both hands on the elevated surface. This might explained the limited number of participants who were able to successfully perform the task using this technique. The transfer with one hand on each surface (n=5) appears to be a compromise between the previous two techniques. During this transfer, the pectoralis major reached its highest EMUR during the lift phase (100–200 of the normalized time). The asymmetry of the task possibly challenged the lateral postural control of the trunk despite a larger mediolateral base of support. Consequently, the ability to ensure the dynamic sitting balance in individuals with SCI is a factor that might influence the movement strategy and EMUR required when performing a transfer.
The kinematic analyses highlighted two distinct movement patterns: a forward flexion strategy and a lift strategy. The first pattern was observed during the posterior transfers on an even surface and during the posterior transfers on elevated surface when either both hands were on the lower surface or one hand on each surface. The kinematic analysis of these tasks showed a considerable amount of head and trunk flexion combined with some shoulder flexion and elbow extension by the upper extremity. This axial skeletal pattern may have generated an angular momentum that facilitated the elevation and posterior displacement of the pelvis and lower extremities. A similar action–reaction relationship (head–hip) was previously identified in individuals with SCI who had limited lifting capacity.23 The second pattern was recorded when transferring onto the elevated surface with both hands on the elevated surface. The kinematic analysis revealed an important reduction of head, trunk and shoulder flexion combined with a significant amount of elbow extension during the lift phase of the transfer (Figure 1). The limited amount of flexion of the axial skeleton restricted the action–reaction pattern previously described. Since less angular momentum was available to facilitate the elevation and posterior displacement, a greater amount of elbow extension and shoulder flexion strength were required. The high EMUR in most muscles also indicated that strength of these muscles was important to execute the posterior transfers with both hands on the elevated surface and some of them contributed to the elevation and posterior displacement of the pelvis and lower extremity. A particular feature of this type of transfer is the biphasic nature of the upper extremity patterns in which shoulder extension and elbow flexion precedes shoulder flexion and elbow extension, respectively. This movement pattern in which the agonist muscles are stretched before shortening is known to promote energy generation during the shortening phase either by facilitating the stretch reflex or by releasing elastic energy stores in the previous lengthening phase.24,25,26 The high muscle activation observed at the beginning of the lift phase also supports this interpretation. The posterior transfer with hands on the elevated surface appears to be the most challenging approach in terms of the muscular effort required thereby explaining why only three subjects could successfully rely upon it to perform the task. Similar forward flexion and lift patterns have been reported in the sagittal plane when individuals with SCI performed a lateral transfer from a long sitting position.9 Future studies should include the rate of angular displacement of the trunk to further support this interpretation.
Different levels of muscle activation were generated during the posterior transfers to the even and elevated surface as demonstrated by the mean EMUR patterns for all muscles. The initiation of the lift phase (prelift) gave rise to a progressively increasing muscular demand in all muscles. This initial loading period required progressively increasing activity of the supporting muscles of the trunk and upper extremity to initiate the necessary changes in segment positions at the trunk, the shoulder and the elbow during the lift phase. Inversely, the intensity of the EMG progressively decreased during the unloading period of the lift phase (post-lift), although the trunk and shoulder musculature were still very active in order to control the descent of the body weight.
The mean (SD) EMUR for the anterior deltoid and pectoralis major were 64.9% (6.9) and 64.6% (11.6), respectively, during the lift phase of all transfers that solicited shoulder flexion and elbow extension at the upper extremity. This highlights the contribution of the anterior deltoid and pectoralis major to shoulder flexion and elbow extension in a closed kinetic chain as previously described.3,4,5 The trapezius was also found to be very active particularly during the transfer with one hand on each surface (80%) and both hands on the elevated surface (83.6%). The elevated demand of this muscle might be compatible with the depression and adduction of the scapula needed to assure its fixation to the thorax in order to provide maximum proximal stabilization to the muscles acting at the shoulder region. In addition, the reversed action of the trapezius during this closed kinetic chain activity might assist the trunk elevation therefore further supporting an elevated EMUR.
The latissimus dorsi presented a surprisingly inferior muscular demand (24.5–55.3%) in this study when compared to the results obtained from previous weight relief raise maneuvers in individuals with SCI.1,2,6 This muscle contributes to the extension, adduction and internal rotation of the shoulder. Since the muscle was activ ated in a closed kinetic chain during the posterior transfer, its functional origin and insertion were mechanically reversed. Consequently, the low muscular demand of the latissimus dorsi can be explained by the fact that the activation of this muscle would have generated an anterior displacement of the lower trunk and pelvis girdle instead of a posterior one as expected during the posterior transfers. However, the higher muscular demand (55.3%) documented when both hands were placed on the elevated surface suggested a larger contribution of this muscle to the shoulder girdle depression to maintain the lower trunk and pelvis anterior to the elevated surface during the lift phase prior to the posterior displacement. Moreover, this might have prevented the sacrum from rubbing against the surface and would assure the integrity of the skin. The result obtained from the lift technique is consistent with previous results obtained during a weight-relief raise (58%) among individuals with SCI.1
A remarkable difference in muscular demand was found between the pectoralis major and the latissimus dorsi during the transfers on an even and elevated surface (both hands on the lower surface and one hand on each surface). This might be attributed to the flexed posture of the trunk that placed elevated demand on the pectoralis major. This postural strategy might have facilitated the posterior displacement since the arm length relative to the transferring surface during the lift phase was optimized and facilitated the elbow extension and shoulder flexion necessary for clearance of the pelvic girdle during the transfer.27,28 The presumed angular momentum initiated by flexion of the head and the upper trunk around the glenohumeral joint axis contributed to the lift and posterior displacement of the pelvis. The forward flexion of the trunk associated with moderate to high activation of the thoracohumeral musculature might functionally bypass the glenohumeral joint thereby avoiding excessive loading of the glenohumeral joint and protecting the rotator cuff muscles.1,6
An elevated muscular demand of the triceps was expected throughout the lift phase of all transfers. Only moderate muscular demand was found when transferring with one hand on each surface (33.4%) and both hands on the elevated surface (40.2%). The elevation of the pelvis and lower extremities was assured by a greater amount of active elbow extension when both hands were placed on the elevated surface thereby producing the highest mean EMUR for the triceps. This high activation is probably needed to equilibrate the expected large external moment created by the reaction force under the hands. In fact the larger elbow flexion observed when the hands were placed on the elevated surface as compared to the other hands positions displaces the joint axis posteriorly relative to the position of the force vector thus creating a larger moment. Future biomechanical analysis might confirm this hypothesis. The results of the present study suggested that factors other than optimal strength of the triceps have to be considered in transfer activities. Poor eccentric control of the forward trunk flexion (trunk extensors) might figure among these factors as previously reported.9 In comparison, the mean EMUR for the triceps during the lift phase was low (<25% EMUR) when both hands were kept on the low surface to transfer to the even or elevated surface despite the significant extension movement observed at the elbow. In addition, the long head of the triceps might underestimate the activity level of the medial and lateral heads of the triceps since there is considerable shoulder flexion accruing in the transfers toward the elevated surface. These results are in accordance with those reported by Perry et al,6 which documented a muscular demand of 11% to 19% at the triceps during a depression transfer among low level paraplegics.
At the same time, minimum to moderate EMUR (25–50%) occurred at the biceps during the lift phase. The reaction force under the hands was directed posteriorly during the initial displacement and a flexor moment was needed to equilibrate this reaction force. In fact, the reverse action of the biceps is believed to contribute to the shoulder flexion moment needed during the lift phase to support the body weight through the flexed elbow as previously documented.2,6,29 Also, this muscular demand might have resulted from the dynamic contribution of the biceps to the stabilization of the glenohumeral joint since body weight was supported on an extended shoulder during this phase.6
Caution should be exercised when interpreting the EMUR from one upper extremity during the posterior transfer with one hand on each surface since similar EMUR cannot be assumed for both upper extremities. One should remember that only the dominant upper extremity placed on the elevated surface was evaluated and that the nondominant one kept on the lower surface may have contributed to varying degrees to the lift and posterior displacement associated with the transfer. Also, the supramaximum mean EMUR values may have resulted from an underestimation of the maximum EMG values. The lack of motor unit activation during the unidirectional static dynamometric testing could be explained by the fact that the muscles under investigation were multiaxial and acted in varying degrees as stabilizers (static) as well as prime movers (dynamic) during the dynamic posterior transfers.
Conclusion
This study provides biomechanical information that can be used to improve the functional mobility rehabilitation programs designed for individuals with SCI. Surprisingly, the transfer toward the elevated surface did not require a greater amount of muscular demand than did the transfer on the even surface. The results suggest that transferring to a 10-cm elevated surface can be performed using two distinct movement patterns: a ‘forward flexion’ pattern and a ‘lift’ pattern. The ‘forward flexion’ pattern, observed when at least one hand remained on the lower surface, is based on the conservation of the angular momentum generated at the axial skeleton by various muscles prior to lifting the body. This strategy facilitates the lift and posterior displacement of the pelvis and lower extremities to the elevated surface, thereby not only facilitating the dynamic trunk control but also reducing the muscular demand during the lift phase. Furthermore, the lowest EMUR at triceps (18%), pectoralis major (53.8%), trapezius (66%) and latissimus dorsi (24.5%) were calculated when both hands remained on the lower surface. Conversely, the ‘lift’ pattern is seen when both hands are placed on the elevated surface during the transfer. This strategy restricts the forward flexion of the axial skeleton on the weight-bearing upper extremities due to the important shoulder extension initially present. Moreover, the utilization of this strategy depends on the work capacity of the subjects with SCI since important muscular effort is required both to lift and shift the pelvis between the weight-bearing upper extremities and to dynamically control the landing of the trunk on the elevated surface. In fact, the triceps (40.2%), anterior deltoid (73.2%), trapezius (83.6%) and latissimus dorsi (55.3%) presented their highest EMUR while transferring using this technique.
Specific stretching and strengthening rehabilitation programs are essential for individuals with SCI who experience difficulty during transfer activities. Strengthening the thoracohumeral (pectoralis major), scapulothoracic (trapezius) and shoulder (deltoid) muscles would reduce muscular demand when transferring to either the even or elevated surface while weight-bearing on the upper extremities as evidenced by the very high EMUR for these muscles. Traditional strengthening programs focusing on the triceps and latissimus dorsi should be expanded to include the pectoralis major and inferior trapezius especially for individuals with SCI who use a ‘forward flexion’ pattern to transfer. Strengthening of the anterior deltoid is also relevant, but additional caution is suggested among individuals who present deficiencies of the thoracohumeral depressor to prevent possible shoulder impingement syndrome. Finally, rehabilitation programs should also target the development of new patterns of postural control at the trunk given its impact on movement strategies and muscular demand during functional transfer activities.
References
Reyes ML, Gronley JK, Newsam CJ, Mulroy SL, Perry J . Electromyographic analysis of shoulder muscles of men with low level paraplegia during a weight relief raise. Arch Phys Med Rehabil 1995; 76: 433–439.
Harvey L, Crosbie J . Biomechanical analysis of weight-relief maneuver in C5 and C6 quadriplegia. Arch Phys Med Rehabil 2000; 81: 500–505.
Gefen JY, Gelmann AS, Herbison GJ, Cohen ME, Schmidt RR . Use of shoulder flexors to achieve isometric elbow extension in C6 tetraplegic patients during weight lift. Spinal Cord 1997; 35: 308–313.
Marciello MA, Herbison GJ, Cohen ME, Schmidt R . Elbow extension using anterior deltoids and upper pectorals in spinal cord injured subjects. Arch Phys Med Rehabil 1995; 76: 426–432.
Zerby SA, Herbison GJ, Marino J, Cohen ME, Schmidt RR . Elbow extension using the anterior deltoids and the upper pectorals. Muscle Nerve 1994; 17: 1472–1474.
Perry J, Gronley JK, Newsam CJ, Reyes ML . Electromyographic analysis of the shoulder muscles during depression transfers in subjects with low level paraplegia. Arch Phys Med Rehabil 1996; 77: 350–355.
Gagnon D, Nadeau S, Gravel D, Noreau L, Larivière C, Gagnon D . Biomechanical analysis of a posterior transfer maneuver on a level surface in individuals with high and low spinal cord injuries. Clin Biomech 2003; 18: 319–331.
Gagnon D, Nadeau S, Gravel D, Noreau L, McFadyen B . Electromyographic analysis of the shoulder musculature during simulated bed mobility activity in patients with spinal cord injury. Arch Phys Med Rehabil 2000; 81: 1617.
Allison GT, Singer KP, Marshall RN . Transfer movement strategies of individuals with spinal cord injuries. Disabil Rehabil 1996; 1: 35–41.
Seelen HAM, Potten YJ, Huson A, Spaans F, Reulen JPH . Impaired balance control in paraplegic subjects. J Electromyogr Kinesiol 1997; 7: 149–160.
Seelen HAM, Vuurman EFPM . Compensatory muscle activity for sitting posture during upper extremity task performance in paraplegic persons. Scand J Rehab Med 1991; 23: 89–96.
Allison GT, Singer KP . Assisted reach and transfers in individuals with tetraplegia: toward a solution. Spinal Cord 1997; 35: 217–222.
Parry I, Johnson A, Ortiz R, Skinner S, James M . A new orthotic device to facilitate transfers in people with tetraplegia. J Spinal Cord Med 2002; 25: S42.
Clarkson HM . Musculoskeletal Assessment Joint Range of Motion and Manual Muscle Strength. Lippincott, Williams & Wilkins: Philadelphia, PA, 2000.
American Spinal Injury Association. International Standards for Neurological Classification of Spinal Cord Injury. American Spinal Injury Association: Chicago, IL, 2000.
Levin MF, Hui-CHan CWY . Relief of hemiparetic spasticity: tens is associated with improvement in reflex and voluntary motor functions. Electroencephalogr Clin Neurophysiol 1992; 85: 131–142.
Center for Functional Assessment Research. Guide for Uniform Data Set for Medical Rehabilitation (Adult FIM), Version 4.0. Buffalo, New: York: State University of New York at Buffalo, 1993.
Richards CL, Malouin F, Durand A, Moffet H . Muscle activation level comparisons for determining functional demands of locomotor tasks. Semin Orthop 1989; 4: 120–129.
Hébert LJ, Gravel D, Arsenault B . Comparisons of mechanical and electromyographical muscular utilisation ratios. Scand J Rehab Med 1995; 27: 83–88.
Lehmkuhl LD, Smith LK . Brunnstrom's Clinical Kinesiology. F.A. Davis Company: Philadelphia, PA, 1983.
Collot A . Le rôle joué par le muscle grand dorsal dans I’équilibre assis d’un paraplégique de niveau métamérique élevé. Ann Kinésithér 1979; 6: 283–301.
Winter DA . Biomechanics and Motor Control of Human Movement. John Wiley: New York, 1990.
Somers MF . Spinal Cord Injury: Functional Rehabilitation. Appleton & Norwalk: Norwalk, CT, 1992.
Komi PV . The Stretch-Shortening Cycle and Human Power Output. Jones NC, McCartney N, McComas AJ (eds) Human Muscle Power. Human Kinetic Books: Champaign, IL, 1986.
Vyse WM, Kramer JF . Interaction of concentric and eccentric muscle actions during continuous activation cycles of the elbow flexors. Physiother Can 1990; 42: 123–127.
Bosco C, Tarkka I, Komi PV . Effect of the elastic energy and myoelectrical potentiation of triceps surae during stretch shortening cycle exercise. Int J Sports Med 1982; 3: 137–140.
Ford JR, Duckworth B . Physical Management for the Quadriplegic Patient. FA Davis Company: Philadelphia, PA, 1987.
Bromley I . Tetraplegia and Paraplegia: A Guide for Physiotherapists. Churchill Livingstone: London, 1986.
Harvey LA, Crosbie J . Weight bearing through flexed upper limbs in quadriplegics with paralyzed triceps brachii muscles. Spinal Cord 1999; 37: 780–785.
Acknowledgements
This study was supported in part by the Réseau Provincial de recherche en adaptation-réadaptation du Fonds de recherche en santé du Québec. We gratefully acknowledge Mr Michel Goyette, ing, Mr Daniel Marineau, and Mrs Marie-Hélène Milot for their technical assistance.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Gagnon, D., Nadeau, S., Gravel, D. et al. Movement patterns and muscular demands during posterior transfers toward an elevated surface in individuals with spinal cord injury. Spinal Cord 43, 74–84 (2005). https://doi.org/10.1038/sj.sc.3101660
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101660
Keywords
This article is cited by
-
Wavelet coherence as a measure of trunk stabilizer muscle activation in wheelchair fencers
BMC Sports Science, Medicine and Rehabilitation (2021)
-
Elbow problems in paraplegic spinal cord injured patients: frequency and related risk factors—a preliminary controlled study
Spinal Cord (2013)
-
Movement strategies during car transfers in individuals with tetraplegia: a preliminary study
Spinal Cord (2012)
