
Abstract
Background:
Conventional anthropometric measurements are time consuming and require well trained medical staff. To use three-dimensional whole body laser scanning in daily clinical work, validity, and reliability have to be confirmed.
Methods:
We compared a whole body laser scanner with conventional anthropometry in a group of 473 children and adolescents from the Leipzig Research Centre for Civilization Diseases (LIFE-Child). Concordance correlation coefficients (CCC) were calculated separately for sex, weight, and age to assess validity. Overall CCC (OCCC) was used to analyze intraobserver reliability.
Results:
Body height and the circumferences of waist, hip, upper arm, and calf had an “excellent” (CCC ≥ 0.9); neck and thigh circumference, a “good” (CCC ≥ 0.7); and head circumference, a “low” (CCC < 0.5) degree of concordance over the complete study population. We observed dependencies of validity on sex, weight, and age. Intraobserver reliability of both techniques is “excellent” (OCCC ≥ 0.9).
Conclusion:
Scanning is faster, requires less intensive staff training and provides more information. It can be used in an epidemiologic setting with children and adolescents but some measurements should be considered with caution due to reduced agreement with conventional anthropometry.
Similar content being viewed by others

Main
Anthropometric data are the base for the assessment of growth and development and thus essential for the differentiation between physiological and pathological processes. Measurements and ratios like the body mass index (BMI) (1), the waist circumference (WC), the waist-to-height-ratio (WHtR) (2) and the neck circumference (NC) (3) are used to evaluate the nutritional status and to detect obesity and the risk of related secondary diseases (4,5). Accordingly, anthropometric measurements are highly important for daily clinical practice, but single measurements can only be interpreted correctly on the base of standards and reference values. These norms have to be compiled specifically for sex, age, ethnicity etc. and will be outdated after some time due to factors like secular trends or population mobility. Traditionally the measurements are taken with instruments like tape measure, stadiometer, and caliper. These techniques are easily available and well known, but there are some drawbacks. Standardization of measurements is needed as well as thorough training of observers to minimize intra and interobserver errors (6). Examination can be very time consuming measuring regions of complex anatomy and the necessary body contact may be unacceptable due to religious or cultural reasons (7).
Three-dimensional whole body scanning is a relatively new technique to gather anthropometric data in medicine, although the scanning technology itself is available for some time. The Loughborough anthropometric shadow scanner for example was introduced in 1989 (8) as one of the first automated whole body scanning systems. The technology of extracting spatial data out of (stereo-) photographs is even older (9). Today most of the available scanning systems are laser-based, use structured light, stereophotogrammetry or a combination of the above (10,11) and calculate a three-dimensional point cloud of the scanned object by the principle of optical triangulation (12). The scanning of whole persons is quite common in industries like apparel and ergonomics (13,14,15), but in current medical usage most applications focus on single parts of the human body, e.g., for cosmetic and reconstructive plastic breast surgery (16,17,18), cancer radiotherapy (19), questions on facial morphology (20,21) or the monitoring of cranial deformities (22). The most important advantage of the body scanning technology is the opportunity to describe a spatial shape with three-dimensional coordinates instead of reducing it to one dimensional measurements, which is important e.g., for the body surface area (23). Furthermore, a single whole body scan is completed in a few seconds. The resulting digital model of the scanned object can be saved easily and stored as a data file for a long time. Measurements can be extracted by calculating distances and angles between every point out of the point cloud with special software. Because of the high grade of automation, the quality of anthropometric data is supposed to be less dependent on the single observer. Nevertheless, the technology should only be used in epidemiologic research and clinical applications if the measurements are valid and reliable. For adults precision, accuracy, reliability, and partly validity of different scanning systems are confirmed by various studies (12,24,25,26,27), whereas some authors described significant differences between the technologies (28). In addition, there is only little research done in pediatrics regarding three-dimensional body scanning (29). Most of the existing validation studies with children and adolescents are either concerning selected diseases, e.g., idiopathic scoliosis (30) or limited to single anatomic regions (31).
Therefore, the purpose of this study is to evaluate validity and intraobserver reliability of a Vitus Smart XXL whole body laser scanner (Human Solutions, Kaiserslautern, Germany). We compared the body scanner with conventional anthropometry in a group of 473 healthy children and adolescents recruited from the study cohort of the Leipzig Research Centre for Civilization Diseases (LIFE-Child, NCT02550236) (32). The study population was stratified for age, weight, and sex ( Table 1 ). About 24 measurements of the body scanner were analyzed in comparison to eight measurements of conventional anthropometry ( Table 2 ). In addition, we established an offset correction technique. All measurements were performed in triplicate.
Methods
Study Population
The study population consisted of children and adolescents from the LIFE-Child study cohort. LIFE is a longitudinal cohort study representing the population of the city of Leipzig. LIFE-Child as a part of the LIFE Research Centre is recruiting 5,000 children and adolescents and their families as well as 2,000 pregnant women with the aim to evaluate how environmental, metabolic, and genetic factors affect development and health from fetal life to adulthood (32). Over a 2-y period, all at least 6-yr-old children and adolescents visiting the LIFE-Child department were asked to participate in this feasibility study by giving their agreement and/or a parental agreement to perform the anthropometric examinations in triplicate. We included 250 boys and 223 girls aged 6.1–17.8 y. Younger participants were not included since we observed that they were often unable to keep the scanning posture correctly. The population ( Table 1 ) was classified in three age groups (≥ 6 and < 10; ≥ 10 and < 14; ≥ 14 and < 18 y old) and three weight groups stratified for BMI-SDS (≤ −1.28 underweight; > −1.28 and < 1.28 normal weight; ≥ 1.28 overweight) in accordance to recommendations of the Arbeitsgruppe Adipositas (AGA, Working Group Obesity) (33). BMI-SDS were calculated using childsds (34) with the reference data from Kromeyer-Hauschild (35) and ranged from −2.78 to 4.34. All procedures performed in this study involving human participants were in accordance with the Ethics Committee of the University of Leipzig (Reg. No. 264-10-19042010) and with the 1964 Helsinki declaration and its later amendments. Informed consent was obtained from participants and their parents. For participants under the age of 12, written consent was obtained only from parents. From the age of 12, written consent was also obtained from the participants themselves.
Measurement Protocol
The anthropometric measurements were part of a larger number of assessments during a visit at the LIFE-Child department. Measurements were taken in triplicate by one observer per child but different observers across all children. Participants undressed to underwear for both assessments. The observers were trained for conventional and body scanner measurements by one supervisor and performed the assessments under guidance first. A correct measurement technique was re-evaluated consistently by the supervisor.
Conventional anthropometry was performed using a tape measure with a precision of 0.1 cm for circumferences and a stadiometer “Dr. Keller I” (Längenmesstechnik GmbH, Limbach-Oberfrohna, Germany) with a precision of 0.1 cm for body height. In addition to body height seven circumferences were measured for head, neck, upper arm, waist, hip, thigh, and calf ( Table 2 ) according to Lohman (36). Circumferences of arm and leg were each taken on the right side. All measurements were first documented on printed forms and digitized in a second step.
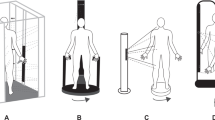
Three-dimensional scans were taken with a Vitus Smart XXL whole body laser scanner. The scanning system emits light using an eye-safe class I laser that is reflected by the scanned object and captured by a camera. With known position of light source and camera a spatial coordinate of the light reflecting point can be calculated by optical triangulation (12). The single measurement points form the three-dimensional virtual model of the scanned object. The Vitus Smart XXL consists of a platform with integrated scales surrounded by four columns with four laser sources and eight cameras driven by a pc-connected control unit. The laser grid is projected as a horizontal band and moves vertically along the body. One scan is completed in about 10 s with a precision of 0.1 cm reported by the manufacturer. Dark curtains around the scanning setup prevent disturbance by external light. All subjects were scanned three consecutive times leaving and re-entering the scan area between each scan. They wear tight underwear and a swim cap to minimize scan errors due to clothing and hairstyle and take an upright posture with the head straight ahead, arms angled away from the body, elbows slightly bent, clenched hands and feet placed shoulder-wide apart as recommended by Human Solutions (Figure 4). The proprietary software AnthroScan Professional (version 2.9.9.b, Human Solutions, Kaiserslautern, Germany) calculates more than 160 anthropometric values out of a single scan. These data are digitally imported to the research database. A detailed documentation of the calculation process is not available but the manufacturer stated standardization according to DIN EN ISO 20685. There are several alternative definitions for neck, waist, and hip circumference implemented in the body scanner measurement protocol. Therefore, a total of 24 measurements of the body scanner were analyzed in comparison to the eight measurements of conventional anthropometry ( Table 2 ).
Statistical Analysis
All calculations were performed with Microsoft Excel (version 16.0.6366.2036, Microsoft, Redmond, Washington) and the statistical software R (version 3.3.1, R core team, Vienna, Austria). For visual data analysis Bland-Altman plots basing on the mean of each measurement triplet were used. Outliers in these plots were double-checked and transfer errors between form and database were corrected. The validity of the body scanner was evaluated by concordance correlation coefficients (CCC) calculation between corresponding measurements of conventional anthropometry and body scanner with averaged measurement triplets as recommended in (27). To assess the intraobserver reliability of both techniques we calculated overall CCC (OCCC) between the three single measurements of each measurement triplet. The CCC by Lin (37) describes the agreement of measurements, where +1 is defined as perfect agreement. The OCCC as a natural generalization of the CCC is designed for examination protocols with more than two observations (38). The chosen strength-of-agreement categories are orientated to the Pearson product-moment correlation coefficient: CCC ≥ 0.9 (“excellent”); < 0.9 and ≥ 0.7 (“good”); < 0.7 and ≥ 0.5 (“moderate”); and < 0.5 (“low”). Differences of CCC between independent groups were tested for significance by an unpaired two-sample t-test. Therefore, we used Fisher-transformed CCC as means and estimated jackknife standard errors of Fisher-transformed CCC for variance estimation. The complete dataset with all results is available as an online supplement (see Supplementary Table S9 online).
To improve concordance between body scanner and conventional anthropometry, we established an offset correction technique to neutralize systematic errors of the body scanner. We calculated the differences between the means of corresponding measurement triplets and averaged these differences for each measurement and subgroup separately (offset correction). The CCC calculation was repeated with the offset-corrected body scanner measurements. We did not derive universal correction factors out of this data.
Results
Body Scanner Validity
We calculated CCC (37) between averaged measurement triplets of corresponding conventional and body scanner measurements. Figure 1 displays CCC for assessment of agreement between both techniques for the complete study population (n = 473). Body height, all hip circumferences (hip girth, buttock girth, high hip girth, and middle hip), upper arm girth, calf girth, and the waist circumferences high waist girth and waist girth reached an “excellent” (CCC ≥ 0.9) degree of agreement between conventional and body scanner measurements. Mid neck girth, the waist circumferences max belly circumference, belly circumference, 3d waistband, and waistband as well as thigh girth had a “good” (CCC ≥ 0.7) level of agreement. Head circumference and neck at base girth were in the “low” (CCC < 0.5) concordance category.

Body scanner validity. CCC (x-axis) between corresponding measurements of body scanner (y-axis) and conventional anthropometry (right side, measurement triplets averaged) for the undivided study population (n = 473). Dashed lines indicate the concordance categories (CCC ≥ 0.9 “excellent”; ≥ 0.7, < 0.9 “good”; ≥ 0.5, < 0.7 “moderate” and < 0.5 “low”).
In case of multiple measurement definitions for one anatomic region we selected those with the highest degree of agreement regarding to the whole study population (n = 473) as displayed in Figure 1 . This way each conventional measurement was assigned to a single body scanner measurement. Figure 2 shows CCC for selected measurements of the study population subdivided into groups of weight, age, and sex. Since the subgroup of underweight participants is rather small (n = 26), we refrained from further dividing. All results with and without offset correction are available as supplement (Supplementary Tables S1–S8 online). We used not offset-corrected data for further analysis.

Body scanner validity. CCC (y-axis) between corresponding measurements of body scanner and conventional anthropometry (y-facets, measurement triplets averaged) with the study population divided into subgroups of age (x-axis), weight (x-facets) and sex (shape). Offset correction is shown by the one-sided error-bars. The underweight subgroup is not divided into age and sex due to the small number of participants. Figure key: dot - male and female, triangle - male, square - female.
Body Height A total CCC of 0.998 for the whole population and a range between 0.987 (male, normal weight, 14–17 y old) and 0.997 (male, normal weight, 10–13) were observed for body height without major influence of age, weight or sex.
Head Head circumference showed a CCC of 0.386 for the complete population and a range between 0.088 (female, overweight, 6–9) and 0.473 (male, overweight, 14–17). Concordance for females was smaller (0.316) than for male participants (0.515, P < 0.0001).
Neck We chose the mid neck girth with a total CCC of 0.877, ranging from 0.439 (female, normal weight, 6–9) up to 0.885 (female, overweight, 14–17) with a dependency on weight: 0.788 for underweight, 0.874 for normal weight (vs. underweight P < 0.0001), and 0.734 for overweight participants (vs. underweight P = 0.0007 and vs. normal weight P < 0.0001). Furthermore, there was a trend toward higher degree of agreement with increasing age: 0.810 (6–9) and 0.806 (10–13) against 0.922 (14–17, vs. 6–9 and 10–13 P < 0.0001).
Waist High waist girth showed the best agreement with a CCC of 0.981 for the whole study population, a range from 0.823 (male, normal weight, 6–9) up to 0.966 (female, overweight, 14–17) and a dependency on weight: from 0.829 for underweight to 0.942 for normal weight (vs. underweight P < 0.0001) and 0.958 for overweight participants (vs. underweight and normal weight P < 0.0001).
Hip Buttock girth was the best fitting measurement among hip circumferences with a total CCC of 0.982, 0.621 (male, normal weight, 14–17) at the lower and 0.976 (female, overweight, 10–13) at the upper end.
Arm The upper arm girth had a CCC of 0.944 over the whole study population with a range from 0.529 (female, overweight, 6–9) to 0.899 (female, overweight, 10–13). The CCC showed dependencies on weight: 0.787 for underweight, 0.907 for normal weight (vs. underweight P < 0.0001), and 0.850 for overweight participants (vs. underweight and normal weight P < 0.0001). Furthermore, the CCC of the 10- to 13-y-old participants (0.959) was higher than in the age groups from 6 to 9 (0.909, vs. 10–13 P < 0.0001) and 14–17 (0.885, vs. 6–9 and 10–13 P < 0.0001).
Thigh For thigh girth we observed a CCC of 0.879 for the total population, ranging between 0.168 (underweight) to 0.863 (male, overweight, 14–17). Male study participants reached higher CCC (0.938) than female ones (0.824, P < 0.0001). For the normal weight children there was a trend toward lower CCC with increasing age: 0.642 (6–9), 0.512 (10–13, vs. 6–9 P < 0.0001), and 0.385 (14–17, vs. 6–9 and 10–13 P < 0.0001) and vice versa for the overweight participants: 0.464 (6–9), 0.698 (10–13, vs. 6–9 P < 0.0001) and 0.702 (14–17, vs. 6–9 P < 0.0001).
Calf For calf girth a CCC of 0.985 was achieved for the whole study population with a minimum CCC of 0.596 (female, overweight, 6–9) and a maximum of 0.985 (female, overweight, 10–13).
Figure 3 shows a graphical analysis of the data using Bland-Altman plots with averaged measurement triplets. The data were fitted with a linear regression model. Differences between measurements increased with higher values especially for head circumference, mid neck girth, high waist girth, and thigh girth, showing an overestimation of greater m+easurements by the body scanner. Upper arm girth was overestimated for lower and underestimated for higher measurements. For body height, buttock girth, and calf girth the differences were barely influenced by the measurement value with an underestimation of body height and an overestimation of buttock girth by the body scanner.

Bland-Altman plots of conventional anthropometry and body scanner measurements. Plots basing on means of each measurement triplet for body height (a), head circumference (b), mid neck (c), high waist (d), buttock (e), upper arm (f), thigh (g) and calf girth (h). The data are fitted with a linear regression model (grey line). Axes are scaled independently for each plot.
Offset Correction
The offset correction improved the degree of concordance especially for the head circumference, mid neck girth, and thigh girth ( Figure 2 , Supplementary Tables S5–S8 online). Compared with the raw data, the lowest degree of concordance for head circumference was changed from 0.088 to 0.282 (female, overweight, 6–9) and over the complete population from 0.386 to 0.734 with major improvements in all subgroups. For mid neck girth the offset correction flattened the concordance differences between the age categories. The 6- to 9-y old normal weight participants increased from 0.563 to 0.803 and the same-aged overweight subgroup from 0.603 to 0.855. Concordances of the overweight 10- to 13-y-olds changed from 0.562 to 0.771. For thigh girth we observed major improvements within the normal weight participants, e.g., for the normal weight, 14- to 17-y-old females from 0.332 to 0.891. The lowest CCC improved from 0.168 to 0.270 (underweight) and over all participants from 0.879 to 0.950.
Intraobserver Reliability
We calculated OCCC (38) between single measurements of each measurement triplet, displayed in Table 2 .
Discussion
In this study, we investigated the feasibility of using three-dimensional whole body laser scanning to gather anthropometric data from children and adolescents in comparison to conventional anthropometry considered as standard in epidemiologic research.
The interpretation of CCC and OCCC in this study is oriented on the conventional correlation coefficient. Choosing another classification, validity categories will change, e.g., according to McBride (39). Due to our moderate study population size, subgroup-analysis is partly hampered by small sample sizes. Accordingly, we expected to see wide ranged confidence intervals for normal weight and overweight 14- to 17-y-old males (n = 23 and 21 respectively) and for overweight 6- to 9-y-old females (n = 21) and can confirm this especially for mid neck girth, upper arm girth, thigh girth, and calf girth. Hence, estimated concordances of our subgroup analyses should be considered with caution. Observed trends in respect of age, sex, and weight require confirmation in a larger study.
Body height, waist, and hip circumference as well as calf girth can be determined with high validity and without remarkable influence of age, sex or weight. Other measurements have to be considered more carefully, e.g., the head circumference. Measuring the head circumference with a tape measure, hair can be compressed. The body scanner as a noncontact measuring system can only detect the shape of the head including hair style. Although the participants wear swim caps to minimize these measurement errors, volume of hair cannot completely be neutralized. Therefore, the validity of measurement is higher for male participants, having more often short hair with less volume. The lower agreement for circumferences of upper arm and thigh can be explained in a similar way. Despite the laser grid is projected from four points, tissue shadowing cannot be prevented completely as illustrated by the black areas in Figure 4b (arrow). Using a tape measure, limb circumferences can be gathered easily at any desired point. In contrast, contact of upper arms to the thorax or close contact between the thighs cause problems for the body scanner assessment. The Vitus Smart XXL requires axilla and thigh gap for correct detection of measurement points. Tissue contact complicating the detection of these landmarks should be prevented as far as possible by the standard scanning posture, which was difficult to ensure for younger or obese children. Therefore, we expected to see a trend toward lower degree of agreement with increasing weight for these measurements. Actually, the lowest degrees of concordance were achieved for the underweights. For thigh girth we observed a higher degree of agreement for male participants. This trend could be explained by a different distribution of fat tissue between male (abdominal) and female (hip and thigh). Nevertheless, thigh and calf girth were measured with a “good” respectively “excellent” degree of concordance over the complete study population. Young participants sometimes showed to be unable to keep the scanning posture correctly or were easily distracted by external factors as presence of parents and siblings or fascination for the scanning device. Therefore, we expected to see less valid measurements with decreasing age, which we can confirm for neck circumference as well as partly waist and hip circumference. In addition, neck circumference was less valid for overweight participants. Eventually the body scanner is simply searching for the widest girth at the neck and with increasing fat tissue this circumference departs more and more from the anatomic landmarks of the conventional anthropometry. The described trend of higher validity with increasing age was reversed for thigh girth. One possible explanation is an age-dependent change in the distribution of muscle and fat tissue causing shadowing of measurement landmarks as mentioned above. These findings are in accordance to other studies, describing measurement differences between the technologies (28).

Scan images. Three-dimensional image of a normal weight (a) and an overweight boy (b). Standard scanning posture. Lines indicate the location of measurements. Note the black areas of missing data due to tissue shadowing, especially at axilla, inside arm (arrow) and thigh.
The linear regression models in Figure 3 show changes of measurement differences in relation to the extent of single measurements and partly trends to over- or underestimation by the body scanner. Wells et al. (29) stated a tendency to greater measurements by the scanner compared with manual techniques but using structured light. Measuring body height with the scanner, participants stand with feet placed shoulder-wide apart whereas for the conventional anthropometry the feet have to be next to each other. Therefore, we expected underestimated body scanner measurements, which we can confirm. Circumferences of the trunk are strictly measured in the horizontal plane by the scanner. This can be difficult to ensure for the conventional anthropometry, especially for young or obese children. Measuring in an inclined plane can cause a bias, too. All outliers in the plots of Figure 3 were double-checked with the handwritten forms of the conventional anthropometry. Identified transfer errors were corrected but we did not exclude any measurements.
Using the offset correction, we were able to improve the degree of concordance in different extents depending on the particular measurement. Major improvements were achieved for head circumference, thigh girth, and partly mid neck girth, showing the measurement errors to be at least partial systematically. Other measurements were either already on a high degree of concordance (e.g., body height, high waist girth, and buttock girth) or just profited less from the offset correction (e.g., upper arm girth or calf and thigh girth for 6- to 9-y-old overweight females). Therefore, we can suppose a smaller systematic component in measurement errors or our subgroup was too small to identify a bias. To confirm observed trends and deduce general correction values for single measurements, results have to be verified with larger subgroups.
We expected a trend toward more reproducible results of the body scanner due to its higher grade of automation compared with the conventional anthropometry. Our results show that intraobserver reliability of body scanner and conventional anthropometry are comparable. There is an outlier among the body scanner measurements we did not choose for comparison. Neck at base girth (OCCC 0.237) reached the “low” concordance category in the intraobserver analysis. Some of the anatomic landmarks are apparently hard to identify for the software. It has to be considered, that the high intraobserver reliability of the conventional anthropometry could be caused by a recall bias which is not possible for the body scanner. High reproducibility was also reported for other scanning systems (26,31).
Three-dimensional whole body laser scanning is a very efficient way to acquire anthropometrical data fast and easy, store it for a long time and extract additional measurements out of the stored data at any time. Another main advantage of body scanning is the possibility to directly take measurements that can only be estimated by conventional anthropometry, e.g., body surface area or body volume. Measuring is faster due to the high grade of automation of scanning. Nevertheless, staff training is still required and should be repeated regularly to guarantee correct guidance of scanned persons. Beside this, there is no need for a manual transfer of any data to digital forms and databases or to use handwritten documentation. A major drawback is the inaccessibility of any technical documentation regarding the scanning procedure in detail. Therefore, the origin of many measurements can only be presumed. This way it is difficult to identify and explain distinct factors influencing the quality and validity of scanning. With its origin in fashion and apparel industries, the body scanner and its software are not optimized for children yet. Nevertheless, most of the body scanner measurements showed an “excellent” concordance but some has to be chosen carefully, e.g., mid neck girth and thigh girth. We cannot recommend using head circumference as measured by the body scanner for medical applications. Considering this, three-dimensional whole body laser scanning is a well-suited tool for epidemiologic settings and can complement or in some applications even replace conventional anthropometry.
Limitations
The subgroups of the study population are not equal and the underweight participants were not further divided. Comparison of these groups has to be done carefully.
The assessments were performed by several observers. Reliability analysis was done within the three measurements of one observer (intrarater), not between observers (inter-rater). Therefore, we cannot completely exclude measurement deviations between observers.
Statement of Financial Support
This publication is supported by LIFE - Leipzig Research Centre for Civilization Diseases. LIFE is supported by financial means of the European Union, by the European Regional Development Fund (ERDF) and by funds of the Free State of Saxony in the context of the excellence initiative.
Disclosure
The authors declare that there are no conflicts of interest.
References
Keys A, Fidanza F, Karvonen MJ, Kimura N, Taylor HL. Indices of relative weight and obesity. J Chronic Dis 1972;25:329–43.
Taylor RW, Jones IE, Williams SM, Goulding A. Evaluation of waist circumference, waist-to-hip ratio, and the conicity index as screening tools for high trunk fat mass, as measured by dual-energy X-ray absorptiometry, in children aged 3-19 y. Am J Clin Nutr 2000;72:490–5.
Hatipoglu N, Mazicioglu MM, Kurtoglu S, Kendirci M. Neck circumference: an additional tool of screening overweight and obesity in childhood. Eur J Pediatr 2010;169:733–9.
Kleiser C, Schienkiewitz A, Schaffrath Rosario A, Prinz-Langenohl R, Scheidt-Nave C, Mensink GB. Indicators of overweight and cardiovascular disease risk factors among 11- to 17-year-old boys and girls in Germany. Obes Facts 2011;4:379–85.
Kahn HS, Imperatore G, Cheng YJ. A population-based comparison of BMI percentiles and waist-to-height ratio for identifying cardiovascular risk in youth. J Pediatr 2005;146:482–8.
Nagy E, Vicente-Rodriguez G, Manios Y, et al. Harmonization process and reliability assessment of anthropometric measurements in a multicenter study in adolescents. Int J Obes (Lond) 2008;32 Suppl 5:65.
Padela AI, Rodriguez del Pozo P. Muslim patients and cross-gender interactions in medicine: an Islamic bioethical perspective. J Med Ethics 2011;37:40–4.
Jones PR, West GM, Harris DH, Read JB. The Loughborough anthropometric shadow scanner (LASS). Endeavour 1989;13:162–8.
Burke PH, Beard L. Stereophotogrammetry of the face. Am J Orthod 1967;53:769–82.
Rodríguez-Quiñonez JC, Sergiyenko O, Tyrsa V, et al. 3D body & medical scanners’ technologies: methodology and spatial discriminations. In: Sergiyenko O, ed. Optoelectronic Devices and Properties. Rijeka: INTECH Open Access Publisher, 2011.
Kau CH, Richmond S, Incrapera A, English J, Xia JJ. Three-dimensional surface acquisition systems for the study of facial morphology and their application to maxillofacial surgery. Int J Med Robot 2007;3:97–110.
Eder M, Brockmann G, Zimmermann A, et al. Evaluation of precision and accuracy assessment of different 3-D surface imaging systems for biomedical purposes. J Digit Imaging 2013;26:163–72.
Simmons KP, Istook CL. Body measurement techniques: comparing 3D body-scanning and anthropometric methods for apparel applications. J Fash Mark Manag 2003;7:306–32.
Kus A, Unver E, Taylor A. A comparative study of 3D scanning in engineering, product and transport design and fashion design education. Comput Appl Eng Educ 2009;17:263–71.
Zwane PE, Sithole M, Hunter L. A preliminary comparative analysis of 3D body scanner, manually taken girth body measurements and size chart measurements. Int J Consum Stud 2010;34:265–71.
Losken A, Fishman I, Denson DD, Moyer HR, Carlson GW. An objective evaluation of breast symmetry and shape differences using 3-dimensional images. Ann Plast Surg 2005;55:571–5.
Losken A, Seify H, Denson DD, Paredes AA Jr, Carlson GW. Validating three-dimensional imaging of the breast. Ann Plast Surg 2005;54:471–6; discussion 477–8.
Moyer HR, Carlson GW, Styblo TM, Losken A. Three-dimensional digital evaluation of breast symmetry after breast conservation therapy. J Am Coll Surg 2008;207:227–32.
Gaisberger C, Steininger P, Mitterlechner B, et al. Three-dimensional surface scanning for accurate patient positioning and monitoring during breast cancer radiotherapy. Strahlenther Onkol 2013;189:887–93.
Aldridge K, George ID, Cole KK, et al. Facial phenotypes in subgroups of prepubertal boys with autism spectrum disorders are correlated with clinical phenotypes. Mol Autism 2011;2:15.
Verzé L, Nasi A, Quaranta F, Vasino V, Prini V, Ramieri G. Quantification of facial movements by surface laser scanning. J Craniofac Surg 2011;22:60–5.
Thompson JT, David LR, Wood B, Argenta A, Simpson J, Argenta LC. Outcome analysis of helmet therapy for positional plagiocephaly using a three-dimensional surface scanning laser. J Craniofac Surg 2009;20:362–5.
Daniell N, Olds T, Tomkinson G. Technical note: Criterion validity of whole body surface area equations: a comparison using 3D laser scanning. Am J Phys Anthropol 2012;148:148–55.
Weinberg SM, Naidoo S, Govier DP, Martin RA, Kane AA, Marazita ML. Anthropometric precision and accuracy of digital three-dimensional photogrammetry: comparing the Genex and 3dMD imaging systems with one another and with direct anthropometry. J Craniofac Surg 2006;17:477–83.
Lee J, Kawale M, Merchant FA, et al. Validation of stereophotogrammetry of the human torso. Breast Cancer (Auckl) 2011;5:15–25.
Bretschneider T, Koop U, Schreiner V, Wenck H, Jaspers S. Validation of the body scanner as a measuring tool for a rapid quantification of body shape. Skin Res Technol 2009;15:364–9.
Kuehnapfel A, Ahnert P, Loeffler M, Broda A, Scholz M. Reliability of 3D laser-based anthropometry and comparison with classical anthropometry. Sci Rep 2016;6:26672.
Heuberger R, Domina T, MacGillivray M. Body scanning as a new anthropometric measurement tool for health-risk assessment. Int J Consum Stud 2008;32:34–40.
Wells JC, Stocks J, Bonner R, et al. Acceptability, precision and accuracy of 3D photonic scanning for measurement of body shape in a multi-ethnic sample of children aged 5-11 years: The SLIC Study. PLoS One 2015;10:e0124193.
Gorton GE 3rd, Young ML, Masso PD. Accuracy, reliability, and validity of a 3-dimensional scanner for assessing torso shape in idiopathic scoliosis. Spine (Phila Pa 1976) 2012;37:957–65.
Kau CH, Zhurov A, Scheer R, Bouwman S, Richmond S. The feasibility of measuring three-dimensional facial morphology in children. Orthod Craniofac Res 2004;7:198–204.
Quante M, Hesse M, Döhnert M, et al.; LIFE Child Study Investigators. The LIFE child study: a life course approach to disease and health. BMC Public Health 2012;12:1021.
Wabitsch M, Kunze D, Moß A. Konsensbasierte (S2) Leitlinie zur Diagnostik, Therapie und Prävention von Übergewicht und Adipositas im Kindes- und Jugendalter. http://www.aga.adipositas-gesellschaft.de/fileadmin/PDF/Leitlinien/AGA_S2_Leitlinie.pdf. Accessed 21 September 2016.
Vogel M. Calculation of standard deviation scores adduced from different growth standards. R package version 0.5., 2014. http://CRAN.R-project.org/package=childsds.
Kromeyer-Hauschild K, Wabitsch M, Kunze D, et al. Perzentile für den Body-mass-Index für das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben. Monatsschr Kinderheilkd 2001;149:807–18.
Lohman TG, ed. Anthropometric Standardization Reference Manual. Champaign IL: Human Kinetics Books, 1988.
Lin LI. A concordance correlation coefficient to evaluate reproducibility. Biometrics 1989;45:255–68.
Barnhart HX, Haber M, Song J. Overall concordance correlation coefficient for evaluating agreement among multiple observers. Biometrics 2002;58:1020–7.
McBride GB. A proposal for strength-of-agreement criteria for Lin’s Concordance Correlation Coefficient. NIWA Client Report: HAM2005-062 2005;(HAM2005-062).
Author information
Authors and Affiliations
Corresponding author
Supplementary information
Supplementary Tables
(ZIP 329 kb)
Rights and permissions
About this article

Cite this article
Glock, F., Vogel, M., Naumann, S. et al. Validity and intraobserver reliability of three-dimensional scanning compared with conventional anthropometry for children and adolescents from a population-based cohort study. Pediatr Res 81, 736–744 (2017). https://doi.org/10.1038/pr.2016.274
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2016.274
This article is cited by
-
The smart body concept as a demonstration of the overarching utility and benefits of 3D avatars in retail, health and wellbeing: an accuracy study of body measures from 3D reconstruction
Multimedia Tools and Applications (2023)
-
The aging human body shape
npj Aging and Mechanisms of Disease (2020)
-
Validity and reliability of three-dimensional scanning compared to conventional anthropometry for children and adolescents: methodological mistake
Pediatric Research (2017)
-
Response to Sabour
Pediatric Research (2017)
