
Abstract
Maternal milk plays an important role in breast milk jaundice (BMJ) development and is the major source of epidermal growth factor (EGF) for neonates. The aim of this study was to investigate whether there is a relationship between EGF levels in the infant serum and in the milk of nursing mothers and BMJ. Two groups were defined: study group (n = 30), newborns who were followed up for BMJ without any identifiable pathologic cause; control group, healthy newborns whose serum total bilirubin levels were <10 mg/dL. Milk and infant plasma samples were collected between the third and the fourth postpartum week. EGF concentrations in all of the samples were determined by using ELISA. The infants with BMJ had higher concentrations of EGF in the serum and in the breast milk compared with that of the infants without BMJ. The milk concentrations of EGF were significantly correlated with neonatal bilirubin and blood EGF concentrations. The degree of BMJ was associated with the increased levels of milk borne EGF. Although the exact mechanisms of the hyperbilirubinemic action of EGF are not completely known, the inhibition of gastric motility, increased absorption, and activation of bilirubin transport have been suggested as possible mechanisms.
Similar content being viewed by others

Main
Late onset breast milk jaundice (BMJ), also called BMJ syndrome, after the fifth day, a majority of breastfed infants either maintain a stable, but elevated serum bilirubin level, or have a second rise in bilirubin, which generally peaks on approximately 10th to 15th days of life. In some infants, these elevated levels may continue for many weeks, whereas in others, the levels decline during the third and fourth weeks. During the third week of life, among the two thirds or more with elevated levels, 2 to 4% of infants have a bilirubin level >10 mg/dL (170 mM) at 3 wks of age. Rarely do the levels in healthy term infants rise beyond 25 mg/dL (425 mM) or place the infant at risk for bilirubin encephalopathy. Ultimately, serum bilirubin levels return to normal in all infants with BMJ. Persistence of hyperbilirubinemia beyond 3 mo would suggest an etiology other than breast milk. The jaundice of breastfed infants is commonly of undetermined etiology (1–11). As reviewed elsewhere (12), many pathophysiologic theories have arisen to explain this prolonged nonconjugated hyperbilirubinemia associated with human milk feedings in otherwise healthy infants. The most attractive and convincing evidence regarding the mechanism of BMJ has come from studies of the effect of human milk on the intestinal absorption of bilirubin with resultant increase in enterohepatic circulation of bilirubin. Milk from mothers of infants with classical BMJ inhibited intestinal absorption of bilirubin only for the first 2 h and was then followed by a dramatic increase in absorption, which continued for at least an additional 14 h and resulted in a total absorption of 60% of the intestinal bilirubin dose. A subsequent study by other investigators confirmed the role of human milk enhancement of intestinal bilirubin absorption and demonstrated a significant positive correlation between the degree of enhancement of bilirubin absorption in the rat model by the human mother's milk and the infant's serum bilirubin elevation (13). The factor in human milk that increases intestinal bilirubin absorption remains unidentified. BMJ does not present in the first 5 d of life, apparently because the factor in human milk inducing an increase in intestinal absorption of bilirubin does not appear until the transition from colostrum to mature milk (14).
The gastrointestinal tract undergoes substantial changes during the early postnatal period. Profound growth, morphologic changes, and functional maturation of the small intestine are observed during this developmental period. The introduction of enteral nutrition initiates significant changes in mucosal structure and function required for the utilization of milk. Most of these changes are concluded by the weaning phase when the transition from milk to solid food occurs. Physiologic changes in digestive and absorptive processes are well described (15), but the understanding of the mechanisms by which intestinal growth and epithelial turnover are regulated remains fragmentary. However, it is clear that biologically active peptides such as hormones and growth factors are essential parts of this regulatory system. It is well established that breast milk contains large numbers of biologically active substances. In vivo and in vitro studies showed that human milk stimulates intestinal development, DNA synthesis, and cell proliferation. Two growth-stimulating peptides that are believed to play an important role in this process are epidermal growth factor (EGF) and transforming growth factor-α (16). EGF, an acid polypeptide of 53 amino acids with three disulfide bonds, has been believed to be the main mitogen in human milk that stimulates cell division (17). Because EGF is detected in several mammalian milks, questions have been raised about its functional significance in milk. Previous studies demonstrated the presence of EGF in the developing gut of suckling rats and showed that intestinal EGF levels are predominantly related to the intake of milk-borne EGF. The concentration of EGF was highest in colostrum and gradually decreases in mature milk to a concentration of approximately 5.0-6.7 nmol/L (18–21). On the other hand, there is a positive correlation between salivary EGF (sEGF) levels and gestational age. Patterns of sEGF levels during the first 2 wks of life were significantly related to the development of necrotizing enterocolitis in very low birth weight infants. Saliva was sampled for EGF measurement because of the importance sEGF has to intestinal integrity and development as well as the close correlation between serum EGF and sEGF values demonstrated in earlier work. Saliva is increasingly being used as a noninvasive sampling source in the pediatric populations, including preterm infants (22,23). EGF may regulate intestinal growth through the EGF receptor on the basolateral membrane. The evidence suggests that EGF in human milk plays an important role in fetal or postnatal intestinal growth and development (24). Our hypothesis is that milk borne of EGF may increase the development and incidence of BMJ.
The objective of the present study was to investigate whether there is a relationship between EGF levels in the mature milk of nursing mothers and BMJ, with the consequent implications on the development of neonatal hyperbilirubinemia.
MATERIALS AND METHODS
Patients.
This prospective study was performed between January 2007 and June 2008 in the Dokuz Eylul University Hospital Departments of Neonatology. In total, 60 infants were admitted to this study. Study protocol was approved by the Dokuz Eylul University Faculty of Medicine Human Clinical Investigation Committee, and informed consent was obtained from the parents of all infants for their child's blood sampling.
All cases were diagnosed during the third to fourth week of life when the parents visited our office concerned about the prolonged jaundice. We analyzed 30 infants who developed prolonged apparent jaundice (begins after 5-7 d of life, peaks around the 10th d or later of life, rule out other causes of prolonged jaundice, serum bilirubin levels return to normal before 3 mo) and had total serum bilirubin concentrations above 171 mM (10 mg/dL) after the third week of life. Sample collection date and time were recorded, as were infants' birth date, gestational age, birth weight, sex, mothers' demographic and anthropometrical characteristics (age, parity, body mass index), and race and route of delivery (cesarean section versus vaginal). Infants who had known risk factors, such as blood group incompatibilities, positive Coombs' test, glucose-6-phosphate dehydrogenase deficiency (measured on all newborns with nonphysiologic jaundice in this hospital), any laboratory evidence of hemolytic disease as evidenced by anemia, reticulocytosis or abnormality of the blood smear, perinatal factors associated with an increased risk of hyperbilirubinemia, including maternal diabetes mellitus, polycytemia, cephalohematoma, asphyxia, hypothermia, intracranial hemorrhage, perinatal infection, or dehydration (defined as >10% weight loss and/or hypernatremia) were excluded. Thirty of the 60 infants (study group) had unexplained prolonged indirect hyperbilirubinemia; they had none of the above-mentioned risk factors, and they were also evaluated for metabolic diseases and hypothyroidism. All the infants were nursed with full breast milk feeding (or fully breast milk fed: the infant receives expressed breast milk in addition to breastfeeding). The remaining 30 infants (control groups) were healthy neonates who were born in our hospital and had no clinical jaundice during their follow-up period. None of the children in the study group or in the control group had a history of any important medical problem that developed in the postneonatal period.
Infant serum samples.
Blood sample for EGF measurement in the study group was obtained when blood was drawn from the infant for other tests necessary for evaluating the cause of jaundice. Control groups were convenience sample of infants of similar age (between 3 and 4 wks) who required admission to our neonatology unit for health control or other reasons, such as phenylketonuria screening. Infant serum samples were collected in sterile tubes, placed on ice, and immediately sent to the laboratory. After centrifugation of blood at 3000 × g for 30 min at 4°C, the plasma supernatant fluid was separated and stored at −80°C until analyzed further (25).
Human milk samples.
Breast milk samples were collected between the third and the fourth postpartum week. Collection was standardized to reduce bias and potential diurnal variability in EGF measurements. While blood samples for serum bilirubin studies were routinely obtained at 0700 and 1600 h and milk specimens were obtained from the two groups within 1 h of the first feeding in the morning, defined between 0800 and 0900 h, respectively. All mothers were able to provide milk at each sampling point. An aliquot of 5 mL was taken using a manual breast pump (Avent, Suffolk, UK). Human milk samples were collected in sterile tubes, placed on ice, and immediately sent to the laboratory. Samples were centrifuged at 3.750 × g for 2 min to remove fat and cell debris. Supernatant aliquots of 1.5 mL were stored at −80°C for EGF analysis (26).
Measurement of EGF in human milk and blood.
Sixty milk samples were diluted to 1:400. EGF measurements in human milk and infant serum were obtained using an ELISA kit (Biosource International Inc., Belgium). Diluted milk and infant serum samples (200 μL) were incubated with human monoclonal EGF antibody coated on a 96-well plate at room temperature for 2 h. After several washes, polyclonal EGF antibody conjugated to horseradish peroxidase (200 μL) was added to the plate and reacted for 1 h. Samples were then incubated with 200 μL substrates (tetramethylbenzidine:H2O2 = 1:1) for 20 min after several washes. The reaction was terminated with 50 μL sulfuric acid (1 mol/L). EGF concentrations were determined at 450 nm and corrected at 540 nm using an ELISA reader (Multiskan RC; Labsystems, Helsinki, Finland) (26).
Statistical analysis.
Mean weight and gestational age of the groups were compared with one-way analysis of variance. Mann-Whitney U tests were used to determine whether there was a difference in mean serum total bilirubin, blood EGF levels, and milk EGF levels. A p value <0.05 was accepted as statistically significant. Linear regression analysis was used to evaluate the relationship between elevated milk EGF levels or blood EGF levels and peak bilirubin level.
RESULTS
The infants in the two groups, the control and the study, were compared according to their anthropometrical, clinical, and peripartal characteristics (Table 1). Of the 30 jaundiced infants in the study group, 13 (43.3%) were girls and 17 (56.7%) were boys. The mean gestational age and weight of neonates in the study group were 40 ± 0.9 wk and 3008 ± 325 g, respectively. Their mean bilirubin level was 15.01 ± 2 mg/dL. When breastfeeding was resumed, serum bilirubin concentrations were increased in some infants, but the concentrations decreased to within normal range (8.55-12.2 mM), or jaundice disappeared visually for all infants by 4 mo of age. In control group, 12 (40%) were boys and 18 (60%) were girls. The mean gestational age and weight of neonates in the control group were 39 ± 1.6 wk and 3168 ± 298 g, respectively, and their mean total serum bilirubin level was 5.9 ± 1.6 mg/dL. Infants in both groups (study group, n = 30, and control group, n = 30) were similar with respect to gender, route of delivery, mean birth weight, gestational age, and age at the time of the study (Table 1).
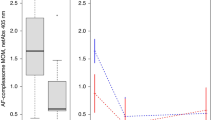
Serum and milk EGF levels of the study group were higher than the control groups (Table 2). There was a positive relationship between serum total bilirubin levels and milk and blood EGF levels in the study group (t = 4.08, p = 0.001, Fig. 1 and t = 3.39, p = 0.002, Fig. 2). In addition, there was a positive relationship between milk and infant serum EGF levels (t = 3.37, p = 0.002, Fig. 3).

Positive relationship between serum total bilirubin levels and serum EGF levels in the study group (R2 linear = 0.373).

Positive relationship between serum total bilirubin levels and milk EGF levels in the study group (R2 linear = 0.291).

Positive relationship between milk and infant serum EGF levels in the study group (R2 linear = 0.289).
DISCUSSION
In this study, we present novel evidence suggesting that the mammary glands' growth function, significantly influencing milk provision of the EGF for breastfeeding, may affect jaundice development in neonates. To clarify the role of growth factors in human milk in the gastrointestinal adaptation of the fetus and newborn, effects of these fluids and multiple growth factors were investigated in a human fetal small intestinal cell line (22). Breastfed infants have higher bilirubin levels than formula-fed infants, possibly because of variations in the composition of the breast milk. Interestingly, in our study, the degree of BMJ was associated with the increased levels of milk-borne EGF.
Human milk is an important source of bioactive substances including hormones, growth factors, and immunologic factors such as cytokines, but the functional consequences of an overexpression or a down-regulation of most milk, immunomodulatory constituents in neonates are largely unknown. EGF is known to play a critical role in the intestinal absorption. The ability of mammary secretions (especially colostrum) to stimulate the growth of cells in culture is unequivocal (27,28). However, for milk-borne growth factors to elicit trophic effects on the intestine of the suckling neonate, they must survive the digestive process and arrive in sufficient concentration to bind to their intestinal receptors and thereby stimulate cell growth and/or differentiation. EGF is acid stable and trypsin resistant, allowing it to survive passage through the gastrointestinal tract and to act directly on the intestinal cells (29). The predominant effects of EGF on the gastrointestinal tract have been reported and include suppression of gastric acid secretion, gastric cytoprotection; stimulation of intestinal DNA synthesis, and cell division; regulation of intestinal brush-border disaccharidase activities; increased water, glucose, and sodium absorption; increased cellular calcium concentration; activation of ion transport; and modulation of prostaglandin synthesis and secretion (30,31). Our study suggests that EGF plays an important role in BMJ. Results from this study support this hypothesis and the critical role of milk-borne EGF in the maintenance of intestinal absorption.
Previous studies have shown that orogastrically (32) and/or intestinally administered EGF (33) is absorbed by the gastrointestinal epithelium and transferred via the portal vein into systemic organs. In the present study, we have shown that neonatal serum bilirubin levels are related to human milk EGF levels. Ingestion of human milk containing high EGF levels was associated with higher serum bilirubin in the infant. EGF is present in milk from many mammalian species and the permeability characteristic of the neonatal gut allows the absorption of EGF into the circulation (34). Our data suggest that milk-borne EGF is an important factor for the maintenance of EGF serum levels in the suckling. The differences in EGF serum levels between the experimental groups also suggest the possibility of changes in gastrointestinal motility. Previous study have shown that the parenteral administration of EGF affects gastrointestinal transit in suckling rats (35), subcutaneous injection of EGF significantly delayed gastric emptying, and the changes in stomach evacuation were EGF dose dependent. A similar phenomenon was observed in the small intestine in which the administration of EGF markedly delayed small intestinal transit (35). Although the exact mechanisms of the hyperbilirubinemic action of EGF are not completely known, the inhibition of gastric motility, increased absorption, and activation of bilirubin transport have been suggested as possible mechanisms.
In conclusion, the concentrations of EGF were higher in the breast milk of the mothers whose infants had BMJ. Our hypothesis was that the enteral intake of EGF might increase the development and incidence of BMJ. The degree of BMJ was associated with the increased levels of milk-borne EGF. Better understanding of molecular processes underlying EGF-mediated hyperbilirubinemia might provide the basis for the future therapeutic strategies for the treatment of BMJ.
References
Schneider AP 1986 Breast milk jaundice in the newborn a real entity. JAMA 255: 3270–3274
DeAngelis C, Sargent J, Chun MK 1980 Breast milk jaundice. Wis Med J 79: 40–42
Osborn LM, Reiff MI, Bolus R 1984 Jaundice in the full-term neonate. Pediatrics 73: 520–525
Saigal S, Lunyk O, Bennett KJ, Patterson MC 1982 Serum bilirubin levels in breast- and formula-fed infants in the first 5 days of life. Can Med Assoc J 127: 985–989
Maisels MJ, Gifford K 1986 Normal serum bilirubin levels in the newborn and the effect of breast-feeding. Pediatrics 78: 837–843
Narayanan I, Gupta A, Mandal RN, Chugh RK, Singh S 1987 Infant feeding and early neonatal jaundice. Indian J Pediatr 54: 257–260
Kivlahan C, James EJ 1984 The natural history of neonatal jaundice. Pediatrics 74: 364–370
Stiehm ER, Ryan J 1965 Report of eight cases and effect of breast feeding on incidence and severity of unexplained hyperbilirubinemia. Am J Dis Child 109: 212–216
Gartner LM, Arias IM 1966 Studies of prolonged neonatal jaundice in the breast-fed infant. J Pediatr 68: 54–66
Cole AP, Hargreaves T 1972 Conjugation inhibitors and early neonatal hyperbilirubinaemia. Arch Dis Child 47: 415–418
Arthur LJ, Bevan BR, Holton JB 1966 Neonatal hyperbilirubinemia and breast feeding. Dev Med Child Neurol 8: 279–284
Gourley GR 1998 Pathophysiology of breast-milk jaundice. In: Polin RA, Fox WW (eds) Fetal and Neonatal Physiology, 2nd Ed. WB Saunders Company, Philadelphia pp 1499–1505
Alonso EM, Whitington PF, Whitington SH, Rivard VA, Given G 1991 Enterohepatic circulation of nonconjugated bilirubin in rats fed with human milk. J Pediatr 118: 425–430
Arias IM, Gartner LM, Seifter S, Furman M 1964 Prolonged neonatal uncounjugated hyperbilirubinemia associated with breast feeding and a steroid, pregnane-3a, 20 b-diol, in maternal milk that inhibits glucuronide formation in vitro. J Clin Invest 43: 2037–2047
Koldovsky O Digestive-absorption functions in fetuses, infants, and children. In: Polin RA, Fox WW(eds) Fetal and Neonatal Physiology. WB Saunders, Philadelphia 1401–1418
Polk DB 1998 Epidermal growth factor receptor-stimulated intestinal epithelial cell migration requires phospholipase C activity. Gastroenterology 114: 493–502
Carpenter G, Stoschech CM, Preston YA, De Larco JE 1983 Antibodies to the epidermal growth factor receptor block the biological activities of sarcoma growth factor. Proc Natl Acad Sci USA 80: 5627–5630
Todaro GJ, Fryling C, De Larco JE 1980 Transforming growth factors produced by certain human tumor cells: polypeptides that interact with epidermal growth factor receptors. Proc Natl Acad Sci USA 77: 5258–5262
Rao RK, Thornburg W, Korc M, Matrisian L, Magun BE, Koldovsky O 1986 Processing of epidermal growth factor by suckling and adult rat intestinal cells. Am J Physiol 250: G850–G855
Thompson JF, Van Den Berg M, Stokkers PC 1994 Developmental regulation of epidermal growth factor receptor kinase in rat intestine. Gastroenterology 107: 1278–1287
Toyoda S, Lee PC, Lebenthal E 1986 Interaction of epidermal growth factor with specific binding sites of enterocytes isolated from rat small intestine during development. Biochim Biophys Acta 886: 295–301
Dvorak B, Fituch CC, Williams CS, Hurst NM, Schanler RJ 2004 Concentrations of epidermal growth factor and transforming growth factor-alpha in preterm milk. Adv Exp Med Biol 554: 407–409
Warner BB, Ryan AL, Seeger K, Leonard AC, Erwin CR, Warner BW 2007 Ontogeny of salivary epidermal growth factor and necrotizing enterocolitis. J Pediatr 150: 358–363
Grimes J, Schaudies RP, Davis D, Williams CS, Curry BJ, Walker MD, Koldovsky O 1992 Effect of short-term fasting/refeeding on epidermal growth factor content in the gastrointestinal tract of suckling rats. Proc Soc Exp Biol Med 199: 75–80
Radfar M, Larijani B, Hadjibabaie M, Rajabipour B, Mojtahedi A, Abdollahi M 2005 Effects of pentoxifylline on oxidative stress and levels of EGF and NO in blood of diabetic type-2 patients: a randomized, double-blind placebo-controlled clinical trial. Biomed Pharmacother 59: 302–306
Chang CJ, Chao JC 2002 Effect of human milk and epidermal growth factor on growth of human intestinal Caco-2 cells. J Pediatr Gastroenterol Nutr 34: 394–401
Brown KD, Blakeley DM 1983 Cell growth-promoting activity in mammary secretions of the goat, cow and sheep. Br Vet J 139: 68–78
Cera K, Mahan DC, Simmen FA 1987 In vitro growth promoting activity of porcine mammary secretions: initial characterization and relationship to known peptide growth factors. J Anim Sci 65: 1149–1159
Britton JR, George-Nascimento C, Udall JN, Koldovsky O 1989 Minimal hydrolysis of epidermal growth factor by gastric fluid of preterm infants. Gut 30: 327–332
Berseth CL 1987 Enhancement of intestinal growth in neonatal rats by epidermal growth factor in milk. Am J Physiol 253: G662–G665
Opleta-Madsen K, Meddings JB, Gall DG 1991 Epidermal growth factor and postnatal development of intestinal transport and membrane structure. Pediatr Res 30: 342–350
Thornburg W, Matrisian L, Magun B, Koldovsky O 1984 Gastrointestinal absorption of epidermal growth factor in suckling rats. Am J Physiol 246: G80–G85
Kong WY, Koldovsky O, Rao RK 1992 Appearance of exogenous epidermal growth factor in liver, bile, and intestinal lumen of suckling rats. Gastroenterology 102: 661–667
Herrington MK, Adrian TE 1998 Effects of epidermal growth factor, cholecystokinin, and secretin on growth of the alimentary tract in the neonatal guinea pig. Biol Neonate 73: 129–136
Shinohara H, Williams CS, Yakabe T, Koldovsky O 1996 Epidermal growth factor delays gastric emptying and small intestinal transit in suckling rats. Pediatr Res 39: 281–286
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kumral, A., Ozkan, H., Duman, N. et al. Breast Milk Jaundice Correlates With High Levels of Epidermal Growth Factor. Pediatr Res 66, 218–221 (2009). https://doi.org/10.1203/PDR.0b013e3181ac4a30
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/PDR.0b013e3181ac4a30
This article is cited by
-
Inherited disorders of bilirubin clearance
Pediatric Research (2016)
