
Abstract
Objective:
Low-carbohydrate (L-CHO) diets are often used for weight loss but their effects on cognitive function are not well understood. The present study compared the effects of a L-CHO and high-carbohydrate (H-CHO) weight-loss diet on cognitive function adults.
Design:
Participants were randomized to either a L-CHO (n=22) or H-CHO (n=25) weight-loss diet. Cognitive function was evaluated by four computerized cognitive tasks (Stroop Task, Continuous Performance Task, Word Recall and Wisconsin Card Sorting Task) presented in random order before and at 1, 4, 12 and 24 weeks after the initiation of the L-CHO or H-CHO diet.
Participants:
Forty-seven adults (25 males) with a mean±s.d. age of 47.4±8.7 years and body mass index of 35.3±3.4 kg m−2.
Results:
There were no significant differences in weight loss between groups at any time point. There were significant improvements on color Stroop task accuracy over time in both diet groups (P<0.05), but there were no differences in performance between groups on this or any other cognitive task at any time period.
Conclusion:
These findings suggest that weight loss has neither a positive nor a negative effect on cognitive function and that L-CHO and H-CHO weight-loss diets have similar effects on cognitive performance.
Similar content being viewed by others

Introduction
There is evidence to suggest that certain weight-loss practices (for example, skipping breakfast, restricting intake, self-initiated dieting) and weight loss are associated with impairments in various cognitive processes, including memory, attention and processing speed.1, 2, 3, 4, 5, 6, 7 One study reported slower reaction times to salient food words on a food Stroop task in weight-loss maintainers compared with non-dieting normal weight and obese individuals.8 Reasons for the decrements in cognitive performance during dieting, weight loss or weight maintenance in these studies are not fully understood but may be due to alterations in blood glucose levels (as a result of skipping meals, restrictions in food intake), preoccupying thoughts of food and weight and emotional reactivity to salient cues. Despite these findings, minimal to no cognitive impairment9, 10, 11 and improvements in executive/attention functioning and memory12, 13 have been observed in other studies investigating the effects of weight loss on cognitive function.
Research over the last decade suggests that low-carbohydrate (L-CHO) diets are a viable option in the treatment of obesity.14, 15, 16 Although the effects of these diets on weight and cardiovascular disease risk factors are well described, less is known about secondary outcomes, such as cognitive functioning, that are also important to those deciding which type of weight-loss diet to employ. Given that L-CHO ketogenic diets are known to affect brain function as evidenced by their ability to suppress seizure activity, it is reasonable to speculate whether L-CHO and high-carbohydrate (H-CHO) diets differ in their effects on cognitive function under other circumstances like dieting and weight loss.
One study in obese women (n=21) who consumed either a very-low-calorie ketogenic or non-ketogenic liquid formula diet for 28 days showed that attention and information processing did not differ as a function of diet; however, psychomotor and problem-solving performance were adversely affected in those consuming a ketogenic diet, primarily during the first week of dieting.17 A more recent study in overweight and obese women (n=19) showed that those consuming an energy-restricted, L-CHO diet for 3 weeks performed worse on a memory-based task but better on an attention-vigilance task than those consuming an energy-restricted H-CHO diet.18 To our knowledge, only one study has compared the effects of consuming an energy-restricted L-CHO or H-CHO diet on cognitive function in overweight and obese adults (n=106) for a period over 4 weeks.19 In this study, participants were instructed to consume less than 20 g of carbohydrate per day for the first 8 weeks. After 8 weeks, they could increase their intake to less than 40 g of carbohydrate per day for the remainder of the study. No differences in working memory were observed between groups after 8 weeks.20 Although both diet groups showed improvements in speed of processing after 8 weeks, the L-CHO group displayed a smaller improvement than the H-CHO group. There were no differences between groups in either working memory or speed of processing after 1 year.19
The purpose of this study was to compare the effects of two weight-reducing dietary approaches (L-CHO vs H-CHO diets) on attention, information processing, reaction time, short-term memory and executive function in overweight or obese men and women over a 6-month period.
Materials and methods
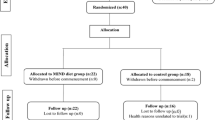
All study participants were enrolled in three-center, two-year randomized controlled trial comparing the effects of L-CHO and H-CHO diets for the treatment of obesity. Results for the main outcomes14 and secondary outcomes21, 22, 23, 24, 25 have been reported previously. A detailed description of the recruitment and screening procedures and assessments used in the parent study are available elsewhere.14 Each volunteer completed a medical and psychological screen. Individuals reporting psychiatric conditions, pre-existing health problems (for example, chronic diseases such as diabetes, hypertension, cardiovascular disease, stroke), use of prescription medications, regular alcohol, tobacco or other drug use were excluded from the study. The current study was a sub-study of the larger study and only involved the Philadelphia site. All participants at this site (n=106) were invited to participate in assessments of cognitive functioning before and after 1, 4, 12 and 26 weeks of treatment and 47 participants agreed to participate. The study was approved by the Institutional Review Board at Temple University.
Participants were randomized to treatment conditions and consumed a self-selected diet while participating in a comprehensive behavioral weight control program.14 Group sessions varied between the two treatment conditions only in the type of diet plan that was prescribed. A detailed description of the diets has been previously described14 but is summarized below. Participants in the L-CHO condition were instructed to follow a diet that was restricted in carbohydrate and unlimited in fat and protein. Participants were provided with information on L-CHO diets as well as numerous suggestions for meal plans. Instruction was consistent with the four recommended phases described in Dr Atkins’ New Diet Revolution.24 Participants in the H-CHO condition were encouraged to consume a diet consistent with the Dietary Guidelines for Americans25 (that is, 30% of calories from fat, 15% from protein and 55% from carbohydrate). Participants were instructed to make changes in dietary intake that included reducing fat and increasing the consumption of fruits, vegetables, breads and cereals. Suggested caloric intakes for men and women were set at 1500–1800 kcal d−1 and 1200–1500 kcal d−1, respectively.
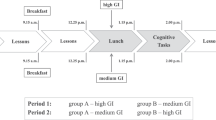
Participants in the current study completed five testing sessions in the laboratory. The week 1 assessment was based on a previous study17 showing impairments in cognitive function 1 week after initiation of a L-CHO diet. A minimum of one 30 min training session was required before the baseline assessment to familiarize participants with the computer tasks. Together with study staff each participant reviewed written instructions describing the procedures for completing the four computer-based performance tasks. Participants were given the opportunity to ask questions and to briefly practice each task in order to demonstrate that they understood how to complete the task. If a participant was unable to demonstrate comprehension of a particular task during the initial training session, (s)he would be given one additional opportunity to practice that particular task and demonstrate understanding (that is, there was a maximum of two training sessions).
On testing days, participants were instructed to consume lunch at noon from a list of suggested foods with known macronutrient compositions (consistent with the dietary prescriptions of the group to which they were randomized), eat a standard L-CHO snack (3% CHO, 180 calories) 2 h later, and to abstain from alcohol. Caffeinated beverages were allowed for regular consumers up until noon on testing days. Testing was conducted approximately 2 h following consumption of the snack to ensure that all participants were in the same fed state. Upon arrival, participants were asked to provide a urine sample (to assess ketones) and to complete a check-in questionnaire (to assess adherence to the pre-session procedures) as well as a VAS questionnaire (to assess hunger, craving and anxiety).
The STIM15 Complete System (Compumedics Neuroscan) was used, and the assessment battery included: the color and food Stroop task (attention and information processing);26 the Continuous Performance Task (CPT, attention and reaction time);27 word recall (verbal short-term memory)28 and the Wisconsin card-sorting task (problem solving, set-shifting and cognitive flexibility).29 Test order was randomly administered, and the performance battery took approximately 30 min to complete.
Statistical analysis
Comparisons between treatment group means over time were conducted with PROC GLIMMIX in SAS v. 9.3 (SAS Institute Inc., Cary, NC, USA). This procedure was designed for generalized linear mixed models, also called random coefficients or multilevel/hierarchical models.30 To build the models, baseline (visit=0) was entered as a covariate to ensure equal starting values between groups. Next, time was coded as 1, 4, 12 and 24 (visit months) and entered as a continuous variable. Overall trends for time were evaluated using linear and up to third order polynomial terms, and differences in trajectories between treatment groups were tested with interaction terms with dummy (0/1) coding for treatment groups. To accommodate the dependence caused by repeated measures for each subject over visits, initial models were parameterized with random intercepts and slopes along with the covariance between the variance components. Lack of significant P-values for regression coefficients as well as confidence intervals including zero for variance/covariance components led to final or reduced models with only random intercepts and linear or curvilinear (quadratic) fixed time slopes. Differences between groups were based on the P-values from the ‘fixed’ effects using α=0.05 as level of statistical significance. Significant time (P<0.05) by condition interactions were followed up with comparison between LSMEANS at each time point employing Bonferroni adjustment for multiple comparisons (P<0.0125).
Results
The sample consisted of 47 (25 males, 22 females) participants who were 70% Caucasian, 28% African American, 2% others, with a mean±s.d. age of 47.4±8.7 years and body mass index of 35.3±3.4 kg m−2. There were no significant differences between participants in the L-CHO (n=22) or the H-CHO (n=25) groups on any baseline variable.
Weight loss
Participants in the H-CHO group lost 0.6±1.0%, 3.4±1.6%, 7.4±4.3% and 9.7±5.6% of their baseline body weight at 1, 4, 12 and 24 weeks, respectively. Participants in the L-CHO group lost 0.5±1.6%, 4.0±2.1%, 8.5±3.8% and 11.4±5.6% of their baseline body weight at 1, 4, 12 and 24 weeks, respectively. There were no significant differences in weight loss between groups at any of the assessment points.
Ketones
There was no difference in concentrations of urinary ketones between groups at baseline. However, there was a significant main effect for time (P<0.0001) and a significant interaction between time and condition (P=0.0002) for urinary ketones. Compared with the H-CHO group, urinary ketones increased to a greater extent in the L-CHO group, particularly during the first week on the diet, and gradually declined over time, suggesting good adherence to L-CHO prescriptions, which increased carbohydrate intake over time (Figure 1).

Urinary ketones in participants consuming H-CHO and L-CHO diets before and after 1, 4, 12 and 26 weeks of treatment.
Cognitive performance tasks
Stroop
The dependent measure for this task was percentage of correct responses. There was a significant main effect for time (P<0.02) and a significant quadratic effect for time (P<0.05) for the percentage of correct responses made on the color Stroop task. The percentage of correct color responses significantly increased over time in both the H-CHO and L-CHO groups, but there was no difference between the groups (Figure 2). There were no significant effects on accuracy as a function of word type (that is, neutral or salient foods) on the food Stroop over time or between groups.

Percentage of correct responses on the color Stroop task in participants consuming H-CHO and L-CHO diets before and after 1, 4, 12 and 26 weeks of treatment.
CPT
The dependent measures were response time and number of correct responses. There were no significant differences over time or between groups in response time or number of correct responses on the CPT.
Word recall
The dependent measures for this task were percentage of correct responses and number of incorrect responses. There were no significant differences in the percentage of correct responses or number of incorrect responses over time or between groups.
Wisconsin card-sorting task
The dependent measures were mean response time and number of errors. There were no significant changes in the performance (that is, mean response time or number of errors) over time or between groups.
Discussion
This study investigated the cognitive effects of L-CHO and H-CHO weight-reducing diets over a 6-month period. The main findings from this study are: (1) weight loss has neither a positive or negative effect on cognitive function and (2) L-CHO and H-CHO weight-loss diets have similar effects on cognitive performance. Although others have reported some improvement in executive/attention functioning and memory with weight loss,12, 13 little improvement was observed in the current study. More specifically, with the exception of improved accuracy over time in both groups on the color Stroop task, assessing attention and information processing, there were no significant differences in performance over time or between groups on tasks assessing attention and reaction time (CPT), short-term memory (word recall) or problem solving (Wisconsin Card-Sorting Task).
In the most restrictive period of the current study (weeks 1–12), participants in the L-CHO group consumed 20 g of carbohydrate. Carbohydrate intake gradually increased by 5 g per day per week, depending on the rate of weight loss, for the remainder of the study. To our knowledge, only one other study has investigated the effects of consuming 20–40 g of carbohydrate as part of an energy-restricted diet on cognitive function in humans.6 In this study, participants were randomized to either a H-CHO diet (that is, 46% carbohydrate) or a L-CHO diet consisting of 9–20 g of carbohydrate per day for the first 8 weeks of the study and no more than 40 g of carbohydrate per day for the remaining 44 weeks of the study. Although there were no differences in working memory between the groups at 8 weeks, there were greater improvements in the speed of processing in the H-CHO diet group compared with the L-CHO group.20 There were, however, no differences in working memory or speed of processing between groups after 12 months.19 Those data along with findings from the current study suggest an overall minimal impact of L-CHO weight-loss diets prescribing 20 g of carbohydrate per day or more on cognitive function. It is important to note that these findings are limited to relatively healthy, overweight and obese, middle-aged adults and to the cognitive processes assessed in these studies.
Other studies suggest that L-CHO diets restricting carbohydrate intake to less than 20 g per day can affect performance in both positive and negative directions depending on the cognitive function assessed.18 One non-randomized study, in which participants completely withdrew from carbohydrates for the first week of the study, consumed 5–8 g of carbohydrate during the second week, and consumed 10–16 g of carbohydrate during the final week of the study, showed that individuals consuming L-CHO diets displayed faster reaction times on the CPT than those consuming a H-CHO diet18 (that is, Dietary Guidelines for Americans).25 In contrast, performance on memory tasks was worse in the L-CHO group compared with the H-CHO group. In addition, participants consuming a H-CHO diet displayed a practice effect over time and consistently responded faster to non-food words compared with food words on the Stroop task, whereas those consuming a L-CHO diet did not show a consistent practice effect and displayed little difference in reaction time as a function of word type. In another randomized study that prescribed either a H-CHO diet (that is, 52% carbohydrate) or a L-CHO diet consisting of 10 g of carbohydrate a day, no differences in performance were observed between groups at any time on the Stroop task or another task requiring sustained attention (digit vigilance task) but participants consuming the L-CHO diet performed worse on a task requiring mental flexibility (trail making task) between baseline and week 1 on the diet.17 These studies suggest that under conditions of more severe carbohydrate restriction, cognitive performance can either be enhanced or impaired depending on the type or complexity of the task.
This study had several strengths including a randomized design and dietary conditions (that is, self-selected foods, dietary prescriptions that followed popular weight-reducing diet strategies) that simulated a real-life setting. As such, the present findings can be more easily generalized to similar populations in the real world. In addition, all participants were given a standardized snack at a set time to ensure that they were all in the same metabolic state during testing. Further, weight loss was the same between groups so there was no confound of differential weight loss between the groups. Despite these strengths, the study has several weaknesses including a small sample size and a limited array of cognitive tasks. Larger sample sizes would allow for a greater diversity in participants (that is, ethnic background, age and so on) and a better ability to detect subtle differences in cognitive performance between groups. It is also possible that the testing parameters in this study were not stringent enough to tease out differences in cognitive performance or elicit differential responding between groups. Previous research has shown poorer performance on complex cognitive tasks but not on more basic cognitive tasks following L-CHO intake.17 A larger array of cognitive tasks would provide a better understanding of the types of mental functioning that can potentially be affected by diets with different macronutrient compositions. Although it is possible that the initial training session raised baseline performance, which might make it difficult to detect changes in subsequent performance, we do not feel that it made a significant impact because of the brevity of the training session.
Conclusion
In conclusion, these findings suggest that individuals participating in a 6-month behavioral weight-loss program randomized to either a L-CHO (that is, Dr Atkins’ New Diet Revolution) or a H-CHO (that is, Dietary Guidelines for Americans) diet experienced similar effects on cognitive performance. Performance on the color Stroop task improved over time in all participants but there were no differences in performance between groups. There were no differences in performance over time or between groups on any other task (that is, the food Stroop, CPT, Word recall or Wisconsin Card Sorting task).
References
Benton D, Parker PY . Breakfast, blood glucose, and cognition. Am J Clin Nutr 1998; 67: 772s–778s.
Sunram-Lea SI, Foster JK, Durlach P, Perez C . Glucose facilitation of cognitive performance in healthy young adults: examination of the influence of fast-duration, time of day and pre-consumption plasma glucose levels. Psychopharmacology 2001; 157: 46–54.
Green MW, Rogers PJ . Impaired cognitive-functioning during spontaneous dieting. Psychol Med 1995; 25: 1003–1010.
Green MW, Rogers PJ . Impairments in working memory associated with spontaneous dieting behaviour. Psychol Med 1998; 28: 1063–1070.
Kemps E, Tiggemann M . Working memory performance and preoccupying thoughts in female dieters: Evidence for a selective central executive impairment. Br J Clin Psychol 2005; 44: 357–366.
Kemps E, Tiggemann M, Marshall K . Relationship between dieting to lose weight and the functioning of the central executive. Appetite 2005; 45: 287–294.
Vreugdenburg L, Bryan J, Kemps E . The effect of self-initiated weight-loss dieting on working memory: the role of preoccupying cognitions. Appetite 2003; 41: 291–300.
Phelan S, Hassenstab J, McCaffery JM, Sweet L, Raynor HA, Cohen RA et al. Cognitive interference from food cues in weight loss maintainers, normal weight, and obese individuals. Obesity (Silver Spring) 2011; 19: 69–73.
Kretsch MJ, Green MW, Fong AKH, Elliman NA, Johnson HL . Cognitive effects of a long-term weight reducing diet. Int J Obes Relat Metab Disord 1997; 21: 14–21.
Bryan J, Tiggemann M . The effect of weight-loss dieting on cognitive performance and psychological well-being in overweight women. Appetite 2001; 36: 147–156.
Martin CK, Anton SD, Han HM, York-Crowe E, Redman LM, Ravussin E et al. Examination of cognitive function during six months of calorie restriction: results of a randomized controlled trial. Rejuvenation Res 2007; 10: 179–189.
Siervo M, Arnold R, Wells JCK, Tagliabue A, Colantuoni A, Albanese E et al. Intentional weight loss in overweight and obese individuals and cognitive function: a systematic review and meta-analysis. Obes Rev 2011; 12: 968–983.
Siervo M, Nasti G, Stephan BCM, Papa A, Muscariello E, Wells JCK et al. Effects of intentional weight loss on physical and cognitive function in middle-aged and older obese participants: a pilot study. J Am Coll Nutr 2012; 31: 79–86.
Foster GD, Wyatt HR, Hill JO, Makris AP, Rosenbaum DL, Brill C et al. Weight and metabolic outcomes after 2 years on a low-carbohydrate versus low-fat diet a randomized trial. Ann Int Med 2010; 153: 147–U37.
Makris A, Foster GD . Dietary approaches to the treatment of obesity. Psychiatr Clin North Am 2011; 34: 813–827.
Hu T, Mills KT, Yao L, Demanelis K, Eloustaz M, Yancy WS Jr. et al. Effects of low-carbohydrate diets versus low-fat diets on metabolic risk factors: a meta-analysis of randomized controlled clinical trials. Am J Epidemiol 2012; 176 (Suppl 7): S44–S54.
Wing RR, Vazquez JA, Ryan CM . Cognitive effects of ketogenic weight-reducing diets. Int J Obes Relat Metab Disord 1995; 19: 811–816.
D'Anci KE, Watts KL, Kanarek RB, Taylor HA . Low-carbohydrate weight-loss diets. Effects on cognition and mood. Appetite 2009; 52: 96–103.
Brinkworth GD, Buckley JD, Noakes M, Clifton PM, Wilson CJ . Long-term effects of a very low-carbohydrate diet and a low-fat diet on mood and cognitive function. Arch Int Med 2009; 169: 1873–1880.
Halyburton AK, Brinkworth GD, Wilson CJ, Noakes M, Buckley JD, Keogh JB et al. Low- and high-carbohydrate weight-loss diets have similar effects on mood but not cognitive performance. Am J Clin Nutr 2007; 86: 580–587.
Mohler ER 3rd, Sibley AA, Stein R, Davila-Roman V, Wyatt H, Badellino K et al. Endothelial function and weight loss: comparison of low-carbohydrate and low-fat diets. Obesity (Silver Spring) 2013; 21: 504–509.
Friedman AN, Ogden LG, Foster GD, Klein S, Stein R, Miller B et al. Comparative effects of low-carbohydrate high-protein versus low-fat diets on the kidney. Clin J Am Soc Nephrol 2012; 7: 1103–1111.
Martin CK, Rosenbaum D, Han H, Geiselman PJ, Wyatt HR, Hill JO et al. Change in food cravings, food preferences, and appetite during a low-carbohydrate and low-fat diet. Obesity (Silver Spring) 2011; 19: 1963–1970.
Atkins R . Dr Atkins' New Diet Revolution. Avon Books: New York, 1998.
Dietary Guidelines for Americans. In: USDA, SUDHHS Home and Garden Bulletin No. 232 5th edn. Home and Garden Bulletin: Washington, DC, 2000, (http://www.health.gov/dietaryguidelines/dga2000/document/back_cover.htm).
Stroop JR . Studies of interference in serial verbal reactions. J Exp Psychol 1935; 18: 643–662.
Rosvold HE, Mirsky AF, Sarason I, Bransome ED, Beck LH . A continuous performance-test of brain-Damage. J Consult Psychol 1956; 20: 343–350.
Sommerfield AJ, Deary IJ, McAulay V, Frier BM . Short-term, delayed, and working memory are impaired during hypoglycemia in individuals with type 1 diabetes. Diabetes Care 2003; 26: 390–396.
Berg EA . A simple objective technique for measuring flexibility in thinking. J Gen Psychol 1948; 39: 15–22.
Gelman A, Hill J . Data Analysis Using Regression and Multilevel/Hierarchial Models. Cambridge University Press: New York, 2007.
Acknowledgements
This study was supported by NIH grant # RO1 AT1103.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
S Klein is a stockholder for Aspire Bariatrics, is on the Advisory Board and/or is a consultant for Takeda Pharmaceuticals, Vivus, Aspire Baratins and ExpressScripts, is a member of Merck’s speakers bureau and receives endowments from Atkins Foundation Charitable Trust and the Kilo Foundation. HR Wyatt is a board member and/or on the advisory board for Eisai and Retrofit, a consultant for Wellspring, a stockholder for Active Planet, receives royalties from Up to Date, and receives research support from the American Beverage Association, GI Dynamics and Novo Nordisk. During the study, GDF served on the advisory board for ConAgra Foods, Novo Nordisk, Inc., Tate & Lyle, and United Health Group, was a consultant for Eisai, GlaxoSmithKline, and Medtronic, and received research support from the NIH, USDA, CDC, Robert Wood Johnson Foundation, American Beverage Association, and Novo Nordisk. GDF is currently employed at Weight Watchers. The remaining authors declare no conflict of interest.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Makris, A., Darcey, V., Rosenbaum, D. et al. Similar effects on cognitive performance during high- and low-carbohydrate obesity treatment. Nutr & Diabetes 3, e89 (2013). https://doi.org/10.1038/nutd.2013.29
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nutd.2013.29
Keywords
This article is cited by
-
Effect of Dietary Intake Through Whole Foods on Cognitive Function: Review of Randomized Controlled Trials
Current Nutrition Reports (2022)
-
Effects of very low-carbohydrate vs. high-carbohydrate weight loss diets on psychological health in adults with obesity and type 2 diabetes: a 2-year randomized controlled trial
European Journal of Nutrition (2021)
-
Higher baseline irisin concentrations are associated with greater reductions in glycemia and insulinemia after weight loss in obese subjects
Nutrition & Diabetes (2014)
