
Abstract
Delirium is a common and serious acute neuropsychiatric syndrome with core features of inattention and global cognitive dysfunction. The etiologies of delirium are diverse and multifactorial and often reflect the pathophysiological consequences of an acute medical illness, medical complication or drug intoxication. Delirium can have a widely variable presentation, and is often missed and underdiagnosed as a result. At present, the diagnosis of delirium is clinically based and depends on the presence or absence of certain features. Management strategies for delirium are focused on prevention and symptom management. This article reviews current clinical practice in delirium in elderly individuals, including the diagnosis, treatment, outcomes and economic impact of this syndrome. Areas of future research are also discussed.
Key Points
-
Delirium is a frequent cause and a serious complication of hospitalization and has important implications from both a functional and an economic standpoint
-
Delirium is potentially preventable and treatable, but major barriers, including underrecognition of the syndrome and poor understanding of the underlying pathophysiology, have hampered the development of successful therapies
-
Neuroimaging has identified structural changes, including cortical atrophy, ventricular dilatation and white matter lesions, to be predictors of delirium
-
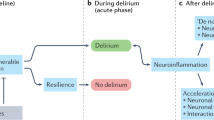
Current evidence suggests that disruption of neurotransmission, inflammation or acute stress responses might contribute markedly to the development of delirium
-
Delirium is not always transient and reversible, and it can result in long-term cognitive changes
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


References
Chadwick, J. & Mann, M. N. The Medical Works of Hippocrates (Blackwell, Oxford, 1950).
Morandi, A. et al. Understanding international differences in terminology for delirium and other types of acute brain dysfunction in critically ill patients. Intensive Care Med. 34, 1907–1915 (2008).
Inouye, S. K. Predisposing and precipitating factors for delirium in hospitalized older patients. Dement. Geriatr. Cogn. Disord. 10, 393–400 (1999).
Inouye, S. K. Delirium in hospitalized older patients: recognition and risk factors. J. Geriatr. Psychiatry Neurol. 11, 118–125 (1998).
US Department of Health and Human Services. CMS statistics (publication no. 03445, Centers for Medicare and Medicaid Services, Washington, DC, 2004).
Inouye, S. K. Delirium in hospitalized older patients. Clin. Geriatr. Med. 14, 745–764 (1998).
Siddiqi, N., House, A. O. & Holmes, J. D. Occurrence and outcome of delirium in medical in-patients: a systematic literature review. Age Ageing 35, 350–364 (2006).
Bruce, A. J., Ritchie, C. W., Blizard, R., Lai, R. & Raven, P. The incidence of delirium associated with orthopedic surgery: a meta-analytic review. Int. Psychogeriatr. 19, 197–214 (2007).
Girard, T. D. & Ely, E. W. Delirium in the critically ill patient. Handb. Clin. Neurol. 90, 39–56 (2008).
Inouye, S. K. Delirium in older persons. N. Engl. J. Med. 354, 1157–1165 (2006).
Pisani, M. A., McNicoll, L. & Inouye, S. K. Cognitive impairment in the intensive care unit. Clin. Chest Med. 24, 727–737 (2003).
Fong, T. G. et al. Cerebral perfusion changes in older delirious patients using 99mTc HMPAO SPECT. J. Gerontol. A Biol. Sci. Med. Sci. 61, 1294–1299 (2006).
Yokota, H., Ogawa, S., Kurokawa, A. & Yamamoto, Y. Regional cerebral blood flow in delirium patients. Psychiatry Clin. Neurosci. 57, 337–339 (2003).
Hshieh, T. T., Fong, T. G., Marcantonio, E. R. & Inouye, S. K. Cholinergic deficiency hypothesis in delirium: a synthesis of current evidence. J. Gerontol. A Biol. Sci. Med. Sci. 63, 764–772 (2008).
Eikelenboom, P. & Hoogendijk, W. J. Do delirium and Alzheimer's dementia share specific pathogenetic mechanisms? Dement. Geriatr. Cogn. Disord. 10, 319–324 (1999).
Han, L. et al. Use of medications with anticholinergic effect predicts clinical severity of delirium symptoms in older medical inpatients. Arch. Intern. Med. 161, 1099–1105 (2001).
Blitt, C. D. & Petty, W. C. Reversal of lorazepam delirium by physostigmine. Anesth. Analg. 54, 607–608 (1975).
Mendelson, G. Pheniramine aminosalicylate overdosage. Reversal of delirium and choreiform movements with tacrine treatment. Arch. Neurol. 34, 313 (1977).
Schuster, P., Gabriel, E., Kufferle, B., Strobl, G. & Karobath, M. Reversal by physostigmine of clozapine-induced delirium. Clin. Toxicol. 10, 437–441 (1977).
Flacker, J. M. et al. The association of serum anticholinergic activity with delirium in elderly medical patients. Am. J. Geriatr. Psychiatry 6, 31–41 (1998).
Mach, J. R. et al. Serum anticholinergic activity in hospitalized older persons with delirium: a preliminary study. J. Am. Geriatr. Soc. 43, 491–495 (1995).
Mussi, C., Ferrari, R., Ascari, S. & Salvioli, G. Importance of serum anticholinergic activity in the assessment of elderly patients with delirium. J. Geriatr. Psychiatry Neurol. 12, 82–86 (1999).
Flacker, J. M. & Lipsitz, L. A. Serum anticholinergic activity changes with acute illness in elderly medical patients. J. Gerontol. A Biol. Sci. Med. Sci. 54, M12–M16 (1999).
Thomas, C. et al. Serum anticholinergic activity and cerebral cholinergic dysfunction: an EEG study in frail elderly with and without delirium. BMC Neurosci. 9, 86 (2008).
Trzepacz, P. T. Is there a final common neural pathway in delirium? Focus on acetylcholine and dopamine. Semin. Clin. Neuropsychiatry 5, 132–148 (2000).
Young, B. K., Camicioli, R. & Ganzini, L. Neuropsychiatric adverse effects of antiparkinsonian drugs. Characteristics, evaluation and treatment. Drugs Aging 10, 367–383 (1997).
Gaudreau, J. D. & Gagnon, P. Psychotogenic drugs and delirium pathogenesis: the central role of the thalamus. Med. Hypotheses 64, 471–475 (2005).
Rudolph, J. L. et al. Chemokines are associated with delirium after cardiac surgery. J. Gerontol. A Biol. Sci. Med. Sci. 63, 184–189 (2008).
Maclullich, A. M., Ferguson, K. J., Miller, T., de Rooij, S. E. & Cunningham, C. Unravelling the pathophysiology of delirium: a focus on the role of aberrant stress responses. J. Psychosom. Res. 65, 229–238 (2008).
Dilger, R. N. & Johnson, R. W. Aging, microglial cell priming, and the discordant central inflammatory response to signals from the peripheral immune system. J. Leukoc. Biol. 84, 932–939 (2008).
Dunn, A. J. Effects of cytokines and infections on brain neurochemistry. Clin. Neurosci. Res. 6, 52–68 (2006).
Eikelenboom, P., Hoogendijk, W. J., Jonker, C. & van Tilburg, W. Immunological mechanisms and the spectrum of psychiatric syndromes in Alzheimer's disease. J. Psychiatr. Res. 36, 269–280 (2002).
de Rooij, S. E., van Munster, B. C., Korevaar, J. C. & Levi, M. Cytokines and acute phase response in delirium. J. Psychosom. Res. 62, 521–525 (2007).
Cunningham, C. et al. Systemic inflammation induces acute behavioral and cognitive changes and accelerates neurodegenerative disease. Biol. Psychiatry 65, 304–312 (2009).
van Munster, B. C. et al. Time-course of cytokines during delirium in elderly patients with hip fractures. J. Am. Geriatr. Soc. 56, 1704–1709 (2008).
Trzepacz, P. T. & van der Mast, R. The Neuropathophysiology of Delirium (Oxford University Press, Oxford, 2002).
Kudoh, A., Takase, H., Katagai, H. & Takazawa, T. Postoperative interleukin-6 and cortisol concentrations in elderly patients with postoperative confusion. Neuroimmunomodulation 12, 60–66 (2005).
McIntosh, T. K. et al. Beta-endorphin, cortisol and postoperative delirium: a preliminary report. Psychoneuroendocrinology 10, 303–313 (1985).
Robertsson, B. et al. Hyperactivity in the hypothalamic-pituitary-adrenal axis in demented patients with delirium. Int. Clin. Psychopharmacol. 16, 39–47 (2001).
O'Keeffe, S. T. & Devlin, J. G. Delirium and the dexamethasone suppression test in the elderly. Neuropsychobiology 30, 153–156 (1994).
McKeith, I. G. Clinical use of the DST in a psychogeriatric population. Br. J. Psychiatry 145, 389–393 (1984).
Soiza, R. L. et al. Neuroimaging studies of delirium: a systematic review. J. Psychosom. Res. 65, 239–248 (2008).
Burns, A., Gallagley, A. & Byrne, J. Delirium. J. Neurol. Neurosurg. Psychiatry 75, 362–367 (2004).
Kishi, Y., Iwasaki, Y., Takezawa, K., Kurosawa, H. & Endo, S. Delirium in critical care unit patients admitted through an emergency room. Gen. Hosp. Psychiatry 17, 371–379 (1995).
Jalan, R. et al. Oral amino acid load mimicking hemoglobin results in reduced regional cerebral perfusion and deterioration in memory tests in patients with cirrhosis of the liver. Metab. Brain Dis. 18, 37–49 (2003).
Strauss, G. I. et al. Regional cerebral blood flow during mechanical hyperventilation in patients with fulminant hepatic failure. Hepatology 30, 1368–1373 (1999).
Yazgan, Y. et al. Value of regional cerebral blood flow in the evaluation of chronic liver disease and subclinical hepatic encephalopathy. J. Gastroenterol. Hepatol. 18, 1162–1167 (2003).
Alsop, D. C. et al. The role of neuroimaging in elucidating delirium pathophysiology. J. Gerontol. A Biol. Sci. Med. Sci. 61, 1287–1293 (2006).
Lipowski, Z. J. Transient cognitive disorders (delirium, acute confusional states) in the elderly. Am. J. Psychiatry 140, 1426–1436 (1983).
McCusker, J., Cole, M., Abrahamowicz, M., Primeau, F. & Belzile, E. Delirium predicts 12-month mortality. Arch. Intern. Med. 162, 457–463 (2002).
Hufschmidt, A. & Shabarin, V. Diagnostic yield of cerebral imaging in patients with acute confusion. Acta Neurol. Scand. 118, 245–250 (2008).
Inouye, S. K. et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann. Intern. Med. 113, 941–948 (1990).
Wei, L. A., Fearing, M. A., Sternberg, E. J. & Inouye, S. K. The Confusion Assessment Method: a systematic review of current usage. J. Am. Geriatr. Soc. 56, 823–830 (2008).
Breitbart, W. et al. The Memorial Delirium Assessment Scale. J. Pain Symptom Manage. 13, 128–137 (1997).
The Hospital Elder Life Program (HELP) http://www.hospitalelderlifeprogram.org.
Inouye, S. K. et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N. Engl. J. Med. 340, 669–676 (1999).
Marcantonio, E. R., Flacker, J. M., Wright, R. J. & Resnick, N. M. Reducing delirium after hip fracture: a randomized trial. J. Am. Geriatr. Soc. 49, 516–522 (2001).
Caplan, G. A., Coconis, J., Board, N., Sayers, A. & Woods, J. Does home treatment affect delirium? A randomised controlled trial of rehabilitation of elderly and care at home or usual treatment (The REACH-OUT trial). Age Ageing 35, 53–60 (2006).
Kaneko, T. et al. Prophylactic consecutive administration of haloperidol can reduce the occurrence of postoperative delirium in gastrointestinal surgery. Yonago Acta. Med. 42, 179–184 (1999).
Kalisvaart, K. J. et al. Haloperidol prophylaxis for elderly hip-surgery patients at risk for delirium: a randomized placebo-controlled study. J. Am. Geriatr. Soc. 53, 1658–1666 (2005).
Liptzin, B., Laki, A., Garb, J. L., Fingeroth, R. & Krushell, R. Donepezil in the prevention and treatment of post-surgical delirium. Am. J. Geriatr. Psychiatry 13, 1100–1106 (2005).
Sampson, E. L. et al. A randomized, double-blind, placebo-controlled trial of donepezil hydrochloride (Aricept) for reducing the incidence of postoperative delirium after elective total hip replacement. Int. J. Geriatr. Psychiatry 22, 343–349 (2007).
Noyan, M. A., Elbi, H. & Aksu, H. Donepezil for anticholinergic drug intoxication: a case report. Prog. Neuropsychopharmacol. Biol. Psychiatry 27, 885–887 (2003).
Slatkin, N. & Rhiner, M. Treatment of opioid-induced delirium with acetylcholinesterase inhibitors: a case report. J. Pain Symptom Manage. 27, 268–273 (2004).
Wengel, S. P., Roccaforte, W. H. & Burke, W. J. Donepezil improves symptoms of delirium in dementia: implications for future research. J. Geriatr. Psychiatry Neurol. 11, 159–161 (1998).
Gleason, O. C. Donepezil for postoperative delirium. Psychosomatics 44, 437–438 (2003).
Bourne, R. S., Tahir, T. A., Borthwick, M. & Sampson, E. L. Drug treatment of delirium: past, present and future. J. Psychosom. Res. 65, 273–282 (2008).
Leung, J. M. et al. Pilot clinical trial of gabapentin to decrease postoperative delirium in older patients. Neurology 67, 1251–1253 (2006).
Levanen, J., Makela, M. L. & Scheinin, H. Dexmedetomidine premedication attenuates ketamine-induced cardiostimulatory effects and postanesthetic delirium. Anesthesiology 82, 1117–1125 (1995).
Budd, S. & Brown, W. Effect of a reorientation technique on postcardiotomy delirium. Nurs. Res. 23, 341–348 (1974).
Cole, M. et al. Systematic intervention for elderly inpatients with delirium: a randomized trial. Can. Med. Assoc. J. 151, 965–970 (1994).
Lazarus, H. & Hagens, J. Prevention of psychosis following open-heart surgery. Am. J. Psychiatry 124, 1190–1195 (1968).
Meagher, D., O'Hanlon, D., O'Mahony, E. & Casey, P. The use of environmental strategies and psychotropic medication in the management of delirium. Br. J. Psychiatry 168, 512–515 (1996).
Williams, M., Campbell, E., Raynor, W., Mlynarczyk, S. & Ward, S. Reducing acute confusional states in elderly patients with hip fractures. Res. Nurs. Health 8, 329–337 (1985).
American Psychiatric Association. Treatment of Patients with Delirium Practice Guideline http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm.
McDowell, J. A., Mion, L. C., Lydon, T. J. & Inouye, S. K. A nonpharmacologic sleep protocol for hospitalized older patients. J. Am. Geriatr. Soc. 46, 700–705 (1998).
Inouye, S. K., Bogardus, S. T., Jr, Williams, C. S., Leo-Summers, L. & Agostini, J. V. The role of adherence on the effectiveness of nonpharmacologic interventions: evidence from the delirium prevention trial. Arch. Intern. Med. 163, 958–964 (2003).
Lonergan, E., Britton, A. M., Luxenberg, J. & Wyller, T. Antipsychotics for delirium. Cochrane Database of Systematic Reviews, 2007, Issue 2. Art. No.: CD005594. DOI:10.1002/14651858.CD005594.pub2 (2007).
Seitz, D. P., Gill, S. S. & van Zyl, L. T. Antipsychotics in the treatment of delirium: a systematic review. J. Clin. Psychiatry 68, 11–21 (2007).
Platt, M. M. et al. Efficacy of neuroleptics for hypoactive delirium. J. Neuropsychiatry Clin. Neurosci. 6, 66–67 (1994).
Breitbart, W. et al. A double-blind trial of haloperidol, chlorpromazine, and lorazepam in the treatment of delirium in hospitalized AIDS patients. Am. J. Psychiatry 153, 231–237 (1996).
Hu, H., Deng, W., Yang, H. & Liu, Y. Olanzapine and haloperidol for senile delirium: a randomized controlled observation. Chin. J. Clin. Rehab. 10, 188–190 (2006).
Han, C. S. & Kim, Y. K. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics 45, 297–301 (2004).
Kim, J. Y. et al. Antipsychotics and dopamine transporter gene polymorphisms in delirium patients. Psychiatry Clin. Neurosci. 59, 183–188 (2005).
US FDA MedWatch: Haloperidol (marketed as Haldol, Haldol decanoate, and Haldol lactate) http://www.fda.gov/medwatch/safety/2007/safety07.htm#Haloperidol.
Inouye, S. & Marcantonio, E. Delirium. In The Dementias (eds Growdon J and Rossor M) 285–312 (Butterworth-Heinemann Elsevier, Philadelphia, 2007).
Marcantonio, E., Ta, T., Duthie, E. & Resnick, N. M. Delirium severity and psychomotor types: their relationship with outcomes after hip fracture repair. J. Am. Geriatr. Soc. 50, 850–857 (2002).
Levkoff, S. E. et al. Delirium. The occurrence and persistence of symptoms among elderly hospitalized patients. Arch. Intern. Med. 152, 334–340 (1992).
Murray, A. M. et al. Acute delirium and functional decline in the hospitalized elderly patient. J. Gerontol. 48, M181–M186 (1993).
Cole, M., McCusker, J., Dendukuri, N. & Han, L. The prognostic significance of subsyndromal delirium in elderly medical inpatients. J. Am. Geriatr. Soc. 51, 754–760 (2003).
Levkoff, S. E. & Marcantonio, E. R. Delirium: a major diagnostic and therapeutic challenge for clinicians caring for the elderly. Compr. Ther. 20, 550–557 (1994).
Marcantonio, E. R., Flacker, J. M., Michaels, M. & Resnick, N. M. Delirium is independently associated with poor functional recovery after hip fracture. J. Am. Geriatr. Soc. 48, 618–624 (2000).
McCusker, J., Cole, M., Dendukuri, N., Han, L. & Belzile, E. The course of delirium in older medical inpatients: a prospective study. J. Gen. Intern. Med. 18, 696–704 (2003).
Rockwood, K. The occurrence and duration of symptoms in elderly patients with delirium. J. Gerontol. 48, M162–M166 (1993).
Clarfield, A. M. The reversible dementias: do they reverse? Ann. Intern. Med. 109, 476–486 (1988).
Fann, J. R., Alfano, C. M., Roth-Roemer, S., Katon, W. J. & Syrjala, K. L. Impact of delirium on cognition, distress, and health-related quality of life after hematopoietic stem-cell transplantation. J. Clin. Oncol. 25, 1223–1231 (2007).
Katz, I. R. et al. Validating the diagnosis of delirium and evaluating its association with deterioration over a one-year period. Am. J. Geriatr. Psychiatry 9, 148–159 (2001).
McCusker, J., Cole, M., Dendukuri, N., Belzile, E. & Primeau, F. Delirium in older medical inpatients and subsequent cognitive and functional status: a prospective study. CMAJ 165, 575–583 (2001).
Rahkonen, T., Luukkainen-Markkula, R., Paanila, S., Sivenius, J. & Sulkava, R. Delirium episode as a sign of undetected dementia among community dwelling elderly subjects: a 2 year follow up study. J. Neurol. Neurosurg. Psychiatry 69, 519–521 (2000).
Fong, T. G. et al. Delirium accelerates cognitive decline in Alzheimer's disease. Neurology, in press.
Baker, F. M., Wiley, C., Kokmen, E., Chandra, V. & Schoenberg, B. S. Delirium episodes during the course of clinically diagnosed Alzheimer's disease. J. Natl Med. Assoc. 91, 625–630 (1999).
Fick, D. & Foreman, M. Consequences of not recognizing delirium superimposed on dementia in hospitalized elderly individuals. J. Gerontol. Nurs. 26, 30–40 (2000).
Rockwood, K. et al. The risk of dementia and death after delirium. Age Ageing 28, 551–556 (1999).
Williamson, J. W. Formulating priorities for quality assurance activity. Description of a method and its application. JAMA 239, 631–637 (1978).
National Quality Measures Clearinghouse™ of the Agency for Healthcare Research and Quality http://www.qualitymeasures.ahrq.gov/ (accessed 13 February 2009).
Sloss, E. M. et al. Selecting target conditions for quality of care improvement in vulnerable older adults. J. Am. Geriatr. Soc. 48, 363–369 (2000).
Inouye, S. K., Schlesinger, M. J. & Lydon, T. J. Delirium: a symptom of how hospital care is failing older persons and a window to improve quality of hospital care. Am. J. Med. 106, 565–573 (1999).
Leslie, D. L., Marcantonio, E. R., Zhang, Y., Leo-Summers, L. & Inouye, S. K. One-year health care costs associated with delirium in the elderly population. Arch. Intern. Med. 168, 27–32 (2008).
Haentjens, P., Lamraski, G. & Boonen, S. Costs and consequences of hip fracture occurrence in old age: an economic perspective. Disabil. Rehabil. 27, 1129–1141 (2005).
Stevens, J. A., Corso, P. S., Finkelstein, E. A. & Miller, T. R. The costs of fatal and non-fatal falls among older adults. Inj. Prev. 12, 290–295 (2006).
Hogan, P., Dall, T. & Nikolov, P. Economic costs of diabetes in the US in 2002. Diabetes Care 26, 917–932 (2003).
Thom, T. et al. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 113, e85–e151 (2006).
Ely, E. W. et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM–ICU). JAMA 286, 2703–2710 (2001).
Ely, E. W. et al. Evaluation of delirium in critically ill patients: validation of the Confusion Assessment Method for the Intensive Care Unit (CAM–ICU). Crit. Care Med. 29, 1370–1379 (2001).
Trzepacz, P. T. et al. Validation of the Delirium Rating Scale-revised-98: comparison with the delirium rating scale and the cognitive test for delirium. J. Neuropsychiatry Clin. Neurosci. 13, 229–242 (2001).
Albert, M. S. et al. The delirium symptom interview: an interview for the detection of delirium symptoms in hospitalized patients. J. Geriatr. Psychiatry Neurol. 5, 14–21 (1992).
Neelon, V. J., Champagne, M. T., Carlson, J. R. & Funk, S. G. The NEECHAM Confusion Scale: construction, validation, and clinical testing. Nurs. Res. 45, 324–330 (1996).
Bergeron, N., Dubois, M. J., Dumont, M., Dial, S. & Skrobik, Y. Intensive Care Delirium Screening Checklist: evaluation of a new screening tool. Intensive Care Med. 27, 859–864 (2001).
Hart, R. P., Best, A. M., Sessler, C. N. & Levenson, J. L. Abbreviated cognitive test for delirium. J. Psychosom. Res. 43, 417–423 (1997).
Hart, R. P. et al. Validation of a cognitive test for delirium in medical ICU patients. Psychosomatics 37, 533–546 (1996).
Acknowledgements
The authors are supported by NIA PHS Grants K24AG000949 (SK Inouye) and K23AG031320 (TG Fong), and Grant IIRG-08-88737 (SK Inouye) from the Alzheimer's Association. Désirée Lie, University of California, Irvine, CA, is the author of and is solely responsible for the content of the learning objectives, questions and answers of the Medscape-accredited continuing medical education activity associated with this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
About this article
Cite this article
Fong, T., Tulebaev, S. & Inouye, S. Delirium in elderly adults: diagnosis, prevention and treatment. Nat Rev Neurol 5, 210–220 (2009). https://doi.org/10.1038/nrneurol.2009.24
Issue Date:
DOI: https://doi.org/10.1038/nrneurol.2009.24
This article is cited by
-
Correlation and influencing factors of preoperative anxiety, postoperative pain, and delirium in elderly patients undergoing gastrointestinal cancer surgery
BMC Anesthesiology (2023)
-
Regional versus general anesthesia in older patients for hip fracture surgery: a systematic review and meta-analysis of randomized controlled trials
Journal of Orthopaedic Surgery and Research (2023)
-
Predicting delirium in older non-intensive care unit inpatients: development and validation of the DELIrium risK Tool (DELIKT)
International Journal of Clinical Pharmacy (2023)
-
Effect of remimazolam on the incidence of delirium after transcatheter aortic valve implantation under general anesthesia: a retrospective exploratory study
Journal of Anesthesia (2023)
-
Ältere PatientInnen in der Viszeralchirurgie
Die Chirurgie (2023)
