
Abstract
Neuroimaging has shown promise as a tool to predict likelihood of treatment response in adult anxiety disorders, with potential implications for clinical decision-making. Despite the relatively high prevalence and emergence of anxiety disorders in youth, very little work has evaluated neural predictors of response to treatment. The goal of the current study was to examine brain function during emotional face processing as a predictor of response to treatment in children and adolescents (age 7–19 years; N=41) with generalized, social, and/or separation anxiety disorder. Prior to beginning treatment with the selective serotonin reuptake inhibitor (SSRI) sertraline or cognitive behavior therapy (CBT), participants completed an emotional faces matching task during functional magnetic resonance imaging (fMRI). Whole brain responses to threatening (ie, angry and fearful) and happy faces were examined as predictors of change in anxiety severity following treatment. Greater activation in inferior and superior frontal gyri, including dorsolateral prefrontal cortex and ventrolateral prefrontal cortex, as well as precentral/postcentral gyri during processing of threatening faces predicted greater response to CBT and SSRI treatment. For processing of happy faces, activation in postcentral gyrus was a significant predictor of treatment response. Post-hoc analyses indicated that effects were not significantly moderated by type of treatment. Findings suggest that greater activation in prefrontal regions involved in appraising and regulating responses to social signals of threat predict better response to SSRI and CBT treatment in anxious youth and that neuroimaging may be a useful tool for predicting how youth will respond to treatment.
Similar content being viewed by others

INTRODUCTION
Anxiety disorders are among the most prevalent psychiatric disorders in children and adolescents and predict great burden into adulthood (Copeland et al, 2014; Merikangas et al, 2010; Weems and Silverman, 2013; Woodward and Fergusson, 2001). Separation, social, and generalized anxiety disorder (GAD) are particularly common among youth, with relatively early ages of onset and high rates of co-occurence with each other (Mohatt et al, 2014; Verduin and Kendall, 2003). Although both pharmacological (ie, selective serotonin reuptake inhibitors (SSRIs)) and cognitive behavioral therapy (CBT) are effective in treating pediatric anxiety disorders, approximately 40–45% of youth fail to show significant improvement in symptoms (Mohatt et al, 2014; Walkup et al, 2008), raising the need to identify predictors of treatment response.
There is growing evidence that brain function as measured by neuroimaging can predict treatment response better than behavioral or clinical measures (Gabrieli et al, 2015; Whitfield-Gabrieli et al, 2015). For example, anterior cingulate cortex (ACC) reactivity measured by functional magnetic resonance imaging (fMRI) has been shown to predict responses to pharmacological and psychotherapy treatment in depression (Ball et al, 2014a; Fu et al, 2013). In contrast, the existing literature on predictors of response to treatment in anxiety disorders is much smaller (Ball et al, 2014a).
The neurocircuity underlying threat processing may be particularly relevant to treatment response in anxiety. Consistent with this, activation in the amydala, involved in signaling the presence of threat, has been shown to predict response to treatment in anxiety (McClure et al, 2007a; Whalen et al, 2008); however, results have been inconsistent. Less amygdala reactivity in adults with GAD predicted better response to venlafaxine (Whalen et al, 2008), yet greater amygdala activation predicted better response to CBT or fluoxetine in anxious youth (McClure et al, 2007a), and other studies have failed to find amygdala effects (Doehrmann et al, 2013; Klumpp et al, 2013; Nitschke et al, 2009). Other work has indicated that greater activation to threatening faces in visual processing regions (ie, occipital and temporal gyri) involved in detecting and appraising emotional cues predicted better response to CBT among adults with social anxiety disorder (Doehrmann et al, 2013; Klumpp et al, 2013), possibly indicating greater initial threat reactivity which can be modified by treatment.
Brain regions involved in appraising and regulating emotion, including ACC and lateral and medial prefrontal cortex (PFC; Frank et al, 2014; Kober et al, 2008; Kohn et al, 2014; Phillips et al, 2003), may also predict treatment response in anxiety. For example, greater ACC activation during threat processing predicted better response to medication and CBT for adults with GAD (Nitschke et al, 2009; Whalen et al, 2008) and social anxiety disorder (Klumpp et al, 2013). Greater dorsolateral PFC (dlPFC) activation during emotion regulation predicted response to treatment in adults with GAD or panic disorder (Ball et al, 2014b), and dlPFC and ventrolateral PFC (vlPFC) activation to threat predicted CBT response in socially anxious adults (Doehrmann et al, 2013).
Only one previous fMRI study has examined predictors of treatment response in anxious youth, with analyses limited to amygdala activation to threat (McClure et al, 2007a). Given the relatively high prevalence of anxiety disorders in children and adolescents (Costello et al, 2005; Merikangas et al, 2010) and evidence that the neural circuitry involved in emotional processing develops into young adulthood (Monk, 2008), evaluating neural predictors of treatment response among youth is essential. In addition, it remains unclear the extent to which patterns of brain activation predict general response to treatment or may be useful for selecting treatments with the highest likelihood of success.
The current study examined brain activation to emotional faces as predictors of response to treatment in anxious youth (N=41). This two-site study was modeled after the Child/Adolescent Anxiety Multimodal Study (Compton et al, 2010) in that it included youth across a large span of development (7–19 years) with primary diagnoses of GAD, social anxiety disorder, or separation anxiety disorder, three of the most common anxiety disorders in youth (Compton et al, 2010; Mohatt et al, 2014), treated with either sertraline (ie, SSRI) or psychotherapy (ie, CBT). Prior to beginning treatment, participants completed an fMRI emotional faces task in which brain responses to angry, fearful, and happy faces were measured. Given the limited existing work on predictors of treatment response in anxious youth, analyses examined whole-brain activation to emotional faces to identify predictors of change in anxiety severity following treatment. As previous fMRI work in anxious adults has indicated that brain activation during threat processing predicts response to treatment (eg, Ball et al, 2014b; Doehrmann et al, 2013; Klumpp et al, 2013), our primary analyses focused on responses to threatening (ie, angry and fearful) faces, with secondary analyses examining response to happy faces. To maximize power, our primary analyses examined predictors across treatment types, and additional post-hoc analyses examined whether effects were moderated by treatment or clinical characteristics.
MATERIALS AND METHODS
Participants
Participants were part of a pediatric anxiety treatment study at the University of Michigan (UM) and University of Illinois at Chicago (UIC). Treatment-seeking youth between the ages of 7 and 19 years with primary diagnoses of GAD, social anxiety disorder, or separation anxiety disorder were eligible to participate. Diagnoses were obtained through the Schedule of Affective Disorders and Schizophrenia for School-Age Children (Kaufman et al, 1997) clinical interview administered by Master’s or Doctoral level clinicians (see Kujawa et al, 2015 for more details). History of bipolar disorder, schizophrenia, intellectual disability, pervasive development disorders, current substance use disorders, severe depression, or suicidal ideation was exclusionary. Participants with secondary comorbid anxiety, depressive, or externalizing disorders were included in the study (see Participant Characteristics). Participants were not taking psychotropic medications or in psychotherapy for at least 4 weeks prior to the initial assessment.
A total of 53 anxious youth completed the fMRI emotional faces task, followed by a minimum of 10 weeks of pharmacotherapy or psychotherapy. Data from 11 participants were excluded for movement during the fMRI (>3 mm) and 1 participant was excluded for low accuracy on the task (<20%), leaving a total sample of 41 youth with pretreatment fMRI and clinical measures and posttreatment clinical measures. The included sample was 63.4% female; and 78.0% Caucasian, 4.9% African American, 4.9% Asian, 2.4% Pacific Islander, and 9.8% multiracial, with 19.5% identifying as Hispanic/Latino.
Procedure
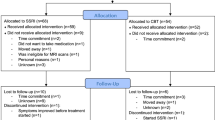
Procedures were approved by the Institutional Review Boards at both UM and UIC. Participants completed the clinical interview and pretreatment symptom measures, followed by the fMRI scan. At UM, participants were offered and self-selected treatment with SSRI or CBT. At UIC, participants were initially randomly assigned to receive either an SSRI or CBT but could opt to switch from SSRI to CBT owing to intolerable side effects. SSRI treatment consisted of 12 weeks of sertraline prescribed by a child psychiatrist during medication management sessions, beginning with a dose of 25 mg/day and in a flexible-dosing design increasing on subsequent visits up to 200 mg/day based on tolerability and treatment response. CBT was delivered through weekly 60-min sessions (up to a maximum of 18 sessions, as clinically indicated) by a Master’s or Doctoral level clinician. Treatment followed an established manualized CBT intervention for pediatric anxiety: the Coping Cat for younger children and C.A.T. Project for adolescents (Kendall and Hedtke, 2006; Kendall et al, 2002), which include psychoeducation, cognitive restructuring, and in vivo exposures. Participants who completed at least 10 sessions of SSRI or CBT and posttreatment symptom measures were included in the current study. Posttreatment symptom measures were completed at the last treatment session (on average, 18.99; SD=5.49 weeks after the initial screening visit).
Measures
Emotional face processing task
Participants performed a modified version of the emotional face processing task by Hariri et al (2002). The task was completed across two runs and consisted of 18 face blocks (6 each for fearful, angry, and happy faces) interspersed with 18 shape-matching blocks. Each block lasted 20 s, containing 4 matching trials (5 s each). During face-matching blocks, participants viewed three faces and were instructed to match the emotion of the target face on the top with one of the two faces at the bottom. The target (top) and matching probe (bottom) displayed angry, fearful, or happy expressions; the foil face (bottom) displayed a neutral expression. Three blocks of each expression (ie, angry, fearful, and happy) were included. During shape-matching blocks, participants were instructed to match a trio of simple shapes (ie, circles, rectangles, and triangles).
fMRI data acquisition and processing
MRI data were collected on 3 Tesla GE scanners with eight-channel head coils at both sites. At UM, functional data were collected with a gradient-echo reverse spiral acquisition with the following parameters: repetition time (TR)=2 s, echo time (TE)=30 ms, flip angle=90°, field of view (FOV)=22 × 22 cm, acquisition matrix 64 × 64, 3-mm slice thickness, 43 axial slices, 180 volumes per run. At UIC, functional data were acquired using gradient-echo echo-planar imaging (EPI) sequence with the following parameters: TR=2 s, TE=minFull (~25 ms), flip angle=90°, FOV=22 × 22 cm, acquisition matrix 64 × 64, 3-mm slice thickness, 44 axial slices, 180 volumes per run.
Functional images were preprocessed in SPM8 (Wellcome Trust Centre for Neuroimaging, http://www.fil.ion.ucl.ac.uk/spm/) for slice timing correction, image normalization, resampling at a 2 × 2 × 2 mm3 voxel size, and 8-mm Gaussian smoothing kernel. First-level within-subject analysis was performed with a general linear model with four regressors of interest: angry, fearful, and happy face and shape matching. Additional nuisance regressors for six motion parameters were included to correct for motion artifacts. For each participant, contrast images of brain activity were generated for second-level analysis. As processing of both angry and fearful faces has been shown to predict treatment response (Doehrmann et al, 2013; McClure et al, 2007a), we collapsed across these face types to evaluate activation to threatening (ie, angry/fearful) faces vs shapes and activation to non-threatening (ie, happy) faces vs shapes.
Response to treatment
To assess severity of anxiety symptoms pretreatment and posttreatment, participants were administered the Pediatric Anxiety Rating Scale (Research Units of Pediatric Psychopharmacology Anxiety Study Group, 2002). PARS was completed at the initial screening visit (ie, pretreatment anxiety severity) and at the final treatment session (ie, posttreatment anxiety severity). To evaluate comorbid depressive symptoms, participants completed the Children’s Depression Inventory (CDI; Kovacs, 1992) pretreatment and posttreatment. The majority of the current sample (85.4%) was ⩽17 years, and in order to avoid confounding age effects with a different measure, we administered the CDI to all participants.
Data Analysis
To maximize power, whole-brain analyses of predictors of treatment response combined participants from both the SSRI and CBT groups. One-sample t-tests with change in PARS scores as a covariate of interest were performed in SPM8. The primary model focused on associations between treatment response and brain activation to threatening (ie, angry/fearful) faces vs shapes, with secondary analyses examining activation to positive (ie, happy) faces vs shapes. To control for demographic and methodological variables, site/scanner (UM or UIC), treatment (SSRI or CBT), age, and pretreatment PARS were included as covariates in second-level analyses. To correct for multiple comparisons, joint height and extent thresholds were determined within a whole-brain mask excluding cerebellum owing to limited coverage (created with MARINA; Walter et al, 2003) via Monte Carlo simulations (10 000 iterations) and applied to second-level statistical results for a corrected p<0.05 (AlphaSim, AFNI; Cox, 1996). Minimum cluster size for significant effects was 99 voxels for threatening faces and 93 voxels for happy faces at uncorrected p<0.001. To interpret significant effects and for additional post-hoc analyses, activation (beta weights) from a 5-mm sphere around the peak voxel was extracted from individual activity maps using MarsBar (Brett et al, 2002). Exploratory multiple regression analyses were computed to examine treatment variables (ie, site, type of treatment, number of sessions) and clinical variables (ie, primary diagnosis) as moderators of associations between pretreatment brain activation and treatment response.
RESULTS
Participant Characteristics
With regard to clinical disorders, 70.7% of the sample had current diagnoses of GAD, 58.5% social anxiety disorder, and 17.1% separation anxiety disorder. In addition, 7.3% had comorbid panic disorder, 9.8% OCD, 24.4% specific phobia, 2.4% PTSD, 2.4% depression, and 12.2% ADHD. At screening, average PARS scores were in the moderate anxiety severity range for the majority of the sample (53.7%), with 29.3% in the mild range and 17.1% in the severe range. With regard to past treatment, 41.5% of the sample reported receiving some type of psychiatric treatment in the past.
Anxiety severity (ie, PARS) decreased following treatment, t(40)=10.92, p<0.001, mean difference=11.88, as did depressive symptomatology (ie, CDI), t(40)=7.22, p<0.001, mean difference=8.61. With regard to treatment response, 75.6% of the sample responded to treatment and 58.5% showed evidence of remission, as indicated by at least a 35 and 50% decrease in PARS, respectively (Caporino et al, 2013). History of psychiatric treatment, number of sessions, and weeks between screening and posttreatment measures were not significantly related to anxiety severity change (ps>0.17).
Participant characteristics by treatment group and study site are presented in Table 1. The CBT and SSRI groups did not significantly differ on PARS, CDI, age, or distribution of sex, race, or primary diagnosis (ps>0.07), though, as expected, the CBT group completed more sessions than the SSRI group, t(39)=−8.20, p<0.001. Study sites did not significantly differ on treatment modality (UM: n=8 CBT, n=12 SSRI; UIC: n=9 CBT, n=12 SSRI), PARS, CDI, age, number of sessions, or primary diagnoses (ps>0.11). Compared with the sample recruited at UM, the UIC sample included a greater proportion of participants who were Hispanic/Latino, χ2(1)=9.47, p<0.001, and greater proportion of males, χ2(1)=7.84, p<0.01.
Behavioral Performance
Behavioral data was lost for one participant owing to a technical error. Participants showed high accuracy on the task overall (M=93.4%, SD=3.54). Accuracy was higher for happy (M=98.8%; SD=2.70) compared with threatening face (M=91.20%; SD=6.14) and shape matching (M=92.50%; SD=2.81), t(39)=8.39, p<0.001 and t(39)=9.97, p<0.001, respectively. Accuracy for shapes did not significantly differ from threatening faces (p=0.20). Lower accuracy on shapes’ trials was driven by non-responses, particularly when shapes were similar to those in the preceding trial, rather than incorrect responses. Reaction time (RT) was shorter for shapes (M=1331.26; SD=220.38) compared with threatening (M=1872.64; SD=447.17) and happy faces (M=1603.74 SD=431.05), t(39)=−11.17, p<0.001 and t(39)=−6.50, p<0.001, respectively. RT was also shorter for happy compared with threatening faces, t(39)=−7.62, p<0.001.
Partial correlations were computed to evaluate whether RT or accuracy on threatening or happy face trials significantly predicted change in anxiety severity, controlling for age, site, treatment type, and pretreatment PARS. None of the correlations reached significance (ps>0.10).
fMRI Predictors of Treatment Response
Results of models examining associations between activation to threatening and happy faces and change in anxiety severity pretreatment to posttreatment are presented in Table 2. Greater activation in inferior and superior frontal gyri, including dlPFC and vlPFC, and precentral/postcentral gyri to threatening faces predicted better response to treatment (Figure 1). One participant was a significant outlier on extracted values for vlPFC and precentral/postcentral gyri activation to threatening faces according to Grubb’s Test (Grubbs, 1969). Both vlPFC, r(34)=0.43, p<0.01, and postcentral gyrus, r(34)=0.56, p<0.001, continued to predict greater change in anxiety severity with this participant excluded (controlling for site, treatment type, age, and pretreatment PARS). Greater activation in postcentral gyrus during processing of happy faces predicted greater change in symptoms (Figure 2). No regions were negatively associated with change in symptoms (ie, reduced activation predicting greater treatment response) for threatening or happy faces.

Regions of brain activation during processing of threatening faces that predicted greater change in anxiety severity pretreatment to posttreatment; dlPFC,dorsolateral prefrontal cortex; vlPFC,ventrolateral prefrontal cortex; SFG,superior frontal gyrus.

Brain activation during processing of happy faces that predicted greater change in anxiety severity pretreatment to posttreatment.
Exploratory analyses were computed to examine moderators. To limit the number of post-hoc analyses, we focused on dlPFC and vlPFC activation to threatening faces, regions linked to emotion regulation and treatment response in adult anxiety (Ball et al, 2014b; Doehrmann et al, 2013; Kohn et al, 2014). Hierarchical multiple regression analyses were computed predicting change in PARS with age, pretreatment PARS, study site, treatment, number of session, and dlPFC or vlPFC activation in Step 1, followed by dlPFC or vlPFC interactions with site, treatment, and number of sessions in Step 2. No interactions reached significance (ps>0.13). Next the models were analyzed including dummy variables for primary diagnoses of social anxiety disorder and GAD in Step 1 (only three participants had primary separation anxiety disorder diagnoses) and interactions between primary diagnoses and dlPFC or vlPFC activation in Step 2. The main effects of diagnoses (ps>0.56) and interactions (ps>0.41) were not significant. We also evaluated whether dlPFC or vlPFC activation was moderated by age or sex, and none of the interactions were significant (ps>0.17).
DISCUSSION
The current study evaluated brain activation during face processing as a predictor of response to SSRI treatment and CBT in anxious youth. Greater activation in inferior and superior frontal gyri, including vlPFC and dlPFC, and precentral/postcentral gyri during processing of threatening faces predicted better treatment response, as did greater activation in postcentral gyrus during processing of happy faces. We did not find evidence that effects of vlPFC or dlPFC activation on symptom severity were moderated by type of treatment or primary diagnosis, suggesting similar effects across SSRI and CBT, as well as diagnoses of GAD and social anxiety disorder.
Superior and inferior frontal gyri, including vlPFC and dlPFC, are associated with cognitive control and emotional appraisal and regulation (Frank et al, 2014; Gyurak et al, 2011; Kohn et al, 2014; Ochsner and Gross, 2005). Ventral lPFC is thought to signal stimulus salience and need for regulation, while dorsal lPFC implements cognitive control and directs attention in order to modulate emotional responses (Kohn et al, 2014). Youth who demonstrate greater activation in vlPFC and dlPFC prior to treatment may be more effective in regulation of responses to threatening stimuli and thus able to achieve greater therapeutic gains. In support, greater vlPFC activation has been observed in anxious youth compared with healthy controls during fear processing (McClure et al, 2007b), with some evidence that vlPFC activation is negatively related to anxiety severity (Monk et al, 2006) and increases following treatment for anxiety (Maslowsky et al, 2010), possibly reflecting improvements in emotion regulation. Another possibility, however, is that youth with greater vlPFC and dlPFC activation prior to treatment require increased effort to regulate emotions, which may become more automatic following treatment and contribute to greater improvement in symptoms. Future studies that examine how brain activation changes pretreatment to posttreatment are needed to address these questions. It should also be noted that lateral PFC is involved in a range of executive functions (Tanji and Hoshi, 2008), and dlPFC is essential for manipulating information in working memory (Barbey et al, 2013). Thus it is possible that greater lateral PFC activation in the current study corresponds with greater attentional control or ability to maintain the goal of face matching in the presence of threat.
We also found that activation in precentral/postcentral gyri in response to threatening faces and postcentral gyrus activation to happy faces predicted response to treatment. Precentral and postcentral gyri are involved in somatosensory processing and voluntary movement and have also been shown to activate during emotion regulation (Buhle et al, 2014; Goldin et al, 2008; Kohn et al, 2014). Though these regions have previously been related to treatment response in anxious adults (Klumpp et al, 2013; Phan et al, 2013), very little work has examined their precise roles in emotion, and future research is needed in this area in order to better understand how these regions relate to treatment gains. It should be noted that though we did not find evidence that PFC activation to happy faces predicted treatment response, the task included more threatening than happy trials; thus we cannot rule out the possibility that task design limited power to detect effects in other regions in response to happy faces, and future research is needed to evaluate neural processing of positive stimuli as a predictor of treatment response in both adult and pediatric anxiety. Taken together, the current results indicate that greater activation in a broad neural network involved in signaling salience, appraising and regulating emotions predicts better response to treatment among anxious youth.
Although anxious youths exhibit heightened amygdala reactivity to threat (Killgore and Yurgelun-Todd, 2005; McClure et al, 2007b; Thomas et al, 2001), and one previous study demonstrated that greater amygdala predicted better treatment response in a small sample of anxious youth (McClure et al, 2007a), we did not find evidence that amygdala activation predicted treatment response. Prior studies using data-driven approaches have also failed to find amygdala activation as a significant predictor of response to treatment (Ball et al, 2014a), suggesting that pathophysiology, as reflected by abnormal patterns of brain reactivity, may not necessarily serve as predictors of treatment response.
The majority of the current sample (75.6%) showed a ⩾35% reduction in PARS severity, which has been associated with treatment response (Caporino et al, 2013). This rate is higher than response rates observed in large randomized controlled trials of CBT and SSRI in anxious youth (Walkup et al, 2008), likely because the current study focused only on youth who completed treatment and posttreatment clinical measures. Though this design allowed us to examine predictors of response to comparable doses of treatment, additional research is needed to evaluate whether neural measures may be useful in predicting whether individuals will remain engaged in treatment and may be more likely to tolerate one type of treatment over another.
These findings should be interpreted in the context of several limitations. First, though this is the largest study of fMRI predictors of treatment response in anxious youth, our sample size is relatively small when divided by type of treatment (ie, CBT or SSRI). There may be insufficient power to detect interactions with treatment modality, particularly at the whole-brain level. Second, although post-hoc analyses did not reveal that age was a significant moderator, our sample spans a large portion of development and may be underpowered to detect age-related interactions. Second, the sample is heterogeneous with regard to primary diagnoses and only a few participants had primary diagnoses of separation anxiety disorder, though primary diagnoses of social anxiety and GAD did not moderate effects, and the three disorders often co-occur and overlap in symptoms (Mohatt et al, 2014). Finally, although our analysis did not reveal a significant effect of site/scanner as a moderator, the sample was collected and combined from two sites to maximize sample size. Variation based on site due to non-specific factors, including how treatments were assigned (eg, patient preference vs random assignment), could have contributed to the findings. In addition, though there is some evidence that PFC activation during emotional face processing demonstrates adequate test–retest reliability across development (van den Bulk et al, 2013), reliability of activation in other regions, including amygdala, may be weaker (van den Bulk et al, 2013; Plichta et al, 2012). For fMRI measures to be useful in clinical settings, future research is needed to evaluate psychometric properties, including test–retest reliability, in clinical populations.
In conclusion, the current findings suggest that greater reactivity to social signals of threat in brain regions involved in emotion regulation, including dlPFC and vlPFC, predicts better response to treatment in anxious youth. These results provide insight into which children and adolescents are most likely to benefit from treatment, as well as neural processes that contribute to responses to treatment.
References
Ball TM, Stein MB, Paulus MP (2014a). Toward the application of functional neuroimaging to individualized treatment for anxiety and depression. Depress Anxiety 31: 920–933.
Ball TM, Stein MB, Ramsawh HJ, Campbell-Sills L, Paulus MP (2014b). Single-subject anxiety treatment outcome prediction using functional neuroimaging. Neuropsychopharmacology 39: 1254–1261.
Barbey AK, Koenigs M, Grafman J (2013). Dorsolateral prefrontal contributions to human working memory. Cortex 49: 1195–1205.
Brett M, Anton J-L, Valabregue R, Poline J-B (2002). Region of interest analysis using an SPM toolbox. Presented at the 8th International Conference on Funcational Mapping of the Human Brain; 2–6 June 2002; Sendai, Japan. Available on CD-ROM in NeuroImage, Vol 16, No 2.
Buhle JT, Silvers JA, Wager TD, Lopez R, Onyemekwu C, Kober H et al (2014). Cognitive reappraisal of emotion: a meta-analysis of human neuroimaging studies. Cereb Cortex 24: 2981–2990.
Caporino NE, Brodman DM, Kendall PC, Albano AM, Sherrill J, Piacentini J et al (2013). Defining treatment response and remission in child anxiety: signal detection analysis using the pediatric anxiety rating scale. J Am Acad Child Adolesc Psychiatry 52: 57–67.
Compton SN, Walkup JT, Albano AM, Piacentini JC, Birmaher B, Sherrill JT et al (2010). Child/Adolescent Anxiety Multimodal Study (CAMS): rationale, design, and methods. Child Adolesc Psychiatry Ment Health 4: 1.
Copeland WE, Angold A, Shanahan L, Costello EJ (2014). Longitudinal patterns of anxiety from childhood to adulthood: the Great Smoky Mountains Study. J Am Acad Child Adolesc Psychiatry 53: 21–33.
Costello EJ, Egger HK, Angold A (2005). The developmental epidemiology of anxiety disorders: phenomenology, prevalence, and comorbidity. Child Adolesc Psychiatr Clin N Am 14: 631–648.
Cox RW (1996). AFNI: software for analysis and visualization of functional magnetic resonance neuroimages. Comput Biomed Res 29: 162–173.
Doehrmann O, Ghosh SS, Polli FE, Reynolds GO, Horn F, Keshavan A et al (2013). Predicting treatment response in social anxiety disorder from functional magnetic resonance imaging. JAMA Psychiatry 70: 87–97.
Frank DW, Dewitt M, Hudgens-Haney M, Schaeffer DJ, Ball BH, Schwarz NF et al (2014). Emotion regulation: quantitative meta-analysis of functional activation and deactivation. Neurosci Biobehav Rev 45: 202–211.
Fu CHY, Steiner H, Costafreda SG (2013). Predictive neural biomarkers of clinical response in depression: a meta-analysis of functional and structural neuroimaging studies of pharmacological and psychological therapies. Neurobiol Dis 52: 75–83.
Gabrieli JDE, Ghosh SS, Whitfield-gabrieli S (2015). Prediction as a humanitarian and pragmatic contribution from human cognitive neuroscience. Neuron 85: 11–26.
Goldin PR, McRae K, Ramel W, Gross JJ (2008). The neural bases of emotion regulation: reappraisal and suppression of negative emotion. Biol Psychiatry 63: 577–586.
Grubbs FE (1969). Procedures for detecting outlying observations in samples. Technometrics 11: 1–21.
Gyurak A, Gross JJ, Etkin A (2011). Explicit and implicit emotion regulation: a dual-process framework. Cogn Emot 25: 400–412.
Hariri AR, Tessitore A, Mattay VS, Fera F, Weinberger DR (2002). The amygdala response to emotional stimuli: a comparison of faces and scenes. Neuroimage 17: 317–323.
Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P et al (1997). Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry 36: 980–988.
Kendall PC, Choudhury S, Hudson J, Webb A (2002) The C.A.T. Project Workbook. Worbook Publishing: Ardmore, PA, USA.
Kendall PC, Hedtke K (2006) Coping Cat Workbook, 2nd edn. Worbook Publishing: Ardmore, PA, USA.
Killgore WDS, Yurgelun-Todd DA (2005). Social anxiety predicts amygdala activation in adolescents viewing fearful faces. Neuroreport 16: 1671–1675.
Klumpp H, Fitzgerald DA, Phan KL (2013). Neural predictors and mechanisms of cognitive behavioral therapy on threat processing in social anxiety disorder. Prog Neuropsychopharmacol Biol Psychiatry 45: 83–91.
Kober H, Barrett LF, Joseph J, Bliss-Moreau E, Lindquist K, Wager TD (2008). Functional grouping and cortical-subcortical interactions in emotion: a meta-analysis of neuroimaging studies. Neuroimage 42: 998–1031.
Kohn N, Eickhoff SB, Scheller M, Laird AR, Fox PT, Habel U (2014). Neural network of cognitive emotion regulation - an ALE meta-analysis and MACM analysis. Neuroimage 87: 345–355.
Kujawa A, MacNamara A, Fitzgerald KD, Monk CS, Phan KL (2015). Enhanced neural reactivity to threatening faces in anxious youth: evidence from event-related potentials. J Abnorm Child Psychol 43: 1493–1501.
Maslowsky J, Mogg K, Bradley BP, McClure-Tone E, Ernst M, Pine DS et al (2010). A preliminary investigation of neural correlates of treatment in adolescents with generalized anxiety disorder. J Child Adolesc Psychopharmacol 20: 105–111.
McClure EB, Adler A, Monk CS, Cameron J, Smith S, Nelson EE et al (2007a). fMRI predictors of treatment outcome in pediatric anxiety disorders. Psychopharmacology (Berl) 191: 97–105.
McClure EB, Monk CS, Nelson EE, Parrish JM, Adler A, Blair RJR et al (2007b). Abnormal attention modulation of fear circuit function in pediatric generalized anxiety disorder. Arch Gen Psychiatry 64: 97–106.
Merikangas KR, He J-P, Burstein M, Swanson SA, Avenevoli S, Cui L et al (2010). Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication—Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry 49: 980–989.
Mohatt J, Bennett SM, Walkup JT (2014). Treatment of separation, generalized, and social anxiety disorders in youths. Am J Psychiatry 171: 741–748.
Monk CS (2008). The development of emotion-related neural circuitry in health and psychopathology. Dev Psychopathol 20: 1231–1250.
Monk CS, Nelson EE, McClure EB, Mogg K, Bradley BP, Leibenluft E et al (2006). Ventrolateral prefrontal cortex activation and attentional bias in response to angry faces in adolescents with generalized anxiety disorder. Am J Psychiatry 163: 1091–1097.
Nitschke JB, Sarinopoulos I, Oathes DJ, Johnstone T, Whalen PJ, Davidson RJ et al (2009). Anticipatory activation in the amygdala and anterior cingulate in generalized anxiety disorder and prediction of reatment response. Am J Psychiatry 166: 302–310.
Ochsner KN, Gross JJ (2005). The cognitive control of emotion. Trends Cogn Sci 9: 242–249.
Phan KL, Coccaro EF, Angstadt M, Kreger KJ, Mayberg HS, Liberzon I et al (2013). Corticolimbic brain reactivity to social signals of threat before and after sertraline treatment in generalized social phobia. Biol Psychiatry 73: 329–336.
Phillips ML, Drevets WC, Rauch SL, Lane R (2003). Neurobiology of emotion perception. I: The neural basis of normal emotion perception. Biol Psychiatry 54: 504–514.
Plichta MM, Schwarz AJ, Grimm O, Morgen K, Mier D, Haddad L et al (2012). Test-retest reliability of evoked BOLD signals from a cognitive-emotive fMRI test battery. Neuroimage 60: 1746–1758.
Research Units of Pediatric Psychopharmacology Anxiety Study Group (2002). The Pediatric Anxiety Rating Scale (PARS): development and psychometric properties. J Am Acad Child Adolesc Psychiatry 41: 1061–1069.
Tanji J, Hoshi E (2008). Role of the lateral prefrontal cortex in executive behavioral control. Physiol Rev 88: 37–57.
Thomas KM, Drevets WC, Dahl RE, Ryan ND, Birmaher B, Eccard CH et al (2001). Amygdala response to fearful faces in anxious and depressed children. Arch Gen Psychiatry 58: 1057–1063.
van den Bulk B, Koolschijn PCMP, Meens PHF, van Lang NDJ, van der Wee NJA, Rombouts SARB et al (2013). How stable is activation in the amygdala and prefrontal cortex in adolescence? A study of emotional face processing across three measurements. Dev Cogn Neurosci 4: 65–76.
Verduin TL, Kendall PC (2003). Differential occurence of comorbidity within childhood anxiety disorders. J Clin Child Adolesc Psychol 32: 290–295.
Walkup JT, Albano AM, Piacentini J, Birmaher B, Compton SN, Sherrill JT et al (2008). Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. N Engl J Med 359: 2753–2766.
Walter B, Blecker C, Kirsch P, Sammer G, Schienle A, Stark R et al (2003). MARINA: an easy to use tool for the creation of MAsks for Region of INterest Analyses. Presented at the 9th International Conference on Functional Mapping of the Human Brain; 19–22 June 2003; New York, NY, USA. Available on CD-Rom in NeuroImage, Vol. 19, No. 2.
Weems CF, Silverman WK (2013) Anxiety disorders. In: Beauchaine T, Hinshaw S (eds). Child and Adolescent Psychopathology. John Wiley: Hoboken, NJ, USA, pp 513–541.
Whalen PJ, Johnstone T, Somerville LH, Nitschke JB, Polis S, Alexander AL et al (2008). A functional magnetic resonance imaging predictor of treatment response to venlafaxine in generalized anxiety disorder. Biol Psychiatry 63: 858–863.
Whitfield-Gabrieli S, Ghosh SS, Nieto-Castanon A, Saygin Z, Doehrmann O, Chai XJ et al (2015). Brain connectomics predict response to treatment in social anxiety disorder. Mol Psychiatry (e-pub ahead of print).
Woodward LJ, Fergusson DM (2001). Life course outcomes of young people with anxiety disorders in adolescence. J Am Acad Child Adolesc Psychiatry 40: 1086–1093.
Acknowledgements
This work was supported by the National Institute of Mental Health Grant R01-MH086517 to CSM and KLP. AK is supported by the National Institute of Mental Health Grant T32-MH067631 to Mark Rasenick.
Author information
Authors and Affiliations
Corresponding author
PowerPoint slides
Rights and permissions
About this article

Cite this article
Kujawa, A., Swain, J., Hanna, G. et al. Prefrontal Reactivity to Social Signals of Threat as a Predictor of Treatment Response in Anxious Youth. Neuropsychopharmacol 41, 1983–1990 (2016). https://doi.org/10.1038/npp.2015.368
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/npp.2015.368
This article is cited by
-
Quantitative electroencephalographic biomarker of pharmacological treatment response in patients with anxiety disorder: a retrospective study
Scientific Reports (2023)
-
Regional cerebral blood flow as predictor of response to occipital nerve block in cluster headache
The Journal of Headache and Pain (2021)
-
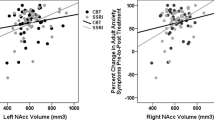
Nucleus accumbens volume as a predictor of anxiety symptom improvement following CBT and SSRI treatment in two independent samples
Neuropsychopharmacology (2020)
-
Cortical Thickness and Subcortical Gray Matter Volume in Pediatric Anxiety Disorders
Neuropsychopharmacology (2017)
