
Abstract
We investigated the effects of nicotine on spatial working memory and spatial selective attention in young, healthy smokers. Spatial working memory was assessed by a delayed response task. Delayed response performance is associated with the integrity of the dorsolateral prefrontal cortex. Spatial interference and negative priming tasks were used to assess spatial selective attention. Nicotine impaired spatial working memory in smokers but it did not affect spatial selective attention. This result suggests that nicotine may impair dorsolateral prefrontal function, as assessed by the spatial working memory task in young smokers and that this deficit does not stem from impairments in spatial selective attention. However, the effects of nicotine on working memory and selective attention in nonsmokers or in psychiatric population with suspected nicotinic receptor abnormalities (e.g., schizophrenia patients) cannot be deduced from the present study.
Similar content being viewed by others
Main
Currently, there is no consensus concerning the effects of nicotine on major cognitive functions. A recent comprehensive review (Heishman et al. 1994) summarizing the effects of nicotine on working memory and selective attention concluded that nicotine enhances selective attention while having no clear effect on working memory. Chronic nicotine infusion causes significant enhancements in working memory in rats (Levin et al. 1996) but in the monkey, cholinergic agonists do not facilitate spatial working memory (Rupniak 1992). In humans, nicotine may leave short term memory unaffected (Jones et al. 1992). Thus, the effects of cholinergic agonists on working memory are not well defined and seem to vary across species. Cholinergic antagonists can disrupt spatial working memory performance (Bartus and Johnson 1976; Rupniak et al. 1991).
On the whole, the effects of nicotine on working memory in humans are poorly understood. One reason might be that nicotine affects cognitive functions via activation of the nicotinic cholinergic receptors but also by its interaction with other neurotransmitter systems. In addition to the effects at cholinergic synapses, nicotine causes the release of dopamine (DA) in the basal ganglia and nucleus accumbens (e.g., Pidoplichko et al. 1997). Thus, nicotine in several brain areas works synergistically with DA (De Belleroche et al. 1979; Lichtensteiger et al. 1982; Clarke and Pert 1985; Imperato et al. 1986; Brazell et al. 1990; Court et al. 1998). Nicotine also interacts with the serotonergic system (Steckler and Sahgal 1995).
Another reason may be that it is difficult to compare nicotinic effects on working memory and attention across different studies because of disparate methodology. This difficulty is compounded by the fact that definitions of attention and working memory vary across these studies. Our aim in this study was to study the effects of nicotine on spatial working memory and spatial selective attention by clearly defining these concepts and by utilizing neurobiologically constrained cognitive probes.
Working memory may be defined as “a system for the temporary holding and manipulation of information” (Baddeley 1986). The dorsolateral prefrontal cortex (DLPFC), as a part of a neural network of cortical and sub-cortical structures, is crucial in mediating working memory (see Goldman-Rakic 1987; Fuster 1995). The neural basis of working memory, especially spatial working memory is well understood. Neurophysiological studies of spatial working memory using the delayed response paradigm (Jacobsen 1935; Fuster 1995), show that a significant proportion of neurons in the DLPFC are involved in the maintenance of spatial information over time (Funahashi et al. 1989, 1990, 1993). The role of DA in spatial working memory has been extensively studied in non-human primates. Its effects on spatial working memory are dependent on the dose and on the receptor type. Spatial working memory is disrupted by a DA D1 antagonist at high concentrations (Sawaguchi and Goldman-Rakic 1991) but it is facilitated by a D1 antagonist at low concentrations (Williams and Goldman-Rakic 1995).
The effects of D2 system on spatial working memory are not clearly understood. Sawaguchi and Goldman-Rakic (1991) observed that D2 antagonists had no significant effects on spatial working memory in the rhesus monkey but Luciana and colleagues (1992) noted a facilitation of spatial working memory in humans by a D2 dopamine agonist, bromocriptine.
Spatial working memory deficits may stem from abnormalities in the frontal cortex which lead to impaired maintenance of information over time (Park and O'Driscoll 1996) but spatial working memory errors may also stem from abnormalities of spatial selective attention and inhibition (Park 1999, in press). Spatial selective attention can be assessed using spatial interference and negative priming tasks. In healthy humans, selective attention in space may be achieved by at least two mechanisms: one involving an excitatory process associated with the target stimulus and the other involving an inhibitory mechanism that is associated with the ignored stimulus. When a stimulus is ignored during a selective attention task, its internal representation is thought to be associated with inhibitory processes. One important consequence of this association is that the inhibitory influences affect the later selection of the ignored stimulus; this is known as ‘negative priming’ (Tipper 1985).
The negative priming paradigm involves exposing subjects to stimuli that are to be ignored initially and later selected. Subjects typically inhibit the ignored stimuli and therefore later, when the ignored stimuli have to be selected, the inhibitory effects increase their response times. Negative priming seems to be independent of visual features of the ignored stimulus (Tipper and Driver 1988), specific motor responses (Tipper et al. 1988), and the modality of tasks (Tipper et al. 1991). In addition, this effect is robust and long-lasting (about 7 seconds), suggesting an active role of inhibition in selective attention.
The idea that exposure to an irrelevant stimulus leads to a deterioration of performance has been studied extensively in rats using the “latent inhibition” paradigm. Latent inhibition is structurally similar to negative priming and indeed, DA agonists abolish both latent inhibition and negative priming while performances on other tasks remain unaffected (see Gray et al. 1991). Limbic system abnormalities, especially those involving the septohippocampal system, abolish latent inhibition and negative priming (see Weiner et al. 1990; Gray et al. 1991; Venables 1992). Taken together, these studies implicate the important role of DA and the limbic system abnormalities, in the disinhibition of attentional processes.
Smoking may interfere with negative priming because nicotine in several brain areas works synergistically with DA (Lichtensteiger et al. 1982; Imperato et al. 1986; De Belleroche et al. 1979). Since there is nicotinic binding on dopaminergic cell bodies in VTA (which projects to the accumbens) and on terminals in the nucleus accumbens (Clarke and Pert 1985) and nicotine increases DA release in the accumbens (Brazell et al. 1990), it is possible that nicotine facilitate a hyperdopaminergic state, which can abolish negative priming. Therefore, we hypothesized that acute nicotine intake may reduce or abolish negative priming but facilitate spatial working memory.
Testing both memory and attention in the same study, with the same participants, is useful because it allows for the analysis of sub-components of information processing. This is especially important in light of the possibility that nicotine may differentially affect different stages of information processing (Stough et al. 1995). Possibility of differential effects in the early and late stages of information processing would be particularly troublesome for a test such as a working memory paradigm with a delayed response design. If a nicotinic effect in accuracy is found, it is unclear whether the effect stems from an impact on memory performance (i.e., maintenance of internal representation in working memory) or from changes in attention at the early part of the task.
One problem with conducting non-invasive human studies involves the selection of the subjects. Often deprived smokers, who abstained from smoking for 8–24 hours are recruited. When the smokers are initially tested (no nicotine condition), they are in a nicotine deficient state. They are, then, typically tested immediately after nicotine intake. Therefore, any observed effect may also be interpreted as the result of performance returning to a non-nicotine-deprived baseline. In other words, any effects on the performance may stem from the withdrawal experienced during the initial testing phase. Thus, the effects of nicotine reported in some studies may simply be the result of restoration of baseline function. In order to address this problem, we decided to test performance during deprivation, following acute administration of nicotine and then during a period of restored baseline level. Testing of both smokers and nonsmokers in the same schedule also allowed for the analysis of any group effects that may indicate chronic effects of nicotine.
METHODS
Participants
Twenty-one smokers (10 females) and 19 nonsmokers (7 females) were recruited from the student population at a private university. There was no difference in the mean ages of the smokers (m = 20.4, s.d. = 1.0), and that of nonsmokers (m = 20.6, s.d. = 1.0) and there was no difference in years of education between the groups (all were seniors at the university). A clinical interview was conducted to rule out DSM Axis 1 disorder. Participants did not have a personal of family history of mental illness nor had a history of head injury or illicit drug use. No participant reported that he/she was currently taking any medication. Smokers had been smoking for an average of 2.9 years (s.d. = 1.3). The mean number of cigarettes smoked per day was 15.6 (s.d. = 5.4). All participants gave written informed consent approved by the Institutional Review Board and were reimbursed for their time.
Design
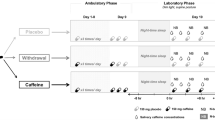
Smokers were asked to abstain from smoking for 24 hours prior to testing. All participants, both smokers and nonsmokers were tested at 9 a.m. The experimenter contacted scheduled subjects at 8 a.m. to ensure that smokers did not accidentally take nicotine in the morning. Those who failed to abstain were re-scheduled. Participants came to the lab at 9 a.m., signed an informed consent form and filled out an information form before cognitive testing. The smokers entered the laboratory in a nicotine deprived state (OFF1 condition). All participants performed three block of testing sequentially within an hour-and-a-half period of time (see Figure 1). Each block took 15–20 minutes to complete.

Procedure for smokers and nonsmokers.
After the first block (A), smokers smoked one cigarette (8 mg nicotine). After nicotine intake, smokers were immediately tested on the second block (B) in this high nicotine state (ON condition). After completing the second block (B), participants waited 15 minutes so that the nicotine could be removed from their system (Block C-OFF2 condition). The Block C-OFF2 condition is important as a gauge of performance under low nicotine levels because the half-life of nicotine in the bloodstream is estimated at 30 min (McKim 1991). Block C was presented more than 30 min after the nicotine intake. During the 15-minute waiting period before the Block C-OFF2 condition, all participants filled out a personality questionnaire so that they were engaged in the same activity.
Nonsmokers followed the same protocol, except that they did not smoke between the first and second blocks. They were asked to wait 15 minutes during which they read a magazine. Between the second and third blocks, they filled out the same questionnaire.
Two experiments were conducted on two separate days, one week apart: spatial working memory and spatial attention tasks. The order of presentation of the two experiments was counterbalanced across subjects. Participants were debriefed after the testing was complete.
Spatial Working Memory Task
Apparatus and Procedure
Participants sat 45 cm from a Macintosh computer screen and a chin rest was used to minimize head movement. The stimulus-display monitor was fitted with a touchscreen (TrollTouch, Valencia, CA). Position accuracy for the touchscreen was better than ±4.6 mm (13 pixels), as measured on a multipoint sampling basis. Calibration involved touching four reference points on the touchscreen and was performed prior to testing.
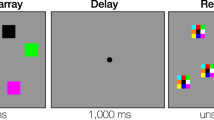
Participants fixated at the center of the screen. When they were ready to begin, the experimenter clicked the mouse to initiate a trial. A target (black circle) then appeared on the screen for 200 milliseconds. Immediately after the target presentation, there was a 30-second delay period, during which the participant performed an intervening subtraction task to prevent verbal rehearsal and to insure continued focus at the center of the screen. For the first two seconds of the delay period a mathematical subtraction operation was displayed in the center of the screen (e.g., 822–7). Participants were asked to continuously reiterate the subtraction of the second number during the delay (e.g., 815, 808, 801, 794 …). Subject's response was recorded by a cassette recorder. This intervening task does not affect spatial working memory performance (Park 1991). After the delay period, eight empty “reference” circles appeared on the screen. Participants were required to touch the remembered location of the target (see Figure 2).

Spatial working memory task.
One block consisted of 32 trials. The order of presentation of trials was counterbalanced across participants. Participants were given practice trials before the first block to ensure that the task was well understood.
Spatial Interference and Negative Priming Tasks
All procedures, designs and stimuli were constructed to approximate Tipper et al.'s experiment 3 (1991) as closely as possible. A Macintosh computer was used. There were four locations on the screen where the target (O) or the distractor (+) could appear. The four positions were placed on the screen so that the horizontal visual angle between the two upper row, outer positions was 8.3 degrees and that between the two lower row, inner positions was 4.3 degrees. The vertical visual angle between the upper outside and lower inside positions was 1.3 degrees. These locations were spatially analogous to the locations of the keys D,C,K, and M on the computer keyboard. Subject used these four keys to indicate the location of the target. The stimuli (O and +) subtended 0.6 by 0.6 degrees of visual angle.
Each trial consisted of a pair of prime and probe displays. Each prime display was always followed by a probe display. Participants were asked to locate the target and ignore the distractor. There were two types of prime displays: with a distractor or with no distractor (see Figure 3). An interference effect is indicated by an increased RT to locate the target in the distractor condition.

Spatial negative priming task.
There were three types of trials, all consisting of pairs of prime and probe displays: control (C), ignored repetition (IR), and neutral (N). The neutral trials contained only the target for both prime and probe displays. In the control (C) trials, the positions of the target and the distractor in the probe and prime displays were all different, whereas in the ignored repetition (IR) trials the location of the target in the probe display was identical to the location of the distractor in the prime display (see Figure 3). Therefore, in the IR probe trials, participants were required to respond to a location that they had previously ignored. A negative priming effect is indicated by longer reaction times (RT's) in the IR probe condition than in the C probe condition.
Participants sat 45 cm from the screen; a chin rest was used to minimize head movement. Participants were told that they must pay attention to the target and ignore the distractor. They were asked to indicate the location of the target (O) by pressing the corresponding key on the keyboard and to ignore the distractor (+). They were asked to identify the target as quickly and as accurately as possible. Participants initiated each block of trials by focusing at the center of the screen and then pressing the spacebar. A trial began with the prime display, which stayed on the screen until the participant responded to it by locating the target. Then, there was a 1350 ms pause before the second display (probe) was presented. During the final 800 ms of the pause, the fixation point appeared at the center to prepare participant for the next response. When the participant responded to the probe display by locating the target, a pattern mask was presented and it stayed on the screen.
When ready for the next trial, the participant pressed the space bar, after which there was always a 6.4 sec period. Therefore, there was always a rest period of at least 6.4 sec and, in practice, the inter-trial interval was about 8–10 sec. This lengthy inter-trial interval was necessary because Tipper et al. (1991) reported that a negative priming effect may last up to about 7 sec and we wanted to insure the dissipation of residual priming effects between trials. During the final 800ms of the pause, a fixation point was presented in the center of the screen to prepare participants for the next prime display (see Figure 4 for a schematic diagram of the procedure).

Procedure for the spatial negative priming task.
There were 72 trials (i.e., 72 pairs of prime and probe displays) in each block. Participants were allowed a brief rest after every 18 trials. Each block took about 16–20 minutes to complete. The order of presentation of different conditions was randomized within each block. Participants were given practice trials before the beginning of the experiment.
RESULTS
A repeated measures ANOVA was conducted to compare the group differences at three testing blocks: A(OFF1), B(ON) and C(OFF2). Further contrast analyses were performed when necessary.
Spatial Working Memory
The accuracy (% correct) of working memory and the response times (ms) were analyzed. A response was scored as correct only if the participant touched within 1.5 degree of the center of the target position and if the finger moved there directly. If the finger moved to a wrong position first, and then later moved to the correct target position, this response was counted as incorrect.
Accuracy
There was a statistically significant main effect of group (F(1,38) = 4.48, p < .04). Overall, the smokers performed worse on the spatial working memory task (m = 81.0%, s.d. = 14.7) than did the nonsmokers (m = 87.7% s.d. = 9.0). There was no significant main effect of the testing blocks (F(2,76) = 1.99, p > .14) but there was a significant group-by-testing block interaction (F(2,76) = 8.41, p < .0005). Smokers and nonsmokers performed almost identically at initial testing block A(OFF1); compare 86.6% (s.d. = 11.7) for smokers with 85.5% (s.d. = 8.3) for nonsmokers. Nonsmokers’ performance improved slightly and did not change subsequently in blocks B (89.5%, s.d. = 8.9) and C (88.2%, s.d. = 9.9). However, smokers’ performance deteriorated to 77.7% (s.d. = 13.2) after the nicotine intake in block B(ON) and remained impaired in block C(OFF2) at 78.6% (s.d. = 16.1) (see Figure 5).

Effect of nicotine on spatial working memory.
Contrast analyses showed that on Block A, the two groups did not differ (F(1,38) = 1.53, p > .22) but on Block B, the smokers were significantly impaired compared with the controls (F(1,38) = 7.05, p < .01) and this group difference was still present on Block C (F(1,38) = 3.99, p < .05).
Response Times
There was a significant group differences in the response times of the correct trials (F(1,38) = 8.6, p < .006). Smokers (m = 1413 ms, s.d. = 342) tended to be slower overall than nonsmokers (m = 1183 ms, s.d. = 153). There was also a main effect of the testing blocks (F(2,76) = 3.2, p < .05). Both smokers and controls became faster on successive blocks (1348 ms for block A, 1290 ms for block B, and 1273 ms for block C). But there was no interaction between the group and the testing blocks (F(2,76) = 0.34, p > .96).
Spatial Interference and Negative Priming
Smokers and nonsmokers were compared on three measures: location detection, spatial interference, and spatial negative priming. The detection was indexed by the RT to locate a single target in the display in ‘prime’ trials (i.e., the first trial of each prime-probe pair for the neutral condition). The interference effect was obtained from the prime trials. The RT to detect a single target (neutral trials) was compared with that for detecting a target in the presence of a distractor. The negative priming effect was indexed by examining the RTs of probe trials following the presentation of the prime trials. The RT to detect a target at a position previously occupied by a distractor was expected to be slowed down. The ignored repetition (IR) condition was compared with the control (C) condition in the probe trials.
Baseline RT to Detect a Single Target
The neutral condition consisted of trials with a single target for detection. Therefore, the mean RTs for the neutral condition in the prime trials were taken as an index of the baseline RT. There were no errors in locating the target in the neutral trials. A repeated measures ANOVA showed that there was a main effect of the group (F(1,38) = 6.9, p < .02). Smokers (m = 411ms, s.d. = 58) were slower than the nonsmokers (m = 374ms, s.d. = 36). There was a significant main effect of the testing block (F(2,76) = 34.1, p < .0001). The RTs to detect the target decreased for both smokers and nonsmokers. But there was no group-by-testing block interaction (F(2,76) = 0.83, p > .43). The decrease in RTs across the three testing blocks is not likely to be caused by nicotine action alone and instead, may reflect a practice effect (see Figure 6).

Effect of nicotine on the response times to locate a target.
Spatial Interference Effect: Concurrent Inhibition of Distractor
Reaction time (RT) to locate the target in the prime trial was the variable of interest. The accuracy in locating the target was above 99%. Trials in which the target was not located correctly were excluded in the computation of the interference score.
Interference effect refers to the difference in RTs to locate the target in the neutral trials (single target) compared with when the stimulus display consisted of the target AND the distractor. The concurrent presence of the distractor was expected to increase the RT's for detecting the target. A raw interference score was calculated by averaging the mean RT for prime trials with target and distractor and then subtracting the mean RT's of prime trials with single target. Interference effect is indicated by score greater than zero. Because there is a group difference in the baseline RT, we calculated the percent interference score to account for the possible individual differences in Rts: % Interference Score = 100 × (Raw Interference Score / RT for neutral prime trials).
There was no main effect of the group (F(1,38) = 1.80, p > .18). The smokers and the non smokers did not differ significantly on their ability to ignore the concurrent distractor. There was no main effect of the testing blocks (F(2, 76) = 1.07, p < . 34). There was no interaction between the group and the testing blocks (F(2, 76) = 1.45, p > . 24). Smokers did not experience different degree of spatial interference compared with nonsmokers, suggesting that the concurrent inhibition of distractors is not altered by chronic or acute nicotine intake (see Figure 7).

Effect of nicotine on spatial interference.
Spatial Negative Priming: Latent Inhibition of Distractor
Reaction time (RT) to locate the target in the probe trial was the variable of interest. The accuracy in locating the target was above 97%. Trials in which the target was not located correctly for either the prime or probe display were not included in the computation of the negative priming score.
Negative priming scores were computed by comparing the RT's of the probe displays of the ignored repetition trials and the RT's of the probe displays of the control trials. A raw negative prime score was first calculated by subtracting the mean RT of ignored repetition probe trials from the main RT of control probe trials. A negative raw score indicates the presence of negative priming, whereas a positive raw score indicates absence of negative priming (disinhibition). To account for differences in baseline RT's, we computed a percent negative prime score as follows: % Negative Prime Score = (Raw Negative Prime Score / RT for Control Probe Trials) × 100.
The means are presented in Figure 8. A repeated measures ANOVA showed that there was no main group effect (F(1,38) = 0.35, p > .56) nor a significant interaction between group and the testing blocks (F(2,76) = 1.76, p > .17) for the % Negative Prime Scores. There was no significant main effect of the testing blocks (F(2,76) = 0.50, p > .60).

Effect of nicotine on spatial negative priming.
DISCUSSION
We investigated the effects of nicotine on spatial working memory and spatial attentional inhibition. Our hypothesis was that nicotine, as a cholinergic agonist and an indirect DA agonist (e.g., Wonnacott 1989), would facilitate working memory while impairing spatial negative priming. Contrary to our hypothesis, acute nicotine intake impaired spatial working memory, at least temporarily. Smokers, after abstaining for 24 hours and controls did not show any deficits in spatial working memory function. But, after acute nicotine intake (block B(ON)), smokers performed significantly worse than the nonsmokers, and this impairment persisted for more than 30 minutes afterwards, as indicated by their continued working memory deficit in block C(OFF). Although it is not possible to unequivocally state that there was a dose-response nicotinic effect across the blocks B and C, we were able to compare the effect sizes. The effect size of the group differences in working memory performance was larger for block B (d = 0.38) than for block C (d = 0.22) and close to zero for block A (d = 0.08). Since we did not assess working memory function at later times after block C, we are unable to extrapolate our data further. However, within the confines of the study design, our results suggest that, in smokers, acute nicotine intake may impair spatial working memory.
Although it is unclear why acute nicotine intake impairs working memory, one hypothesis is that nicotine may increase proactive interference (Dunnett and Martel 1990). Proactive interference in the spatial working memory task could occur with prior target locations interfering with memory for subsequent target locations, thereby increasing perseverative errors. In our data, we did not observe a statistically significant increase in perseverative errors after nicotine intake but this hypothesis should be systematically tested in future studies by varying the inter-trial intervals.
Although nicotine impaired spatial working memory, it did not have a detrimental effect on spatial selective attention. Nicotine had no significant impact on the spatial interference effect; both smokers and nonsmokers were faster at localizing the target when the target appeared alone than when a distractor was presented simultaneously but there was no group difference. Similarly, nicotine did not affect spatial negative priming. Thus, the deficit in spatial working memory was not accompanied by abnormalities in spatial selective attention mechanisms. This result suggests that acute nicotine intake may impair prefrontal mechanisms without affecting neural systems that mediate spatial selective attention. We expected nicotine intake to impair negative priming because nicotine in several brain areas works synergistically with DA and acute nicotine intake causes a hyperdopaminergic state. One reason why we did not find nicotinic effects on spatial negative priming may be that we tested chronic smokers. Chronic smoking is associated with a loss of high affinity binding of nicotinic receptors and reduced activity of the DA neurons (Court et al. 1998).
There are several limitations to our study: 1) We were not able to measure blood serum or urinary level nicotinic or DA metabolites and we could not examine effects of nicotine intake on nonsmokers, for ethical reasons. Therefore, extrapolation of our results to nonsmokers, which could be relevant for secondary smoking concerns, must await further study; and 2) We did not assess the level of subjective withdrawal from nicotine after abstinence and after nicotine intake so we cannot rule out the possibility that the smokers may have performed better than nonsmokers if they had been examined when they were smoking at their habitual rate. On the other hand, we tested smokers 30 minutes after the nicotine intake (block C) when they are less likely to be experiencing withdrawal; at this point, smokers still showed working memory deficits without any impairments in spatial selective attention.
To summarize, we found detrimental effects of acute nicotine administration after 24-hour abstinence on spatial working memory in healthy young smokers. At the same time, these subjects showed intact spatial selective attention. However, the effects of nicotine on working memory and selective attention in nonsmokers or in psychiatric population with suspected nicotinic receptor abnormalities (e.g., schizophrenia patients) cannot be deduced from the present study.
References
Baddeley AD . (1986): Working Memory. NY, Oxford University Press
Bartus RT, Johnson HR . (1976): Short-term memory in the rhesus monkey: Disruption from the anti-cholinergic scopolamine. Pharmacol Biochem Behav 5 (1): 39–46
Brazell MP, Mitchell SN, Gray JA . (1990): Acute administration of nicotine increases the in vivo extracellular levels of DA, 3,4-dihyddroxyphenylacetic acid and ascorbic acid preferentially in the nucleus accumens of the rat: Comparison with caudate putamen. Neuropharmacology 29: 1177–1185
Clarke PBS, Pert A . (1985): Autoradiographic evidence for nicotine receptors on nigrostriatal and mesolimbic dopaminergic neurons. Brain Res 348: 355–358
Court JA, Lloyd S, Thomas N, Piggott MA, Marshall EF, Morris CM, Lamb H, Perry PH, Johnson M, Perry EK . (1998): Dopamine and nicotinic receptor binding and the levels of dopamine and homovanillic acid in human brain related to tobacco use. Neuroscience 87 (1): 63–78
De Belleroche J, Lugmini Y, Bradford HF . (1979): Evidence for presynaptic cholinergic receptors on dopaminergic terminals: Degeneration studies with 6-hydroxydopamine. Neurosci Lett 11: 209–213
Dunnett SB, Martel FL . (1990): Proactive interference effects on short-term memory in rats. I. Basic parameters and drug effects. Behav Neurosci 104 (5): 655–665
Funahashi S, Bruce CJ, Goldman-Rakic PS . (1989): Mnemonic coding of visual cortex in the monkey's dorsolateral prefrontal cortex. J Neurophysiol 61 (2): 331–348
Funahashi S, Bruce CJ, Goldman-Rakic PS . (1990): Visuospatial coding in primate prefrontal neurons revealed by oculomotor paradigms. J Neurophysiol 63: 814–831
Funahashi S, Bruce CJ, Goldman-Rakic PS . (1993): Dorsolateral prefrontal lesion and oculomotor delayed-response performance: Evidence for mnemonic “scotomas.” J Neurosci 13 (4): 1479–1497
Fuster JM . (1995): Memory in the cortex of the primate. Biol Res 28 (1): 59–72
Goldman-Rakic PS . (1987): Circuitry of primate prefrontal cortex and regulation of behavior by representational knowledge. In Plum F, Mountcastle V (eds), Handbook of Physiology—The nervous system. V. Bethesda, MD, American Physiological Society, pp 373–417
Gray JA, Feldon J, Rawlins JNP, Hemsley DR, Smith AD . (1991): The neuropsychology of schizophrenia. Behav Brain Sci 14: 1–84
Heishman SJ, Taylor RC, Henningfield JE . (1994): Nicotine and moking: A review of effects on human performance. Exp Clin Psychopharmacol 2: 345–395
Imperato A, Mulas A, Di Chiara G . (1986): Nicotine preferentially stimulates dopamine relase in the limbic system of freely moving rats. Eur J Pharmacol 132: 337–338
Jacobsen CF . (1935): Studies of cerebral functions in primates. I. The functions of the frontal association areas in monkeys. Compar Psychol Monogr 13: 3–60
Jones GM, Sahakian BJ, Levy R, Warburton DM, Gray JA . (1992): Effects of acute subcutaneous nicotine on attention, information processing and short-term memory in Alzheimer's disease. Psychopharmacology 108 (4): 485–494
Levin ED, Kim P, Meray R . (1996): Chronic nicotine working and reference memory effects in the 16-arm radial maze: Interactions with D1 agonist and antagonist drugs. Psychopharmacology 127: 25–30
Lichtensteiger W, Hefti F, Felix D, Huwyler T, Melamed E, Schlumpf M . (1982): Stimulation of nigrostriatal dopamine neurons by nicotine. Neuropharmacology 21: 963–968
Luciana M, Depue RA, Arbisi P, Leon A . (1992): Facilitation of working memory in humans by a D2 dopamine receptor agonist. J Cogn Neurosci 4 (1): 58–68
McKim WA . (1991): Drugs and Behavior. Englewood Cliffs NJ, Prentice Hall, pp 160–183
Park S . (1991): The role of prefrontal cortex in spatial working memory deficits of schizophrenic patients. Doctoral Dissertation. Boston, MA, Harvard University
Park S, O'Driscoll GA . (1996): Components of working memory deficit in schizophrenia. In Matthysse SW, Levy DL, Kagan J, Benes F (eds), Psychopathology: The Evolving Science of Mental Disorder. NY, Cambridge University Press, pp 34–50
Park S . (1999): Spatial working memory function in schizophrenia. In Spitzer M, Maher BA (eds), Experimental Psychopathology. NY, Cambridge University Press, in press.
Pidoplichko VI, DeBiasi M, Williams JT, Dani JA . (1997): Nicotine activates and desensitizes midbrain dopamine neurons. Nature 390 (6658): 401–404
Rupniak NMJ, Samson NA, Tye SJ, Field MJ, Iversen SD . (1991): Evidence against a specific effect of cholinergic drugs on spatial memory in primates. Behav Brain Res 43 (1): 1–6
Rupniak NMJ . (1992): Profile of cholinomimetic drugs in primates: Status of screens for potential Alzheimer therapies. Drug Dev Res 27: 77–88
Sawaguchi T, Goldman-Rakic PS . (1991): D1 Dopamine receptors in prefrontal cortex: Involvement in working memory. Science 251: 947–950
Steckler T, Sahgal A . (1995): The role of serotonergic-cholinergic interactions in the mediation of cognitive behavior. Behav Brain Res 67: 165–199
Stough C, Mangan G, Bates T, Frank N, Kerkin B, Pellett O . (1995): Effects of nicotine on perceptual speed. Psychopharmacology 119 (3): 305–310
Tipper SP . (1985): The Negative priming effect: Inhibitory priming by ignored objects. Q J Exp Psychol 37A: 571–590
Tipper SP, MacQueen GM, Brehaut JC . (1988): Negative priming between response modalities: Evidence for the central locus of inhibition in selective attention. Percep Psychophysics 43: 45–52
Tipper SP, Driver J . (1988): Negative priming between pictures and words: Evidence for semantic analysis of ignored stimuli. Memory Cogn 16: 64–70
Tipper SP, Weaver B, Cameron S, Brehaut J, Bastedo J . (1991): Inhibitory mechanisms of attention in identification and localization tasks: Time course and disruption. J Exp Psychol: Learn Memory Cogn 17 (4): 681–692
Venables PH . (1992): Hippocampal function and schizophrenia. Experimental psychological perspective. Ann NY Acad Sci 658: 111–127
Weiner I, Shofel A, Feldon J . (1990): Disruption of latent inhibition by low dose of amphetamine is antagonized by haloperidol and apomorphine. J Psychopharmacol 4: 255
Williams GV, Goldman-Rakic PS . (1995): Modulation of memory fields by dopamine D1 receptor in prefrontal cortex. Nature 376: 572–575
Wonnacott S . (1989): Nicotinic involvement in ACh-DA interaction? Trends Pharmacol Sci 10 (10): 395–396
Acknowledgements
This research was supported in part by NIMH, NARSAD, and the Scottish Rite Schizophrenia Research Program.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Park, S., Knopick, C., McGurk, S. et al. Nicotine Impairs Spatial Working Memory while Leaving Spatial Attention Intact. Neuropsychopharmacol 22, 200–209 (2000). https://doi.org/10.1016/S0893-133X(99)00098-6
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1016/S0893-133X(99)00098-6
Keywords
This article is cited by
-
An exploratory, randomised, crossover study to investigate the effect of nicotine on cognitive function in healthy adult smokers who use an electronic cigarette after a period of smoking abstinence
Harm Reduction Journal (2024)
-
Working memory- and anxiety-related behavioral effects of repeated nicotine as a stressor: the role of cannabinoid receptors
BMC Neuroscience (2013)
-
The effects of psychotomimetic and putative cognitive-enhancing drugs on the performance of a n-back working memory task in rats
Psychopharmacology (2009)
-
Dose-Related Enhancement of Mood and Cognition in Smokers Administered Nicotine Nasal Spray
Neuropsychopharmacology (2008)
-
A double-blind placebo-controlled experimental study of nicotine: II—Effects on response inhibition and executive functioning
Psychopharmacology (2007)
