
Abstract
Paediatric solid tumours arise from endodermal, ectodermal, or mesodermal lineages1. Although the overall survival of children with solid tumours is 75%, that of children with recurrent disease is below 30%2. To capture the complexity and diversity of paediatric solid tumours and establish new models of recurrent disease, here we develop a protocol to produce orthotopic patient-derived xenografts at diagnosis, recurrence, and autopsy. Tumour specimens were received from 168 patients, and 67 orthotopic patient-derived xenografts were established for 12 types of cancer. The origins of the patient-derived xenograft tumours were reflected in their gene-expression profiles and epigenomes. Genomic profiling of the tumours, including detailed clonal analysis, was performed to determine whether the clonal population in the xenograft recapitulated the patient’s tumour. We identified several drug vulnerabilities and showed that the combination of a WEE1 inhibitor (AZD1775), irinotecan, and vincristine can lead to complete response in multiple rhabdomyosarcoma orthotopic patient-derived xenografts tumours in vivo.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 51 print issues and online access
$199.00 per year
only $3.90 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others

References
Chen, X., Pappo, A. & Dyer, M. A. Pediatric solid tumor genomics and developmental pliancy. Oncogene 34, 5207–5215 (2015)
Smith, M. A., Altekruse, S. F., Adamson, P. C., Reaman, G. H. & Seibel, N. L. Declining childhood and adolescent cancer mortality. Cancer 120, 2497–2506 (2014)
van de Wetering, M. et al. Prospective derivation of a living organoid biobank of colorectal cancer patients. Cell 161, 933–945 (2015)
Boj, S. F. et al. Organoid models of human and mouse ductal pancreatic cancer. Cell 160, 324–338 (2015)
Gao, D. et al. Organoid cultures derived from patients with advanced prostate cancer. Cell 159, 176–187 (2014)
Townsend, E. C. et al. The Public Repository of Xenografts enables discovery and randomized phase ii-like trials in mice. Cancer Cell 30, 183 (2016)
Bruna, A. et al. A biobank of breast cancer explants with preserved intra-tumor heterogeneity to screen anticancer compounds. Cell 167, 260–274 (2016)
Klco, J. M. et al. Functional heterogeneity of genetically defined subclones in acute myeloid leukemia. Cancer Cell 25, 379–392 (2014)
Gao, H. et al. High-throughput screening using patient-derived tumor xenografts to predict clinical trial drug response. Nat. Med. 21, 1318–1325 (2015)
Zarzosa, P. et al. Patient-derived xenografts for childhood solid tumors: a valuable tool to test new drugs and personalize treatments. Clin. Transl. Oncol. 19, 44–50 (2017)
Stewart, E. et al. The Childhood Solid Tumor Network: a new resource for the developmental biology and oncology research communities. Dev. Biol. 411, 287–293 (2016)
Ernst, J. & Kellis, M. ChromHMM: automating chromatin-state discovery and characterization. Nat. Methods 9, 215–216 (2012)
Hafner, M., Niepel, M., Chung, M. & Sorger, P. K. Growth rate inhibition metrics correct for confounders in measuring sensitivity to cancer drugs. Nat. Methods 13, 521–527 (2016)
Stewart, E. et al. Targeting the DNA repair pathway in Ewing sarcoma. Cell Reports 9, 829–840 (2014)
Langenau, D. M., Sweet-Cordero, A., Wechsler-Reya, R. & Dyer, M. A. Preclinical models provide scientific justification and translational relevance for moving novel therapeutics into clinical trials for pediatric cancer. Cancer Res. 75, 5176–5186 (2015)
Chen, X. et al. Targeting oxidative stress in embryonal rhabdomyosarcoma. Cancer Cell 24, 710–724 (2013)
Chen, X. et al. Recurrent somatic structural variations contribute to tumorigenesis in pediatric osteosarcoma. Cell Reports 7, 104–112 (2014)
Pinto, E. M. et al. Genomic landscape of paediatric adrenocortical tumours. Nat. Commun. 6, 6302 (2015)
Tirode, F. et al. Genomic landscape of Ewing sarcoma defines an aggressive subtype with co-association of STAG2 and TP53 mutations. Cancer Discov. 4, 1342–1353 (2014)
Benjamini, Y. & Hochberg, Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J. R. Stat. Soc. B 57, 289–300 (1995)
Campbell, I. Chi-squared and Fisher–Irwin tests of two-by-two tables with small sample recommendations. Stat. Med. 26, 3661–3675 (2007)
Richardson, J. T. The analysis of 2 × 2 contingency tables—yet again. Stat. Med. 30, 890 (2011)
Ritz, C. et al. Bioassay analysis using R. J. Stat. Softw. 12, 5 (2005)
R Core Team. R: a language and environment for statistical computing (R Foundation for Statistical Computing, 2012)
Do, K. et al. Phase I study of single-agent AZD1775 (MK-1775), a Wee1 kinase inhibitor, in patients with refractory solid tumors. J. Clin. Oncol. 33, 3409–3415 (2015)
Liang, X. et al. Evaluation of homogenization techniques for the preparation of mouse tissue samples to support drug discovery. Bioanalysis 3, 1923–1933 (2011)
Reece, D. E. et al. Pharmacokinetic and pharmacodynamic study of two doses of bortezomib in patients with relapsed multiple myeloma. Cancer Chemother. Pharmacol. 67, 57–67 (2011)
Atadja, P. Development of the pan-DAC inhibitor panobinostat (LBH589): successes and challenges. Cancer Lett. 280, 233–241 (2009)
Xie, C. et al. Panobinostat enhances cytarabine and daunorubicin sensitivities in AML cells through suppressing the expression of BRCA1, CHK1, and Rad51. PLoS ONE 8, e79106 (2013)
Ocio, E. M. et al. In vitro and in vivo rationale for the triple combination of panobinostat (LBH589) and dexamethasone with either bortezomib or lenalidomide in multiple myeloma. Haematologica 95, 794–803 (2010)
Acknowledgements
We thank A. McArthur for editing the manuscript. This work was supported by Cancer Center Support (CA21765), grants to M.A.D. from the National Institutes of Health (EY014867, EY018599, and CA168875), and American Lebanese Syrian Associated Charities. M.A.D. was also supported by the Howard Hughes Medical Institute, Alex Lemonade Stand, Tully Family and Peterson Foundations. E.S. was supported by the St. Baldrick’s Foundation and the National Pediatric Cancer Foundation.
Author information
Authors and Affiliations
Contributions
E.S. and M.A.D. designed the study and wrote the paper. S.F. wrote and supervised the protocol. X.C. and B.X. performed all computational analyses. C.B., B.G., V.H., M.O., K.B., and J.D. assisted with preclinical animal studies and cell screening. J.E. assisted with molecular analyses. M.C. and A.B. provided pathology review. B.F. performed pharmacokinetic analysis. J.W. performed biostatistics. N.T. and A.S. analysed drug sensitivity data. A.K. manages the Childhood Solid Tumour Network and assisted with drug screening. X.Z. developed the protein paint visualization. E.R.M., R.K.W., J.D., J.Z., A.P., and M.A.D. are part of the St Jude’s Children’s Health Research Hospital–Washington University Pediatric Cancer Genome Project.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Additional information
Reviewer Information Nature thanks P. Lichter, D. Weinstock and the other anonymous reviewer(s) for their contribution to the peer review of this work.
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data figures and tables
Extended Data Figure 1 O-PDX models retain the cellular features of the corresponding patient tumours.
a–d, Micrographs of H&E-stained patient tumours and corresponding O-PDX tumours for a representative rhabdomyosarcoma (a), liposarcoma (b), osteosarcoma (c), and neuroblastoma (d). e, Immunohistochemical staining for synaptophysin (brown) for SJNBL013761_D and the matched O-PDX. f–i, Transmission electron micrographs of a representative rhabdomyosarcoma (f), neuroblastoma (g), liposarcoma (h), and osteosarcoma (i). Inset for each micrograph is a higher magnification view of a key cellular hallmark of each tumour. HA, hydroxyapatite. Scale bars, a–e 40 μm; f–i 2 μm.
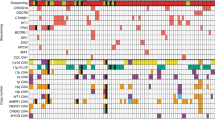
Extended Data Figure 2 O-PDX tumours retain the genomic features of the patient tumours.
a–d, Heat maps of the 51 tumours that had sufficient material for whole-genome sequencing and whole-exome sequencing analyses. Individual O-PDX/patient tumour pairs are indicated by alternating grey and white columns. Heat maps are grouped on the basis of the disease: rhabdomyosarcoma (a), osteosarcoma (b), neuroblastoma (c), and rare tumours (d).
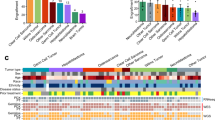
Extended Data Figure 3 Molecular and cellular clonal heterogeneity.
a, Boxplot of the correlation coefficient (R) between each O-PDX and the corresponding patient tumour. The error bars represent 1.5× the interquartile range. b–d, Scatterplots for the gene-expression correlation coefficients for the patient tumour compared with the O-PDX relative to the patient tumour purity determined from whole-genome sequencing. The Pearson correlation between those two variables is indicated for each tumour type. The line of best fit for the data is shown (red). e, f, Diagram and scatterplot of the clonal changes in SJOS001132 between the patient tumour and the O-PDX. The proportion of proliferating cells as measured by Ki67 immunostaining and dying cells as measured by cleaved caspase 3 immunostaining. The patient tumour had a major clone with two clusters of SNVs (C1 and C2) that then continued to evolve and diverge in the O-PDX into two distinct clones. One clone contained the original SNVs found in the patient tumour (C1 and C2) and the other clone had an additional cluster of SNVs (C3). The total number of SNVs analysed in this sample was 238. g, H&E staining of the patient tumour and the O-PDX showing an expansion of cells with more aggressive pleiomorphic cellular features. h, i, Diagram and scatterplot of the clonal changes in SJNBL124 between the patient tumour and the O-PDX. The proportion of proliferating cells as measured by Ki67 immunostaining and dying cells as measured by cleaved caspase 3 immunostaining. The patient tumour had a major clone (80% of the tumour) with one cluster of SNVs (C1) and a minor clone (20% of the tumour) with two clusters of SNVs (C1 and C2). In the O-PDX, the minor clone was lost and the tumour continued to evolve and acquired an additional cluster of SNVs (C3). The total number of SNVs analysed in this sample was 373. j, In the H&E-stained patient tumour, there was a major clone (90% of the tumour) with proliferating small round cells and a minor clone (10% of the tumour) that had features of differentiated neuroblastoma cells. The cells with features of differentiated cells were lost in the O-PDX.
Extended Data Figure 4 Epigenetic landscape reflects cellular origins.
a, Heat map of the HMM states used in this study. b, Stack histogram of the percentage of each of the 16 HMM states for the genes expressed specifically in rhabdomyosarcoma across the 3 tumour types (osteosarcoma, neuroblastoma, rhabdomyosarcoma). c, Representative HMM and expression of a gene (MYOG) that is specifically expressed in rhabdomyosarcoma. d, e, Corresponding ChIP–seq peaks for all 12 antibodies and the input sample for the MYOG promoter in the rhabdomyosarcoma and osteosarcoma O-PDXs. f, Stack histogram of the percentage of each of the 16 HMM states for the genes expressed specifically in neuroblastoma across the 3 tumour types (osteosarcoma, neuroblastoma, rhabdomyosarcoma). g, Representative HMM and expression of a gene (PHOX2B) that is specifically expressed in neuroblastoma. h, i, Corresponding ChIP–seq peaks for all 12 antibodies and the input sample for the PHOX2B promoter in the neuroblastoma and rhabdomyosarcoma O-PDXs.
Extended Data Figure 5 Drug screening quality control.
a, Box plot for the Z′ score for each of the 1,911 plates screened in this study that passed our quality control metrics. Most cell models (O-PDXs and cell lines) had a Z′ score above 0.4 (red line). The average Z′ was 0.57 and 95% of plates had Z′ between 0.27 and 0.82. The error bars represent 1.5× the interquartile range. b, Scatterplot of AUC for the dose–response curves for pairs of drugs with similar and dissimilar mechanisms. Larger AUC values represent greater drug potency (killing). The Pearson correlation is shown for each drug pair. c, Scatterplot of AUC for the dose–response curve for two MEK inhibitors (trametinib and selumetinib). The cell models highlighted in red have mutations in the RAS/NF1/MEK pathway.
Extended Data Figure 6 Preclincial pharmacokinetics and in vivo preclinical phase II.
a–c, Concentration–time curves for panobinostat, bortezomib, and AZD1775 in mice bearing O-PDX tumours. Each data point is the mean and standard deviation of triplicate animals. The pharmacokinetics for IRN and VCR had been determined previously. d, Outline of the schedule used for the combination of panobinostat with bortezomib, VCR + IRN as the standard of care and AZD1775 + VCR + IRN. The schedules were selected to match that used in patients and the dose was selected to provide the same plasma exposure based on the pharmacokinetics in a–c. e–g, Tumour response for individual SJRHB000026_X1 mice on the preclinical phase II study for placebo-treated mice and each of the three treatment groups. Each line indicates an individual mouse with tumour. h, Stack bar plots of the response percentages for three different RMS O-PDX models with standard of care for recurrent RMS (IRN + VCR) and the AZD1775 + VCR + IRN treatment regimen. The numbers of mice in each response category are indicated on the plot.
Supplementary information
Supplementary Information
This file contains a Supplementary Discussion and additional references. (PDF 271 kb)
Supplementary Table 1
Characteristics of patient tumor samples. Basic clinical information on the patient tumor samples is provided in addition to the time to initial engraftment and time to passage for a subset of those samples. One tab has all patients and the other tab has those that engrafted and are cryopreserved for distribution. (XLSX 27 kb)
Supplementary Table 2
Histopathologic and electron microscopic analysis of patient tumors and matched O-PDXs. Pediatric solid tumor pathologists reviewed the histopathology of the individual patient tumors and matched O-PDXs. Immunohistochemical staining was also scored for the majority of those that had samples available. In the 2nd tab, specific subcellular features characteristic of each type of tumor were scored from electron microscopic images for the O-PDX and the patient tumor when sample was available. Electron microscopy is not routinely performed for pediatric solid tumors so availability of patient tumor is limited. Antibody information is provided in the 3rd tab. (XLSX 23 kb)
Supplementary Table 3
Analysis of single nucleotide variations and indels in patient tumors and matched O-PDXs. 4 tables are provided on separate tabs for the mutations identified in patient tumor or O-PDX for each pair of samples. (XLSX 466 kb)
Supplementary Table 4
Clonal analysis of O-PDXs relative to corresponding patient tumors and sublines, multiple passages and treated tumors. The number of single nucleotide variants analyzed and the clonal score grouping is provided for each patient/O-PDX pair. Three additional tabs are included with the clonal analysis of the passaged tumors, the sublines and the treated samples. (XLSX 52 kb)
Supplementary Table 5
RNA-seq and epigenetic analysis. Four separate tabs are included with correlation analysis for RNA-seq between the O-PDX and matched patient tumor. The boxes are color coded based on correlation coefficient with red being high correlation and blue being lower correlation. The genes that were up or downregualted in individual tumor types relative to all others were used for pathway analysis. Those genes were also correlated with H3K27me3 at the promoter in the tumors that had low expression in individual tabs based on tumor type. (XLSX 276 kb)
Supplementary Table 6
High throughput drug screening data. Three tabs are provided that summarize the drug screening experiments. One tab has a legend explaining the analysis. The 2nd tab has the drug sensitivity calculations without growth rate correction and the 3rd is growth rate corrected. A tab with plating density and growth medium for drug screening is also provided. (XLSX 2809 kb)
Supplementary Table 7
Preclinical phase II data. Individual tabs for each O-PDX with raw preclinical phase II data for each mouse at each timepoint. (XLSX 24 kb)
Supplementary Table 8
Preclincial phase III data. Individual tabs for each O-PDX with raw preclinical phase III data for each mouse at each timepoint. (XLSX 41 kb)
Rights and permissions
About this article

Cite this article
Stewart, E., Federico, S., Chen, X. et al. Orthotopic patient-derived xenografts of paediatric solid tumours. Nature 549, 96–100 (2017). https://doi.org/10.1038/nature23647
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nature23647
This article is cited by
-
Hallmark discoveries in the biology of Wilms tumour
Nature Reviews Urology (2024)
-
Establishment of a high-fidelity patient-derived xenograft model for cervical cancer enables the evaluation of patient’s response to conventional and novel therapies
Journal of Translational Medicine (2023)
-
Temporal chromatin accessibility changes define transcriptional states essential for osteosarcoma metastasis
Nature Communications (2023)
-
Refined high-content imaging-based phenotypic drug screening in zebrafish xenografts
npj Precision Oncology (2023)
-
Genomic profiling of subcutaneous patient-derived xenografts reveals immune constraints on tumor evolution in childhood solid cancer
Nature Communications (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
