
Abstract
Distal common bile duct carcinoma is a poorly characterized entity for reasons such as variable terminology and difficulty in determining site of origin of intrapancreatic lesions. We compared clinicopathologic features of pancreatobiliary-type adenocarcinomas within the pancreas, but arising from the distal common bile duct, with those of pancreatic and ampullary origin. Upon careful review of 1017 pancreatoduodenectomy specimens with primary adenocarcinoma, 52 (5%) qualified as intrapancreatic distal common bile duct carcinoma. Five associated with an intraductal papillary neoplasm were excluded; the remaining 47 were compared to 109 pancreatic ductal adenocarcinomas and 133 ampullary carcinomas. Distal common bile duct carcinoma patients had a younger median age (58 years) than pancreatic ductal adenocarcinoma patients (65 years) and ampullary carcinoma patients (68 years). Distal common bile duct carcinoma was intermediate between pancreatic ductal adenocarcinoma and ampullary carcinoma with regard to tumor size and rates of node metastases and margin positivity. Median survival was better than for pancreatic ductal adenocarcinoma (P=0.0010) but worse than for ampullary carcinoma (P=0.0006). Distal common bile duct carcinoma often formed an even band around the common bile duct and commonly showed intraglandular neutrophil-rich debris and a small tubular pattern. Poor prognostic indicators included node metastasis (P=0.0010), lymphovascular invasion (P=0.0299), and margin positivity (P=0.0069). Categorizing the tumors based on size also had prognostic relevance (P=0.0096), unlike categorization based on anatomic structures invaded. Primary distal common bile duct carcinoma is seen in younger patients than pancreatic ductal adenocarcinoma or ampullary carcinoma. Its prognosis is significantly better than pancreatic ductal adenocarcinoma and worse than ampullary carcinoma, at least partly because of differences in clinical presentation. Use of size-based criteria for staging appears to improve its prognostic relevance. Invasive pancreatobiliary-type distal common bile duct carcinomas are uncommon in the West and have substantial clinicopathologic differences from carcinomas arising from the pancreas and ampulla.
Similar content being viewed by others

Main
Cholangiocarcinoma, which accounts for ~3% of all gastrointestinal cancers, has an incidence of ~5000 new cases per year in the United States,1 although incidence per capita is several times higher in many Eastern countries.2, 3 While the World Health Organization uses the term ‘cholangiocarcinoma’ only to refer to intrahepatic malignancies of biliary epithelial origin,4 other authors have used the term to encompass extrahepatic bile duct adenocarcinomas as well.5 These extrahepatic tumors have traditionally been divided into upper, middle, and lower categories,5 although considering that middle bile duct tumors are rare and are often treated the same as either upper or lower tumors, some authors have advocated eliminating the category and designating cholangiocarcinomas as either intrahepatic, perihilar, or distal.6, 7 Regarding extrahepatic lesions, perihilar/upper are the most common, followed by distal, with the nebulous middle lesions the least common.6, 8, 9 Whereas proximal and perihilar cholangiocarcinomas may be amenable to hepatic resection, surgically treatable distal tumors require pancreatoduodenectomy.
Although carcinomas of extrahepatic bile ducts are well analyzed in the East, their frequency and clinicopathologic associations in Western countries have been less thoroughly analyzed, particularly in the pathology literature. For example, the reported frequency of bile duct origin among what are called ‘periampullary carcinomas’ (mostly referring to carcinomas removable by pancreatoduodenectomy) ranges from 5 to 17%,10, 11, 12 and this variation is most likely due to definitional differences. Moreover, distinguishing intrapancreatic distal common bile duct carcinoma from pancreatic ductal adenocarcinoma and ampullary adenocarcinoma is often a challenge both clinically and pathologically, as there is significant anatomic and histologic overlap. Furthermore, distal common bile duct carcinoma can be subtle on gross examination and can secondarily involve the main pancreatic duct and/or the ampulla. Additionally, secondary involvement of the common bile duct is very common in pancreatic ductal adenocarcinoma; in our experience, 97% of pancreatic ductal adenocarcinomas show invasion into the intrapancreatic common bile duct. As a result, there has unsurprisingly been variation in the clinicopathologic characteristics of these entities reported in different studies, and many cases of these three carcinomas may have been incorrectly classified.
To address these issues, we performed a detailed pathologic review of 1017 pancreatoduodenectomy specimens with invasive adenocarcinoma by using more refined criteria in the classification of these tumors,13 along with a comparative clinicopathologic analysis distinguishing intrapancreatic distal common bile duct carcinoma cases from pancreatic ductal adenocarcinoma and ampullary carcinoma.
Materials and methods
With appropriate Institutional Review Board approval, we performed a review of 1017 pancreatoduodenectomy specimens with the primary diagnosis of invasive adenocarcinoma, all resected in the United States; these specimens had been previously compiled into a computerized archive. Clinical history, gross photographs, available slides, and original signout report were all used to classify the tumors, with the original diagnoses overturned in some instances. During this process, distal common bile duct carcinoma was defined as a carcinoma either grossly or microscopically centered unequivocally around the intrapancreatic common bile duct (Figure 1). Cases where the site of origin was not entirely clear, but was most likely the common bile duct (e.g., >75% of the tumor oriented around the bile duct) were also classified as distal common bile duct carcinoma. Dubious cases (e.g., tumor halfway involving the pancreatic duct and halfway involving the distal common bile duct, or tumors causing biliary-type symptoms clinically but primarily sparing the common bile duct grossly) were excluded. The exact number of diagnoses changed during this process was not recorded.

Pancreatic ductal adenocarcinoma (red), ampullary carcinoma (blue), and distal common bile duct carcinoma (green) all arise within close proximity to one another and can therefore overlap in terms of the anatomic space they occupy. Furthermore, pancreatic ductal adenocarcinoma can secondarily involve the ampulla or common bile duct, and ampullary carcinoma and distal common bile duct carcinoma can similarly invade structures from which they did not originate. Careful consideration of the size, epicenter, presentation, and histology of each lesion should allow for accurate diagnosis.
Fifty-two cases (5%) met the inclusion criteria. Five cases associated with an intraductal papillary neoplasm of the bile duct (the biliary counterpart of pancreatic intraductal papillary mucinous neoplasm)4, 14, 15, 16 were excluded to eliminate potentially confounding factors; all five were conventional adenocarcinomas and were from four men and one woman. The remaining 47 cases came from Emory University, Atlanta, Georgia (33 cases); Wayne State University, Detroit, Michigan (13 cases); and Piedmont Hospital, Atlanta, Georgia (1 case). Slides from these cases were reviewed by three of the authors (RSG, PB, NVA). The morphology of each tumor was scrutinized, with an emphasis on various patterns of growth and differentiation, as well as factors that might distinguish them from pancreatic ductal adenocarcinoma or ampullary carcinoma. Biliary intraepithelial neoplasia was noted when present, and anomalous anatomy of the biliary tree was documented if identified. Margin and node status, presence or absence of lymphovascular and perineural invasion, and tumor stage were all reappraised.
Appropriate data for comparative analysis, including patient survival, was available for a separate cohort of 109 pancreatic ductal adenocarcinomas in our database. All cases, which were removed by pancreatoduodenectomy in the United States, were conventional pancreatobiliary-type adenocarcinomas arising within the pancreas. To eliminate confounding factors, colloid-type and intraductal papillary mucinous neoplasm-associated cases were excluded from the analysis, as these have been shown to be different biologically from ordinary pancreatobiliary-type adenocarcinomas.17, 18 Malignancies other than adenocarcinoma were also excluded. Appropriate data for comparative analysis was also available for a separate cohort of 133 ampullary carcinomas with pancreatobiliary-type morphology in our database. Only cases with predominantly pancreatobiliary-type histology were included in this group, to have a more fair and uniform comparison with pancreatic ductal adenocarcinoma and distal common bile duct carcinoma.
The following clinicopathologic parameters were compared among the distal common bile duct carcinoma, pancreatic ductal adenocarcinoma, and ampullary carcinoma groups: patient age and sex, tumor size, presence of positive surgical margins and lymph node metastases, and clinical outcome. Data on distant metastases were missing from a majority of pancreatic ductal adenocarcinoma cases, precluding the use of this variable. Cases were not controlled for postoperative therapy, but there was no particular bias toward a specific treatment protocol based on the classification. Differences among the groups were assessed by analysis of variance (patient age and tumor size), χ2 (patient sex, margin status, and metastases), and log-rank (survival) tests. Multivariable regression was conducted using Cox proportional hazard models to compare the predicted survival among the three tumor groups, independent of other factors. The proportional hazard assumption was tested for all variables using log–log survival curves. The final model was created using backward elimination to retain only the variables that were statistically significant predictors of survival.
Within the distal common bile duct carcinoma group, independent factors potentially associated with survival, including tumor size, margin and node status, perineural and lymphovascular invasion, and American Joint Committee on Cancer T-classification and stage,19 were analyzed using Wald tests from unadjusted Cox models. To compare the predictive utility of certain factors, the Schwarz Bayesian criteria and C-index were calculated as measures of goodness of fit and discriminatory power. Lymph node harvesting results using two different methods were compared using an unpaired t-test. All tests were two-sided, and statistical significance was defined as P-value <0.05. Statistical analyses were performed using SAS v.9.3 (SAS Institute, Cary, NC).
Results
Table 1 shows clinicopathologic comparisons among the distal common bile duct carcinoma, pancreatic ductal adenocarcinoma, and ampullary carcinoma groups.
Clinical Findings in Distal Common Bile Duct Carcinoma
The 47 distal common bile duct carcinoma patients included 26 men and 21 women, with a median age at resection of 58 years (range 39–80). This was younger than the pancreatic ductal adenocarcinoma patients (median age 65 years; P=0.0576) and significantly younger than the ampullary carcinoma patients (median age 68 years; P=0.0018). Patient ethnicity was not available, but all were treated in a Western hospital, and only one patient had a name that could be construed as indicating Eastern heritage.
Clinical history was available for review on 70% of the patients (33/47). The most common clinical symptom was jaundice, with 27/33 patients initially presenting with it (82%) and three more developing it during their clinical course. Other symptoms indicating biliary obstruction, such as scleral icterus, pruritis, dark urine, and light stools, were reported by 14 patients (42%), including two of the patients who did not develop jaundice. Other common symptoms included abdominal pain (14/33, 42%), weight loss (13/33, 39%), diarrhea (5/33, 15%), nausea (5/33, 15%), and vomiting (4/33, 12%). Imaging was available for 68% of the patients (32/47) and depicted a stricture of the distal biliary system in half (16/32, 50%). The other patients were interpreted as having a biliary mass (10/32, 31%) or a pancreatic mass (6/32, 19%); the 6 with a ‘pancreatic mass’ only underwent computed tomography. The combined clinical and imaging findings led to the correct diagnosis preoperatively in all 33 patients. None of the cases was known to have any association with biliary parasites or demonstrable pancreatobiliary duct malunion, and only one had a documented choledochal cyst.
Pathologic Findings in Distal Common Bile Duct Carcinoma
The distal common bile duct carcinomas had a median size of 2.5 cm (range: 1.0–5.8 cm), a lymph node metastasis rate of 61%, and a positive margin rate of 23%. The retroperitoneal margin was the most frequently involved (6/44, 14%), with the common bile duct (3/44, 7%) and vascular bed (1/44, 2%) margins sometimes involved. As with prognosis (see below), all three of these figures placed distal common bile duct carcinoma directly in between pancreatic ductal adenocarcinoma and ampullary carcinoma; these relationships were statistically significant for median size and margin positivity rate, but not quite for lymph node metastasis rate (see Table 1). Lymphovascular invasion was observed in 40% of cases.
The median number of lymph nodes examined per case was 16. A specific form of lymph node harvesting (the ‘orange-peeling’ approach)20 had been used in 62% of the cases, and the median number of nodes identified by this method was 19, vs 6 in cases not ‘orange-peeled’ (performed before this approach had been instituted) (P<0.0001). The median number of involved nodes in node-positive cases was 3. Thirteen patients (28%) had documented distant metastases, with the liver the most commonly involved site.
Four cases showed cystic duct–common bile duct union within the pancreas (‘low union’), with the tumor immediately distal to this abnormal junction (Figures 2a and b); this anomaly was observed in one man and three women.

(a) In four of our distal common bile duct carcinoma cases, the common hepatic duct and cystic bile duct did not join until both were within the pancreas, creating a short and entirely intrapancreatic common bile duct. We refer to this phenomenon as ‘low union’ of the ducts. (b) A pancreatoduodenectomy specimen demonstrating low union. Green ink and green arrow denote cystic duct; yellow ink and yellow arrow denote common hepatic duct.
Most distal common bile duct carcinomas (41/47; 87%) were pT3 by the current American Joint Committee on Cancer criteria (7th Edition) at resection, with 3/47 (6%) being pT1 and 3/47 being pT2. No T-classification or other staging comparison was performed between distal common bile duct carcinoma and the pancreatic ductal adenocarcinoma or ampullary carcinoma cases, as the staging parameters used for these three sites are vastly different, are mostly arbitrary, present significant challenges in their application, and are undergoing revision.21, 22, 23, 24, 25, 26
Given the retrospective nature of the study and the fact that the 47 distal common bile duct carcinomas came from multiple different institutions, gross approach to the pancreatoduodenectomy specimens was not uniform. Still, valuable information could be gleaned from most of the gross descriptions: Distal common bile duct carcinomas were often subtle, scirrhous, constrictive lesions forming circumferential plaque-like thickening of the common bile duct wall in a lunar or semilunar pattern (Figure 3a). In some cases, however, evidence of malignancy was limited to friability and erythema of the duct mucosa. Gross examination failed to detect subtle carcinoma in a few cases.

(a) This pancreatoduodenectomy specimen demonstrates a distal common bile duct carcinoma forming a constrictive lesion that surrounds and tracks along the common bile duct within the pancreas. It also extends partially into the main pancreatic duct and the ampulla; however, the tumor epicenter is at the common bile duct. (b) This pattern of spread can also be observed microscopically. (c) This carcinoma instead traverses just underneath the common bile duct surface, occasionally penetrating it. Intraepithelial neoplasia is not present in this portion of the duct. (d) Distal common bile duct carcinoma morphologically resembles typical pancreatobiliary-type adenocarcinomas in most cases.
Microscopically, distal common bile duct carcinoma often formed an even band around the common bile duct (Figure 3b), which could be particularly striking in the pancreas-neighboring aspects of the duct. Careful analysis in these situations revealed more infiltrative foci, especially in the posterior aspect of the common bile duct, where soft tissue is immediately adjacent. In two cases, the carcinoma tracked along the common bile duct microscopically, traveling just underneath the epithelium but occasionally penetrating into the main duct lumen (Figure 3c). The tumor often secondarily involved pancreatic ducts and mimicked high-grade pancreatic intraepithelial neoplasia, underscoring the need for careful gross examination in establishing the precise site of tumor origin.
The infiltrative glands in distal common bile duct carcinoma closely resembled those of pancreatic ductal adenocarcinoma, namely one or two layers of cuboidal cells forming small lumens (Figure 3d). In cases of well-differentiated carcinoma, infiltration was at times subtle and hard to distinguish from surrounding normal duct structures. Perineural invasion was a common finding (92%), as it is in pancreatic ductal adenocarcinoma.
Compared with typical pancreatic ductal adenocarcinoma morphology, distal common bile duct carcinoma more commonly showed intraglandular neutrophil-rich debris and a smaller tubular pattern. Other histologic patterns focally observed in otherwise pancreatobiliary-type distal common bile duct carcinoma included a tubulolobular pattern akin to that of invasive lobular carcinoma of the breast (2/47 cases, 4%; Figure 4a); a microglandular pattern reminiscent of mesonephric remnants (7/47, 15%; Figure 4b); a vacuolated cell pattern, as documented recently in pancreatic ductal adenocarcinoma27 (2/47, 4%; Figure 4c); a clear-cell or foamy gland appearance (2/47, 4%; Figure 4d); an intestinal-like pattern that demonstrated goblet cells (3/47, 6%; Figure 4e); medullary morphology (1/47, 2%; Figure 4f); and prominent papilla formation within the invasive glands (1/47, 2%).

Morphologic variants of otherwise pancreatobiliary-type distal common bile duct carcinoma. (a) Tubulolobular features, reminiscent of mammary carcinoma, (b) microglandular features with intraluminal acidophilic secretions (‘mesonephric’ pattern), (c) vacuolated features, (d) clear-cell and foamy gland features, (e) intestinal-type features, and (f) medullary features.
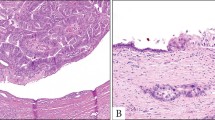
The common bile duct mucosa showed what could be interpreted as high-grade biliary intraepithelial neoplasia28 in 28 cases (60%), although it was impossible to determine whether these lesions represented true intraepithelial neoplasia or duct cancerization. This finding was often present only focally, although large portions of the common bile duct epithelium were denuded in virtually every specimen (presumably secondary to stenting and/or manipulation of the gross specimen), potentially removing evidence of an intraepithelial component in some cases. While biliary intraepithelial neoplasia was mostly of the simple, flat type, five cases (11%) demonstrated a micropapillary pattern (Figure 5a), and in one case, it took on an intestinal appearance, mimicking low- and high-grade dysplasia from a colonic tubular adenoma (Figure 5b). One case demonstrated multifocal biliary intraepithelial neoplasia along the entire intrapancreatic common bile duct.

(a) High-grade biliary intraepithelial neoplasia growing in a micropapillary pattern. (b) Biliary intraepithelial neoplasia simulating intestinal-type low- and high-grade dysplasia.
Incidental findings noted during analysis of the distal common bile duct carcinoma cases included several foci of pancreatic intraepithelial neoplasia. Most foci were low-grade pancreatic intraepithelial neoplasia, which is known to be a common incidental finding in pancreata,29 although two patients had small foci of severely atypical cells well away from the primary tumor, raising the differential of high-grade pancreatic intraepithelial neoplasia vs spread of the carcinoma to the pancreatic ducts. Other incidental observations, each seen in one case, included pancreas divisum, squamoid cyst of the pancreatic duct, duodenal lymphangioma, duodenal well-differentiated neuroendocrine tumor, and traumatic neuroma adjacent to and involved by the carcinoma.
Outcome
Factors associated with worse clinical outcome in distal common bile duct carcinoma included tumor size (P=0.0402), lymph node metastases (P=0.0010), lymphovascular invasion (P=0.0299), and margin positivity (P=0.0069). Perineural invasion did not affect patient survival (P=0.2204) but was only absent in four cases.
Grouping the distal common bile duct carcinomas according to American Joint Committee on Cancer T-classification was not significantly related to survival (P=0.1575). However, stratifying the carcinomas into three groups based on maximum tumor dimension (size <2, 2–4 cm, and >4 cm) was strongly associated with survival, as patients with larger tumors fared worse (P=0.0096). This result held when comparing the two groups using the Schwarz Bayesian criteria, which is a type of information criteria used in model selection as a measure of goodness of fit; the Schwarz Bayesian criteria was 186.23 for American Joint Committee on Cancer T-classification and 183.73 for size stratification, with a lower Schwarz Bayesian criteria indicating a better fit of the model. However, when using the C-index, which is a measure of model discrimination created as an extension of the receiver-operating characteristic that can be applied to survival data, American Joint Committee on Cancer T-classification was a better fit than size stratification (0.8389 and 0.8149, respectively, with a higher C-index indicating better predictive ability). Therefore, two of three comparisons favored size stratification over American Joint Committee on Cancer T-classification.
In a similar vein, a ‘modified American Joint Committee on Cancer’ system, where the three aforementioned size cutoffs were used in place of the American Joint Committee on Cancer definitions for pT1/pT2/pT3, better predicted patient outcome than non-modified staging. The modified system had a P-value of 0.0030, a Schwarz Bayesian criteria of 188.06, and a C-index of 0.7145, all of which were more favorable than the non-modified American Joint Committee on Cancer system (P-value of 0.0086, Schwarz Bayesian criteria of 191.04, C-index of 0.7023).
Follow-up data was available for 45 patients (median: 18 months; range: 0–157 months). Seven were alive at last follow-up (median: 36 months). One was still alive 114 months after surgery, and two of the deceased survived for 157 and 104 months; such survival lengths are almost unheard of in pancreatic ductal adenocarcinoma.30
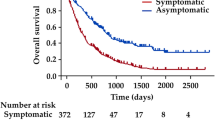
The 1-, 3-, 5-year, median survival, and log-rank test all showed increased survival for distal common bile duct carcinoma patients compared with pancreatic ductal adenocarcinoma patients (P=0.0010) and worse survival compared with ampullary carcinoma patients (P=0.0006) (Figure 6). In the multivariable analysis including all three groups, factors significantly impacting survival included older age (P=0.0107), margin involvement (P=0.0008), and nodal disease (P<0.0001). These characteristics were retained in the final model. Using this adjusted model and patients with ampullary carcinomas as the reference group, the hazard ratio for patients with distal common bile duct carcinoma was 2.3 (P=0.0005), and the hazard ratio for patients with pancreatic ductal adenocarcinoma was slightly lower, at 2.1 (P=0.0041).

Kaplan–Meier survival curves for ampullary carcinoma, distal common bile duct carcinoma, and pancreatic ductal adenocarcinoma. Patients with distal common bile duct carcinoma fared worse than patients with ampullary carcinoma (P=0.0006) but better than patients with pancreatic ductal adenocarcinoma (P=0.0010, log-rank test).
Discussion
There have been several impediments in the literature to characterizing the clinicopathologic features of distal common bile duct carcinoma. Classification and terminology of cholangiocarcinomas have varied over time; currently, most accepted schemes use ‘distal’ common bile duct carcinoma synonymously with ‘intrapancreatic cholangiocarcinoma,’ although tumors arising outside the pancreas but within the distal extrapancreatic common bile duct are considered distal common bile duct carcinomas as well and usually are surgically approached with pancreatoduodenectomy.6 Overall, distal common bile duct carcinoma appears to be the most straightforward and encompassing term for these tumors. The argument over whether these extrahepatic tumors are ‘cholangiocarcinomas’ or ‘adenocarcinomas’ is beyond the scope of this project, hence the use of ‘distal common bile duct carcinoma’ for our cohort of cases removed by pancreatoduodenectomy.
Although cholangiocarcinoma overall is not an especially rare diagnosis in Western countries, it appears far more prevalent in Eastern countries, mostly attributable to association with parasites.2, 3 Accordingly, many studies dealing with the clinicopathologic aspects of distal common bile duct carcinoma have been from Japan,8, 31, 32, 33, 34, 35, 36 Korea,37 and China.9 Recently, certain groups in the United States have described and analyzed series of this entity as well.7, 10, 38, 39 However, many of these studies lumped distal common bile duct carcinoma in with proximal cases and/or did not include pathologic review, meaning they may well have included cases of pancreatic ductal adenocarcinoma and ampullary carcinoma masquerading as distal common bile duct carcinoma. Our rigorous efforts to exclude intrapancreatic cancers of non-biliary origin may explain why only 5% of the adenocarcinomas in our pancreatoduodenectomies were distal common bile duct carcinomas, whereas other studies have found rates of 12%10 to 17%.11
Known clinical risk factors for ‘cholangiocarcinoma’ include parasites, primary sclerosing cholangitis, choledochal cysts, Thorotrast exposure, viral hepatitis, and possibly choledocholithiasis.3, 36, 40 Our study observed a previously unrecognized factor that may also be important in the pathogenesis of distal common bile duct carcinoma: union of the cystic duct and common hepatic duct within the pancreas. In these cases, the cystic duct, rather than joining with the common hepatic duct just distal to the hepatic hilum, traveled separately toward the pancreas, entered it, and joined the common hepatic duct there, creating a short, entirely intrapancreatic common bile duct. While several anomalous configurations of the biliary tree have been described,5 this appears to be a relatively unexplored phenomenon that we refer to as ‘low union’ of the extrahepatic biliary system.41 As biliary carcinoma can arise in anatomic abnormalities such as pancreatobiliary maljunction42 and bile duct duplication,43 we suspect that low union can contribute to the development of intrapancreatic malignancy. The incidence of low union in the general population is unknown. As more careful grossing protocols are adopted,41 its true incidence and potential role in tumorigenesis may become better appreciated.
Clinically, as demonstrated in this study, many distal common bile duct carcinoma patients present with symptoms related to biliary obstruction; as a result, they tend to present earlier than patients who have an intrahepatic biliary lesion.40 However, intrapancreatic distal common bile duct carcinoma may present with more stereotypically pancreatic symptoms, such as pain, abdominal fullness, early satiety, and weight loss.4, 40, 44
Radiologic techniques, such as computed tomography, magnetic resonance imaging, and endoscopic retrograde cholangiopancreatography, can help determine the site of origin of an intrapancreatic lesion.5, 45 However, pancreatic head lesions cannot always be localized correctly preoperatively.5 In our study, proper synthesis of clinical and imaging data allowed for a diagnosis of distal common bile duct carcinoma to be made before surgery in each case.
For cases where the preoperative diagnosis is unclear or in question, careful gross examination of the pancreatoduodenectomy specimen is essential and should be standardized as much as possible.41 The epicenter of the gross lesion should be considered, as well as what structures are involved and in what manner. Some distal common bile duct carcinomas are obviously distinct from pancreatic ductal adenocarcinoma, as they involve the common bile duct in a circumferential manner, forming a constrictive lesion that spreads along the duct lengthwise. Less overt cases can be challenging, especially considering that pancreatic ductal adenocarcinoma secondarily invades the common bile duct in the vast majority of cases. However, it would be unusual in our experience for pancreatic ductal adenocarcinoma to involve the common bile duct circumferentially rather than in a haphazard, disorganized manner. Accordingly, a recent study reported that intrapancreatic tumors symmetrically/concentrically involving the common bile duct are likely to be distal common bile duct carcinomas, whereas asymmetric/eccentric involvement generally implies a pancreatic ductal adenocarcinoma.38 Large tumors that destroy all the surrounding anatomic structures are also most likely to be pancreatic ductal adenocarcinoma, as it is the more common tumor and the more likely to be large in size at the time of resection, primarily because it does not cause jaundice as readily as distal common bile duct carcinoma. Nebulous tumors that could have possibly arisen from one of several structures based on their anatomic location (e.g., those with the epicenter right at the junction of the common bile duct and ampulla) require methodical microscopic analysis of the ductal system for intraepithelial neoplasia, as well as careful correlation with clinical and radiologic findings. Furthermore, pancreatic ductal adenocarcinoma and distal common bile duct carcinoma are similar histologically; while our study found that intraluminal neutrophils were often seen in distal common bile duct carcinomas, they can occasionally be seen in pancreatic ductal adenocarcinoma as well.46
In some instances, unfortunately, it may well be impossible to classify an intrapancreatic tumor correctly, calling the prognosis of the patient and the stage of the tumor into question.47 We found that distal common bile duct carcinoma has significantly longer survival than pancreatic ductal adenocarcinoma and significantly shorter survival than ampullary carcinoma. Other studies have reached similar conclusions regarding the relative prognosis of these three tumors, and many found that tumor type is an independent prognostic indicator on multivariable analysis.10, 11, 12, 35 It should be noted that, unlike other studies, we have included only carcinomas of pancreatobiliary-type morphology in our cohorts, and we have also excluded adenocarcinomas arising from an intraductal papillary mucinous neoplasm or an intraductal papillary neoplasm of the bile duct. Comparison of these purified categories disclosed a potentially important facet of these carcinomas: On multivariable analysis, we found that pancreatic ductal adenocarcinoma has a hazard ratio of 2.1 compared with ampullary carcinoma, whereas distal common bile duct carcinoma has a hazard ratio of 2.3. This suggests that distal common bile duct carcinoma is intrinsically as aggressive as pancreatic ductal adenocarcinoma, if not more so. This is not necessarily surprising, as distal common bile duct carcinoma and pancreatic ductal adenocarcinoma are both conventional pancreatobiliary-type adenocarcinomas and are very similar to each other. Distal common bile duct carcinoma likely has an overall better prognosis because it manifests relatively early (due to common bile duct obstruction) and is therefore discovered at a lower stage. Still, the higher hazard ratio of distal common bile duct carcinoma may be related to either a more aggressive inherent biology or to the fact that distal common bile duct carcinoma has ready access to the peritoneal cavity and may spread more easily than recognized by clinical or pathologic evaluation.
Criteria for tumor staging also differ among the three entities. At the time of this writing, the American Joint Committee on Cancer Cancer Staging Manual is on its 7th Edition. This edition, in addition to a classification for pancreas (endocrine and exocrine) lesions, has a separate classification for distal bile duct tumors,19 whereas the 6th Edition included distal bile duct lesions in its chapter on all extrahepatic bile duct tumors. In the 7th Edition, invasion of the pancreas by distal common bile duct carcinoma is classified as pT3, whereas invasion of only the pancreas in pancreatic ductal adenocarcinoma is pT1 or pT2, depending on size. Hong et al25, 26 have taken issue with this approach of staging distal biliary malignancy by involvement of nearby structures. They note that the anatomy of the extrahepatic bile duct wall is variable throughout its length, making distinction between pT1 tumors (confined to the bile duct) and pT2 tumors (invading beyond the bile duct wall but not into adjacent organs) difficult, if not impossible. They also found no survival difference between American Joint Committee on Cancer pT2 and pT3 carcinomas. Instead, they proposed a classification based entirely on depth of invasion, with 5 and 12 mm of spread from the common bile duct epithelial surface offered as cutoff points with statistically significant differences in prognosis.25, 26 As the distal common bile duct carcinoma cases in our study were not grossed in a uniform manner, we were unable to perform the same careful, goal-directed analysis that Hong’s group did. Still, we similarly found that the current American Joint Committee on Cancer T-classification did not correlate with prognosis. Instead, we found that size-based criteria—stratifying distal common bile duct carcinoma cases by greatest dimension (<2, 2–4, and >4 cm), as has been proposed for pancreatic ductal adenocarcinoma23—correlated significantly with prognosis, both in isolation and as a substitute for American Joint Committee on Cancer T-classification. These results, in conjunction with Hong’s, indicate that a size-based T-classification system is appropriate for staging distal common bile duct carcinomas. In any case, the size of an invasive carcinoma should be documented in the surgical pathology report and taken into consideration in assessing the prognosis of a given patient. Of note, some surgical studies have reported that size is not an independent prognostic factor, but those studies analyzed extrahepatic bile duct tumors as a whole.7, 8, 9
In addition to tumor size, we found that lymphovascular invasion and nodal metastases significantly impact prognosis in distal common bile duct carcinoma. The lymphatic system supplying the distal biliary tree drains to lymph nodes around the head of the pancreas, making harvesting of the nodes in a pancreatoduodenectomy specimen appropriate for distal common bile duct carcinoma.48 Many of the aforementioned studies also found that node status7, 8, 9, 31, 32, 33, 34, 37, 38, 39 is a key prognostic indicator in distal common bile duct carcinoma patients. Some also reported that prognosis worsens with increased number of positive nodes.31, 32, 33, 37
The prognostic significance of nodal disease underscores the importance of accurate gross sampling of lymph nodes, with examination of at least 12 nodes recommended for pancreatoduodenectomy specimens.48 We use an ‘orange-peeling’ technique20, 41 that has been proven to increase both node count and percentage of node-positive cases. This approach was used in 62% of our distal common bile duct carcinoma cases in this study and more than tripled the median number of nodes found in each case.
Most studies on distal common bile duct carcinoma, ours included, found positive margins to negatively impact prognosis,6, 7, 31, 33, 34 although a few did not.8, 39 Perineural invasion, found by some,8, 9, 31 but not all,33, 37 groups to be a negative prognostic indicator, did not have a prognostic impact in our study, although our rate of perineural invasion (91%) was higher than in these other studies, presumably due to the more careful scrutiny we used during re-review of the cases, along with the careful exclusion of non-pancreatobiliary-type cancers, which are less prone to show perineural invasion.
In summary, while less common than their intrahepatic counterparts, distal common bile duct carcinomas are a distinct entity that can require careful clinical, gross, and/or microscopic evaluation to properly identify. As they possess clinicopathologic characteristics significantly different than pancreatic ductal adenocarcinoma and ampullary carcinoma, which they can approximate both morphologically and anatomically, due diligence is warranted to provide accurate prognostic information to patients. While factors such as smaller tumor size and lower rate of margin positivity in distal common bile duct carcinoma compared with pancreatic ductal adenocarcinoma may be due to factors such as earlier onset of symptoms and increased ease of total resection due to tumor location, the relatively younger mean age of distal common bile duct carcinoma patients may be related to unknown genetic factors, including those that give rise to ductal anomalies such as low union.
References
Shaib Y, El-Serag HB . The epidemiology of cholangiocarcinoma. Semin Liver Dis 2004;24:115–125.
Shin HR, Oh JK, Masuyer E et al, Comparison of incidence of intrahepatic and extrahepatic cholangiocarcinoma—focus on East and South-Eastern Asia. Asian Pac J Cancer Prev 2010;11:1159–1166.
Nishimura M, Naka S, Hanazawa K et al, Cholangiocarcinoma in the distal bile duct: a probable etiologic association with choledocholithiasis. Dig Dis Sci 2005;50:2153–2158.
Bosman FT, Carneiro F, Hruban RH et al, (eds). WHO Classification of Tumours of the Digestive System, 4th edn. IARC Press: Lyon, France, 2010.
Blumgart LH (ed). Surgery of the Liver, Biliary Tract, and Pancreas, 4th edn. Saunders: Philadelphia, PA, 2006.
Nakeeb A, Pitt HA, Sohn TA et al, Cholangiocarcinoma. A spectrum of intrahepatic, perihilar, and distal tumors. Ann Surg 1996;224:463–473.
DeOliveira ML, Cunningham SC, Cameron JL et al, Cholangiocarcinoma: thirty-one-year experience with 564 patients at a single institution. Ann Surg 2007;245:755–762.
Bhuiya MR, Nimura Y, Kamiya J et al, Clinicopathologic factors influencing survival of patients with bile duct carcinoma: multivariate statistical analysis. World J Surg 1993;17:653–657.
He P, Shi JS, Chen WK et al, Multivariate statistical analysis of clinicopathologic factors influencing survival of patients with bile duct carcinoma. World J Gastroenterol 2002;8:943–946.
He J, Ahuja N, Makary MA et al, 2564 resected periampullary adenocarcinomas at a single institution: trends over three decades. HPB (Oxford) 2014;16:83–90.
Riall TS, Cameron JL, Lillemoe KD et al, Resected periampullary adenocarcinoma: 5-year survivors and their 6- to 10-year follow-up. Surgery 2006;140:764–772.
Schmidt CM, Powell ES, Yiannoutsos CT et al, Pancreaticoduodenectomy: a 20-year experience in 516 patients. Arch Surg 2004;139:718–725.
Adsay V, Ohike N, Tajiri T et al, Ampullary region carcinomas: definition and site specific classification with delineation of four clinicopathologically and prognostically distinct subsets in an analysis of 249 cases. Am J Surg Pathol 2012;36:1592–1608.
Zen Y, Fujii T, Itatsu K et al, Biliary papillary tumors share pathological features with intraductal papillary mucinous neoplasm of the pancreas. Hepatology 2006;44:1333–1343.
Rocha FG, Lee H, Katabi N et al, Intraductal papillary neoplasm of the bile duct: a biliary equivalent to intraductal papillary mucinous neoplasm of the pancreas? Hepatology 2012;56:1352–1360.
Barton JG, Barrett DA, Maricevich MA et al, Intraductal papillary mucinous neoplasm of the biliary tract: a real disease? HPB (Oxford) 2009;11:684–691.
Adsay NV, Pierson C, Sarkar F et al, Colloid (mucinous noncystic) carcinoma of the pancreas. Am J Surg Pathol 2001;25:26–42.
Adsay NV, Merati K, Andea A et al, The dichotomy in the preinvasive neoplasia to invasive carcinoma sequence in the pancreas: differential expression of MUC1 and MUC2 supports the existence of two separate pathways of carcinogenesis. Mod Pathol 2002;15:1087–1095.
Edge SB, Byrd DR, Carducci MA et al, (eds). AJCC Cancer Staging Manual, 7th edn. Springer: New York, NY, 2009.
Adsay NV, Basturk O, Altinel D et al, The number of lymph nodes identified in a simple pancreatoduodenectomy specimen: comparison of conventional vs orange-peeling approach in pathologic assessment. Mod Pathol 2009;22:107–112.
Adsay NV, Bagci P, Tajiri T et al, Pathologic staging of pancreatic, ampullary, biliary, and gallbladder cancers: pitfalls and practical limitations of the current AJCC/UICC TNM staging system and opportunities for improvement. Semin Diagn Pathol 2012;29:127–141.
Choi H, Saka B, Balci S et al, Proposal for a revised N-stage for pancreatic ductal adenocarcinoma as N1 (<3) and N2 (≥3) with strong prognostic correlation. Mod Pathol 2014;448A.
Saka B, Balci S, Basturk O et al, Pancreatic ductal adenocarcinoma is spread to the peripancreatic soft tissue in the majority of resected cases, rendering the AJCC T-stage protocol (7th edition) inapplicable and insignificant: a size-based staging system (pT1: ≤2, pT2: >2–≤4, pT3: >4 cm) is more valid and clinically relevant. Ann Surg Oncol 2016;23:2010–2018.
Saka B, Oliva I, Bandyopadhyay S et al, Will the pT1 and pT2 pancreas cancer please stand up? 'Peripancreatic soft tissue’ is involved in most pancreatic ductal adenocarcinomas (PDAC), negating its value as a staging parameter and necessitating a new staging scheme. Mod Pathol 2014;27:454A.
Hong SM, Cho H, Moskaluk CA et al, Measurement of the invasion depth of extrahepatic bile duct carcinoma: an alternative method overcoming the current T classification problems of the AJCC staging system. Am J Surg Pathol 2007;31:199–206.
Hong SM, Pawlik TM, Cho H et al, Depth of tumor invasion better predicts prognosis than the current American Joint Committee on Cancer T classification for distal bile duct carcinoma. Surgery 2009;146:250–257.
Dursun N, Feng J, Basturk O et al, Vacuolated cell pattern of pancreatobiliary adenocarcinoma: a clinicopathological analysis of 24 cases of a poorly recognized distinctive morphologic variant important in the differential diagnosis. Virchows Arch 2010;457:643–649.
Zen Y, Adsay NV, Bardadin K et al, Biliary intraepithelial neoplasia: an international interobserver agreement study and proposal for diagnostic criteria. Mod Pathol 2007;20:701–709.
Andea A, Sarkar F, Adsay VN . Clinicopathological correlates of pancreatic intraepithelial neoplasia: a comparative analysis of 82 cases with and 152 cases without pancreatic ductal adenocarcinoma. Mod Pathol 2003;16:996–1006.
Conlon KC, Klimstra DS, Brennan MF . Long-term survival after curative resection for pancreatic ductal adenocarcinoma. Clinicopathologic analysis of 5-year survivors. Ann Surg 1996;223:273–279.
Murakami Y, Uemura K, Hayashidani Y et al, Pancreatoduodenectomy for distal cholangiocarcinoma: prognostic impact of lymph node metastasis. World J Surg 2007;31:337–342.
Sasaki R, Takahashi M, Funato O et al, Prognostic significance of lymph node involvement in middle and distal bile duct cancer. Surgery 2001;129:677–683.
Yoshida T, Matsumoto T, Sasaki A et al, Prognostic factors after pancreatoduodenectomy with extended lymphadenectomy for distal bile duct cancer. Arch Surg 2002;137:69–73.
Kayahara M, Nagakawa T, Ohta T et al, Role of nodal involvement and the periductal soft-tissue margin in middle and distal bile duct cancer. Ann Surg 1999;229:76–83.
Shimizu Y, Kimura F, Shimizu H et al, The morbidity, mortality, and prognostic factors for ampullary carcinoma and distal cholangiocarcinoma. Hepatogastroenterology 2008;55:699–703.
Ito Y, Kenmochi T, Egawa T et al, Diagnosis of distal cholangiocarcinoma after the removal of choledocholithiasis. Gastroenterol Res Pract 2012;396869.
Hong SM, Cho H, Lee OJ et al, The number of metastatic lymph nodes in extrahepatic bile duct carcinoma as a prognostic factor. Am J Surg Pathol 2005;29:1177–1183.
Deshpande V, Konstantinidis IT, Castillo CF et al, Intra-pancreatic distal bile duct carcinoma is morphologically, genetically, and clinically distinct from pancreatic ductal adenocarcinoma. J Gastrointest Surg 2016;20:953–959.
Fong Y, Blumgart LH, Lin E et al, Outcome of treatment for distal bile duct cancer. Br J Surg 1996;83:1712–1715.
Veillette G, Castillo CF . Distal biliary malignancy. Surg Clin N Am 2008;88:1429–1447, xi.
Adsay NV, Basturk O, Saka B et al, Whipple made simple for surgical pathologists: orientation, dissection, and sampling of pancreaticoduodenectomy specimens for a more practical and accurate evaluation of pancreatic, distal common bile duct, and ampullary tumors. Am J Surg Pathol 2014;38:480–493.
Bragazzi MC, Cardinale V, Carpino G et al, Cholangiocarcinoma: epidemiology and risk factors. Transl Gastrointest Cancer 2012;1:21–32.
Kosar I, Ataseven H, Yönem O et al, A new variant of bile duct duplication with coexistence of distal cholangiocarcinoma. Nat Rev Gastroenterol Hepatol 2010;7:527–530.
DiMagno EP . Pancreatic cancer: clinical presentation, pitfalls and early clues. Ann Oncol 1999;10:140–142.
Mangiavillano B, Mariani A A, Petrone MC . An intrapancreatic cholangiocarcinoma detected with optical coherence tomography during endoscopic retrograde cholangiopancreatography. Clin Gastroenterol Hepatol 2008;6:A30.
Adsay NV, Bandyopadhyay S, Basturk O et al, Chronic pancreatitis or pancreatic ductal adenocarcinoma? Semin Diagn Pathol 2004;21:268–276.
Kurosaki I, Tsukada K, Hatakeyama K et al, The mode of lymphatic spread in carcinoma of the bile duct. Am J Surg 1996;172:239–243.
Bilimoria KY, Bentrem DJ, Lillemoe KD et al, Pancreatic cancer quality indicator development expert panel, American College of Surgeons. Assessment of pancreatic cancer care in the United States based on formally developed quality indicators. J Natl Cancer Inst 2009;101:848–859.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Gonzalez, R., Bagci, P., Basturk, O. et al. Intrapancreatic distal common bile duct carcinoma: Analysis, staging considerations, and comparison with pancreatic ductal and ampullary adenocarcinomas. Mod Pathol 29, 1358–1369 (2016). https://doi.org/10.1038/modpathol.2016.125
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/modpathol.2016.125
This article is cited by
-
Intra-pancreatic distal cholangiocarcinoma and pancreatic ductal adenocarcinoma: a common short and long-term prognosis?
Updates in Surgery (2021)
-
Bile duct angulation and tumor vascularity are useful radiographic features for differentiating pancreatic head cancer and intrapancreatic bile duct cancer
Surgery Today (2018)
-
Cytologic predictors of malignancy in bile duct brushings: a multi-reviewer analysis of 60 cases
Modern Pathology (2017)
