
Abstract
Lymphomas are a group of hematological malignancies derived from lymphocytes. Lymphomas are clinically and biologically heterogeneous and have overlapping diagnostic features. With the advance of new technologies and the application of efficient and feasible detection platforms, an unprecedented number of novel biomarkers have been discovered or are under investigation at the genetic, epigenetic, and protein level as well as the tumor microenvironment. These biomarkers have enabled new clinical and pathological insights into the mechanisms underlying lymphomagenesis and also have facilitated improvements in the diagnostic workup, sub-classification, outcome stratification, and personalized therapy for lymphoma patients. However, integrating these biomarkers into clinical practice effectively and precisely in daily practice is challenging. More in-depth studies are required to further validate these novel biomarkers and to assess other parameters that can affect the reproducibility of these biomarkers such as the selection of detection methods, biological reagents, interpretation of data, and cost efficiency. Despite these challenges, there are many reasons to be optimistic that novel biomarkers will facilitate better algorithms and strategies as we enter a new era of precision medicine to better refine diagnosis, prognostication, and rational treatment design for patients with lymphomas.
Similar content being viewed by others


Main
Lymphomas are a group of hematological malignancies that are derived from lymphocytes and occur predominantly in lymph nodes or other lymphoid structures. More than 50 different types of lymphoma were described in the 2008 World Health Organization Classification of Tumors of the Hematopoietic and Lymphoid Tissues.1 Lymphomas are heterogeneous at the clinical, morphological, and molecular level, and have overlapping features. Mechanistic studies have shown that lymphomas are driven or affected by abnormal genetic alterations, disordered epigenetic regulation, aberrant pathway activation, and complex tumor–microenvironment interactions.2, 3, 4 Hence, the diagnosis and classification of different lymphomas and related entities can be challenging. In addition, the molecular heterogeneity underlying lymphoma aggressiveness and progression leads to patients who are treated similarly having variable outcomes.5, 6, 7 Although biomarkers, especially protein markers detected mainly by immunohistochemistry and flow cytometry, have been used widely and have contributed greatly to diagnosis, classification, and prognostication of lymphomas, novel clinically applicable, reliable, and reproducible biomarkers for lymphoma diagnosis and prognosis are still needed for better supervision of clinical trials.
In this review, we summarize biomarkers that are related to alterations in lymphomas at the genetic, epigenetic, and protein level as well as the tumor microenvironment. We mainly concentrate on the diagnostic and prognostic value of these biomarkers in the most common types of lymphoma.
Biomarkers of genetic alterations
Genomic aberrations and relevant dysregulated oncogenic regulatory pathways account for many malignant phenotypes in lymphomagenesis.4, 8 With the wide application of advanced technologies, the identification of genetic alterations and related biomarkers has become available.4 Microarray-based technologies like gene expression profiling and massively parallel sequencing technologies like next-generation sequencing have enabled the discovery of novel biomarkers and the exploration of underlying molecular mechanisms of lymphomagenesis;2, 9 these findings also support better diagnosis and stratification of patients who may benefit from potential therapeutic strategies based on targeting specific alterations. Figures 1 and 2 summarize recurrent genomic and molecular biomarkers involved in B-cell, T-cell, and natural killer (NK) cell lymphomas. The prognostic effects of genetic abnormalities of MYC, BCL2, BCL6, and TP53 in diffuse large B-cell lymphoma are also presented using a large cohort data set in Figure 3.10, 11, 12, 13

Schematic representation of B-cell development and summary of molecular and immunophenotypic biomarkers in B-cell non-Hodgkin lymphomas and Hodgkin lymphomas. The GC is an important structure during B-cell differentiation (black arrows direct the B-cell development). Most types of B-cell lymphoma are proposed to be derived from GC or post-GC B cells (purple arrows indicate the proposed cellular origin of B-cell lymphomas). FL, BL, and GCB-DLBCL are of GC origin, whereas ABC-DLBCL, PMBL, and cHL are inferred to be post-GC origin. MCL is thought to be derived from the mantle zone. Certain molecular features are relatively specific for given type of lymphoma and have diagnostic or prognostic potential. Recurrent gain of function (red) and loss of function (blue) molecular biomarkers of common types of B-cell lymphoma and HLs are summarized. Immunohistochemical biomarkers (green) that are of diagnostic value in B-cell lymphomas are also shown. ABC-DLBCL, activated B-cell-DLBCL; BL, Burkitt lymphoma; cHL, classical Hodgkin lymphoma; FDC, follicular dendritic cell; FL, follicular lymphoma; GCB-DLBCL, GC B-cell-like diffuse large B-cell lymphoma; MCL, mantle cell lymphoma; PMBCL, primary mediastinal B-cell lymphoma; TFH, T follicular helper cell.

Schematic representation of T- and NK-cell development and summary of the molecular and immunophenotypic biomarkers in the most common types of peripheral T- and NK-cell lymphoma. T-cells originate from HSC and CLP in the bone marrow and then migrate to the thymus to undergo positive or negative selection. Eventually, single-positive T-cells enter the periphery (black solid arrows direct T-cell development; black broken arrows direct some inclusive NK/NKT-cell development). Most types of T-cell lymphoma are CD4-positive (purple arrows indicate the proposed origin of T-cell lymphomas). Certain molecular features are relatively specific for a given type or subtype of T-cell lymphoma and have diagnostic or prognostic potential. Recurrent gain of function (red) and loss of function (blue) molecular biomarkers of the most common types of peripheral T- and NK-cell lymphoma are summarized. Immunohistochemical biomarkers (green) that have diagnostic value in the most common types of peripheral T- and NK-cell lymphoma are also shown. ALCL, anaplastic large cell lymphoma; AITL, angioimmunoblastic T-cell lymphoma; ALK, anaplastic lymphoma kinase; ATLL, adult T-cell leukemia/lymphoma; CLP, common lymphoid progenitors; DN, double negative; DP, double positive; ENKTCL, extranodal NK/T-cell lymphoma; HSC, hematopoietic stem cell; NK, natural killer; NKT, natural killer T-cell; PTCL-NOS, peripheral T-cell lymphoma, not otherwise specified.

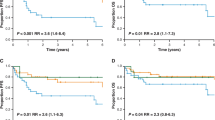
Prognostic effects of genetic abnormalities and overexpression of MYC, BCL2, BCL6, and TP53 in diffuse large B-cell lymphoma. (a–b) MYC or BCL2 translocations (MYC-R and BCL2-R) correlated with significant poorer OS in DLBCL. (c) BCL6 translocations (BCL6-R) did not significantly correlate with poorer OS in DLBCL. (d) Patients with TP53 mutations (MUT-TP53) had significantly poorer OS in DLBCL than patients wild-type TP53 (WT-TP53). (e) MYC translocations correlated with significant poorer PFS in DLBCL. (f–g) BCL2 or BCL6 translocations did not significantly correlate with poorer PFS in DLBCL. (h) Patients with TP53 mutations had significantly poorer PFS in DLBCL than patients wild-type TP53. (i–j) Myc or Bcl-2 overexpression (≥70%) correlated with significant poorer OS in DLBCL. (k) High level of Bcl-6 protein (>50%) did not correlate with poorer OS in DLBCL. (l) p53 overexpression (≥ 20%) correlated with significant poorer OS in DLBCL. (m–n) Myc or Bcl-2 overexpression correlated with significant poorer PFS in DLBCL. (o) High level of Bcl-6 protein correlated with significantly better PFS in DLBCL. (l) p53 overexpression correlated with significant poorer PFS in DLBCL. The clinical and pathological data in this figure have been organized from International DLBCL Consortium Program. Results have been previously reported and now are organized for presentation in different formats.10, 11, 12, 13 DLBCL, diffuse large B-cell lymphoma; OS, overall survival; PFS, progression-free survival.
B-Cell Lymphoma 6 (BCL6)
BCL6 encodes a transcriptional factor that has a key role in germinal center B-cell differentiation and in the pathogenesis of germinal center-derived lymphomas. Translocation and mutation are the most common means by which BCL6 activity is dysregulated.14, 15 Both rearrangement and somatic mutation of BCL6 can be present simultaneously in diffuse large B-cell lymphoma, but somatic mutations occur independently of BCL6 rearrangement. Studies in vitro and in animal models have shown that aberrant Bcl-6 expression results mainly from BCL6 translocation.16, 17 High expression of BCL6 mRNA and protein have been shown to be associated with better prognosis for patients with diffuse large B-cell lymphoma, concordant with immunohistochemical stain.18, 19 Some reported results are inconsistent in the literature, possibly attributable to heterogeneity within BCL6 mRNA expression and/or post-translational regulation.16
Tumor Protein 53 (TP53)
Dysfunction of the TP53 tumor suppressor gene is common in many hematological malignancies. Despite a low frequency of mutation in hematological malignancies, TP53 mutation status is an independent prognostic biomarker in patients with diffuse large B-cell lymphoma, follicular lymphoma, and mantle cell lymphoma.20, 21 In diffuse large B-cell lymphoma patients, rather than TP53 deletion and loss of heterozygosity, TP53 mutation has been shown to be associated with a poorer prognosis in patients with either germinal center B-cell-like diffuse large B-cell lymphoma or activated B-cell-like diffuse large B-cell lymphoma, especially if the mutations occur in the Loop-sheet-helix, L3, and L2 motifs of the DNA-binding domain.20 These results are true in diffuse large B-cell lymphoma patients treated with either the cyclophosphamide, doxorubicin, vincristine, prednisolone (CHOP), or rituximab plus CHOP (R-CHOP) chemotherapy regimens.10 Thus, it is necessary to account for TP53 mutation status in the design of future therapeutic strategies for diffuse large B-cell lymphoma patients.
V-Myc Avian Myelocytomatosis Viral Oncogene Homolog (MYC)
MYC is one of the most important oncogenes in cancer. As a pleiotropic transcription factor, MYC is involved in almost every process of cell biology and oncology by interacting with thousands of target genes.22, 23 In the prototypical example of a MYC translocation in cancer, Burkitt lymphoma, MYC normally located on chromosome 8q24 is juxtaposed with the IGH on the derivative chromosome 14 or with the 'IG light chains' on the derivative chromosome 8. The t(8;14)(q24;q32), t(2;8)(p12;q24), or t(8;22)(q24;q11) lead to Myc overexpression.22, 24 MYC translocations with either IG or non-IG partners also occur in diffuse large B-cell lymphoma and other aggressive B-cell lymphomas,24, 25 and usually are associated with a poorer prognosis, particularly MYC-IG translocations.26, 27
B-Cell Lymphoma 2 (BCL2)
t(14;18)(q32;q21), involving IGH and BCL2 at chromosome 18q21, has been proven to be a molecular hallmark of follicular lymphoma28 and also can be detected in germinal center B-cell-like diffuse large B-cell lymphoma.29 In contrast, BCL2 is rarely translocated but frequently amplified in activated B-cell-like diffuse large B-cell lymphoma.30, 31 Fluorescence in situ hybridization analysis has confirmed a strong correlation between BCL2 rearrangement and germinal center B-cell-like subtype.32 The prognostic impact of BCL2 alterations in diffuse large B-cell lymphoma remains controversial and may depend on subtype, Bcl-2 expression, BCL2 gene polymorphism, and the treatment regimen.31, 33, 34 A minority of diffuse large B-cell lymphoma cases associated with both MYC translocation and t(14;18)/IGH/BCL2 and/or BCL6 translocation are commonly designated as double-hit or triple-hit lymphoma and affected patients usually have an aggressive clinical course and poor prognosis.26, 27, 35
Myeloid Differentiation Primary Response 88 (MYD88)
MYD88, an adaptor protein, has a role in facilitating Toll-like and interleukin 1 receptor signaling.36 Somatic mutation of MYD88L265P is the most frequent mutation found in lymphoplasmacytic lymphoma/Waldenstrom macroglobulinemia and activated B-cell-like diffuse large B-cell lymphoma.36, 37, 38 MYD88 mutations also occur in small (<5%) subsets of marginal zone lymphoma, mantle lymphoma, and chronic lymphocytic leukemia/small lymphocytic lymphoma. MYD88 mutation has not been observed to have prognostic impact in patients with diffuse large B-cell lymphoma, but MYD88 protein expression, regardless of the MYD88 genetic status, has been shown to be significantly associated with recurrence and shorter disease-free survival.37, 39
Spi-B Transcription Factor (SPIB)
SPIB, which encodes an ETS family transcription factor on chromosome 19, is expressed at substantially elevated levels and can be detected in 26% of activated B-cell-like diffuse large B-cell lymphoma, but only in 3% of germinal center B-cell-like diffuse large B-cell lymphoma and primary mediastinal B-cell lymphoma. Knockdown of SPIB in cell lines also indicates that SPIB is an oncogene dysregulated by chromosomal aberrations in activated B-cell-like diffuse large B-cell lymphoma.30
Tumor Necrosis Factor α-Induced Protein 3 (TNFAIP3)
TNFAIP3, which encodes the NF-κB inhibitor A20, is commonly mutated, deleted, or silenced epigenetically in activated B-cell-like diffuse large B-cell lymphoma, primary mediastinal B-cell lymphoma, mantle cell lymphoma, and classical Hodgkin lymphoma.40, 41, 42 Inactivation of TNFAIP3 has a role in dysregulation of the NF-κB pathway.
Major Histocompatibility Complex Class II Transactivator (CIITA)
CIITA, located at chromosome 16p13.13, is a non-DNA-binding coactivator of the major histocompatibility complex (MHC) class II promoter. CIITA is altered by chromosomal translocation in 38% of primary mediastinal B-cell lymphoma cases, which is associated with reduced MHC class II expression. Translocations involving CIITA are uncommon in de novo diffuse large B-cell lymphoma, and seen in <5% of cases.43, 44 Deletion or mutation of CIITA is also uncommon in diffuse large B-cell lymphoma.45, 46 Therefore, CIITA has the potential to act as a biomarker to distinguish primary mediastinal B-cell lymphoma from diffuse large B-cell lymphoma. However, CIITA is also translocated in 15–20% of cases of classical Hodgkin lymphoma.43
Other Genetic Biomarkers or Simplified Gene Expression Models in B-Cell Lymphomas
Several investigators have attempted to simplify analysis of gene expression profiling using smaller gene expression models. In particular, attempts to quantitate gene expression for activated B-cell-like/germinal center B-cell-like molecular sub-classification using formalin-fixed and paraffin-embedded tissue have become clinically practicable.47, 48, 49
Lossos et al.50 identified a six-gene model (LMO2, BCL6, FN1, CCND2, SCYA3, and BCL2) that could predict survival in CHOP-treated diffuse large B-cell lymphoma patients. Another study combined LIM domain only two (LMO2) expressed by tumor cells and tumor necrosis factor receptor superfamily member 9 (TNFRS9) expressed by microenvironmental cells to predict overall survival in patients with diffuse large B-cell lymphoma.51
Love et al.52 identified several recurrently mutated genes in Burkitt lymphoma including ID3, GNA13, RET, PIK3R1, ARID1A, and SMARCA4 as well as MYC. They found that ID3 is mutated in Burkitt lymphoma, but not in most cases of diffuse large B-cell lymphoma, implicating ID3 as a new tumor suppressor gene that has lost function via genetic alteration(s) and could be a new potential therapeutic target in Burkitt lymphoma. In addition to ID3 and MYC, TPST2 and RET mutations were also found predominantly in Burkitt lymphoma, whereas PIM1, CECR1 and MYD88 mutations occurred predominantly in diffuse large B-cell lymphoma. MLL3, TP53, and LAMA3 showed overlapping patterns of mutation in Burkitt lymphoma and diffuse large B-cell lymphoma.
The chromosomal translocation t(11:14)(q13;q32), involving CCND1 at 11q13, leads to overexpression of cyclin D1 and is the molecular hallmark of mantle cell lymphoma.53 Hartmann et al.54 established a gene expression-based predictor of survival in mantle cell lymphoma patients using a quantitative PCR with reverse transcription-based assay on formalin-fixed, paraffin-embedded tissue specimens. This model identified five genes including RAN, MYC, TNFRSF10B, POLE2, and SLC29A2. Elevated expression of TNFRSF10B was associated with a favorable outcome; in contrast, increased expression of RAN, MYC, POLE2, and SLC29A2 correlated with a poorer prognosis.
Pastore et al.55 integrated the mutation status of seven-genes (EZH2, ARID1A, MEF2B, EP300, FOXO1, CREBBP, and CARD11) with the follicular lymphoma international prognostic index (FLIPI) and established a clinicogenetic-risk stratification model for follicular lymphoma patients (known as the m7-FLIPI). This model exhibits a reasonable ability to recognize a high-risk group (28%) of patients with follicular lymphoma with 5-year failure-free survival, but needs to be further validated in an independent study.
The diagnosis of primary mediastinal B-cell lymphoma can be challenging because there is morphological and immunophenotypic overlap with classical Hodgkin lymphoma.56, 57 Specific characteristics of primary mediastinal B-cell lymphoma include STAT6 constitutive activation and JAK2 amplification.58, 59 In contrast, NF-κB1A mutation is rather specific for classical Hodgkin lymphoma, suggesting that NF-κB activation in classical Hodgkin lymphoma and primary mediastinal B-cell lymphoma may result from different gene mutations and other mechanisms.59, 60
Other Genetic Biomarkers or Gene Expression Models for Differential Diagnosis in Peripheral T-Cell Lymphoma
Approximately 30–50% cases of peripheral T-cell lymphoma are categorized as peripheral T-cell lymphoma, not otherwise specified, because of a lack of specific morphological features and key biomarkers. However, studies using gene expression profiling have shown that a subset of cases of peripheral T-cell lymphoma, not otherwise specified has profiles more consistent with angioimmunoblastic T-cell lymphoma, adult T-cell leukemia/lymphoma, anaplastic large T-cell lymphoma or extra-nodal NK/T-cell lymphoma.6, 61 Moreover, cases of peripheral T-cell lymphoma, not otherwise specified without a distinctive profile can be classified into two subsets based on distinct oncogenic pathways and associated with different outcomes. One subgroup, characterized by high expression of GATA3 and its known target genes (CCR4, IL18RA, CXCR7, and IK) is associated with poorer overall survival. Another subgroup, characterized by high expression of cytotoxic gene signature such as TBX21, EOMES and their target genes (CXCR3, IL2RB, CCL3, and IFNγ) is associated with a more favorable clinical outcome.6
Chromosomal translocations also occur in some types of T-cell lymphoma. In anaplastic lymphoma kinase (ALK)-positive anaplastic large T-cell lymphoma, a characteristic chromosomal translocation, t(2;5)(p23;q35) involving NPM/ALK, or other ALK translocations occur. As a consequence, ALK is aberrantly expressed by the lymphoma cells.62 In ALK− anaplastic large T-cell lymphoma, ~20% of cases carry t(6;7)(p25.3;q32.3) involving DUSSP22 at 6p25.3 which was discovered by massively parallel genomic (next-generation) sequencing.63 DUSP22 is located within 40 kb of MUM1/IRF4 and is a dual-specificity phosphatase that physiologically has a role in inhibiting T-cell receptor signaling. Translocations involving DUSP22 result in reduced DUSP22 expression; these data suggest that translocation disrupts the tumor suppressor gene functions of DUSP22. A second subset of ~10% of cases of ALK- anaplastic large T-cell lymphoma carries rearrangements of TP63, a homolog of TP53, located at chromosome on 3q28. Fluorescence in situ hybridization may be utilized to identify these chromosomal translocations. The remaining cases of ALK− anaplastic large T-cell lymphoma have neither DUSP22 nor TP63 translocations.64
Despite the overlap of morphology and immunophenotype, ALK+ and ALK− anaplastic large cell lymphoma are associated with different patient outcomes. In general, ALK+ anaplastic large cell lymphoma patients have a better outcome than patients with ALK− anaplastic large cell lymphoma as a single entity, but patients with DUSSP22/IRF4 locus abnormalities also have a relatively good outcome.64 Therefore, these translocations might be used as biomarkers not only in diagnosis of ALK+ anaplastic large cell lymphoma and ALK− anaplastic large cell lymphoma, but also as molecular targets for therapeutic inhibitors. ALK-targeting drugs used to treat non-small cell lung cancer with EML4/ALK fusion may also benefit patients with ALK+ anaplastic large cell lymphoma.65, 66
Assessment of T-cell receptor rearrangement is necessary for establishing the diagnosis of many cases of T-cell lymphoma, most often accomplished by using PCR assays to demonstrate T-cell monoclonality. NK cell lymphoma, however, is an exception because NK cells do not rearrange their T-cell receptor genes. Killer cell immunoglobulin-like receptor (KIR), as one of NK cell receptors, can be used as a surrogate biomarker of clonal cellular expansion to distinguish reactive NK cell proliferations from neoplastic disease.67, 68 Restricted KIR expression can be immunohistochemically detected in extranodal NK/T-cell lymphoma.69
The t(5,9)(q33;q22) involving ITK and SYK has been found to be common in the follicular variant of peripheral T-cell lymphoma, not otherwise specified which has characteristic expression of T follicular helper cell markers similar to angioimmunoblastic T-cell lymphoma.70, 71 This translocation may serve as a diagnostic biomarker for the follicular variant of peripheral T-cell lymphoma, not otherwise specified.
Overall, genetic alterations that are relatively specific for a given type of lymphoma may be a defining feature or have prognostic implications, and are of great value in the evaluation of lymphomas.
Biomarkers related to epigenetic alterations
Epigenetic alterations are usually defined as heritable changes independent of alterations in DNA sequence.72 In numerous cellular processes of lymphomas, epigenetic aberrations have been shown to alter genes involved in signal transduction, DNA repair, cell cycle regulation, differentiation, invasion, and apoptosis.73, 74 With components of the epigenome being the focus of extensive studies, and epigenetic alterations involved in lymphomagenesis being understood in various types of lymphomas, altered patterns of DNA methylation, histone modification, and noncoding RNA expression are promising potential biomarkers for lymphoma diagnosis, assessment of prognosis, and prediction of response to therapy (Table 1).
P16/INK4
One of the most frequent molecular alterations of P16/INK4A is homozygous deletion.75, 76 However, methylation also has a major role in P16/INK4A inactivation in lymphomas and has been associated with a poorer prognosis in some studies.77, 78, 79 To date, the prognostic importance of P16/INK4A promoter methylation in lymphomas remains inconsistent and needs to be validated.78, 79
DNA Repair Enzyme O(6)-Methylguanine DNA Methyltransferase (MGMT)
MGMT, although rarely deleted or mutated, frequently loses its function as a result of epigenetic alteration. MGMT promoter hypermethylation has been found to correlate with a favorable prognosis in diffuse large B-cell lymphoma patients treated with multidrug regimens including cyclophosphamide.80
Kruppel-Like Factor 4 (KLF4)
KLF4 acts as a tumor suppressor gene in T- and B-cell lymphomas and is aberrantly hypermethylated in many types of lymphoma including follicular lymphoma, diffuse large B-cell lymphoma, Burkitt lymphoma and Hodgkin lymphoma.79, 81 These findings suggest a subtype-independent mechanism of lymphomagenesis. Epigenetic silencing of KLF4 may be of potential benefit to patients with B-cell lymphomas and particularly classical Hodgkin lymphoma.81
Myeloid/Lymphoid or Mixed-Lineage Leukemia 2 (MLL2)
MLL2 (also known as KMT2D) encodes human H3K4-specific histone methyltransferase and is inactivated by mutations in about 90% of follicular lymphoma and 32% of diffuse large B-cell lymphoma; there is no difference between germinal center B-cell-like diffuse large B-cell lymphoma and activated B-cell-like diffuse large B-cell lymphoma.79, 82
Myocyte Enhancer Factor 2 (MEF2)
MEF2, a calcium-regulating gene, encodes transcription factors and recruits histone-modifying enzymes.79, 82 MEF2B mutations have been linked to lymphoma. These mutations are somatic and are detected mostly in germinal center B-cell-like diffuse large B-cell lymphoma and follicular lymphoma, suggesting that MEF2B mutations have a role in enhancing the malignant transformation of germinal center B cells to lymphoma.82 In addition, one study showed somatic mutations of MEF2B in a subset of diffuse large B-cell lymphoma with consequential dysregulation of BCL6 expression, suggesting that inhibition of MEF2 could be an alternative to inhibit BCL6 activity for patients with diffuse large B-cell lymphoma and MEF2B mutation.79, 83
Enhancer of Zeste 2 Polycomb Repressive Complex 2 (EZH2)
EZH2 is one of the most commonly mutated epigenetic modifiers and is mutated in 27% of follicular lymphoma84 and 6-14% of diffuse large B-cell lymphoma.85, 86 EZH2Y641 mutations can enhance H3K27 trimethylation activity of the polycomb repressive complex 2 in diffuse large B-cell lymphoma and follicular lymphoma, mainly occurring in germinal center B-cell-like diffuse large B-cell lymphomas. EZH2 mutations have not been observed to have prognostic impact, but protein expression may be a better prognostic indicator of overall survival. The combination of an EZH2 inhibitor and demethylating agents might be a useful therapeutic option for patients with an EZH2 hypermethylation phenotype.87, 88
Other Epigenetic Gene Signatures
Other aberrant epigenetic gene signatures have been identified in several studies. For example, five hypermethylated genes (SOX9, HOXA9, AHR, NR2F2, and ROBO1) were found to correlate with higher proliferation, increased chromosomal abnormalities, and poorer survival in patients with mantle cell lymphoma.89
Using quantitative real-time methylation assays, Bethge et al90 analyzed the methylation status of a colorectal cancer biomarker panel (CNRIP1, FBN1, INA, MAL, SNCA, and SPG20) and showed that methylation of SNCA and SPG20 separate lymphoma from healthy control samples with high sensitivity (98%) and specificity (100%), suggesting that SNCA and SPG20 methylation status could be suitable for early detection and monitoring of patients with non-Hodgkin lymphomas. Meanwhile, promoter methylation of CNRIP1 was found to be associated with poorer overall survival in patients with diffuse large B-cell lymphoma and potentially could be used as a prognostic factor. Another concise methylation signature set that includes TNF alpha pathway biomarkers and downstream biomarkers was shown to be helpful in distinguishing germinal center B-cell-like diffuse large B-cell lymphoma from activated B-cell-like diffuse large B-cell lymphoma.91 Hypermethylation of SMAD family member 1 (SMAD1) has been reported to predict chemotherapy resistance in patients with diffuse large B-cell lymphoma,92, 93 and functional assays have confirmed that chemotherapy responsiveness can be induced through SMAD1 expression in chemotherapy-resistant diffuse large B-cell lymphoma cells.92
Using a combination of whole-exome sequencing, RNA sequencing analysis and targeted deep sequencing, Palomero et al94 identified frequently mutated genes involved in epigenetic alterations in peripheral T-cell lymphoma, including ten-eleven translocation 2 (TET2), DNA methyltransferase 3A (DNMT3A), isocitrate dehydrogenase 2 (IDH2), and RHOA. RHOA is mutated in up to 67% of angioimmunoblastic T-cell lymphoma and 18% of peripheral T-cell lymphoma, not otherwise specified. TET2 mutations occur in both angioimmunoblastic T-cell lymphoma and peripheral T-cell lymphoma, not otherwise specified with similar frequency and are associated with advanced-stage disease, thrombocytopenia, high International Prognostic Index scores, and a shorter progression-free survival. IDHR172 mutation occurs mainly in angioimmunoblastic T-cell lymphoma and has potential as a specific biomarker of this disease.94, 95, 96 IDH2 mutations in angioimmunoblastic T-cell lymphoma have not been associated with overall survival.97
Biomarkers related to epigenetic regulation have great potential for use in the diagnosis of lymphomas and for prognostication. However, the relationship between mutations and epigenetic status of these genes, and the value of these alterations for diagnosis and prognosis in lymphomas needs to be further explored.
MicroRNA and lncRNA as Biomarkers for Diagnosis and Prognosis in Lymphomas
MicroRNAs, a class of small noncoding RNA, regulate numerous biological processes at the post-transcriptional level by targeting a broad set of messenger RNAs and affecting a multitude of cellular transcripts and pathways.98, 99 Long noncoding RNAs (lncRNAs) have specific tissue expression patterns and nuclear location, and exhibit an important role in regulating gene expression at different levels and in malignant transformation, mainly involving regulation of epigenetic processes.100, 101, 102 Growing evidence supports a role for dysregulation of expression of microRNAs and lncRNAs in the development and progression of lymphomas and the rationale that microRNAs and lncRNAs may serve as promising biomarkers for diagnosis and prognosis in lymphoma patients (Table 2).5, 98, 101, 103
miR-155
miR-155 is one of the best recognized miRNA in lymphomas, particularly in diffuse large B-cell lymphoma. miR-155 acts as an onco-miR in the pathogenesis and aggressiveness of diffuse large B-cell lymphoma.104 Levels of miR-155 in activated B-cell-like diffuse large B-cell lymphoma were found to be significantly higher than that in germinal center B-cell-like diffuse large B-cell lymphoma, suggesting that miR-155 is diagnostically useful to distinguish activated B-cell-like diffuse large B-cell lymphomas from germinal center B-cell-derived tumors and may explain the poor prognosis of activated B-cell-like diffuse large B-cell lymphoma patients.105 In transgenic mice models, the critical role of constitutive expression of miR-155 in activated B-cell-like diffuse large B-cell lymphoma tumorigenesis has been shown.106 Furthermore, a correlation between miR-155 expression and resistance to R-CHOP therapy in diffuse large B-cell lymphoma patients has been observed.5
miR-17-92 Cluster
The miR-17-92 cluster, including six microRNAs (miR-17, miR-18a, miR-19a, miR-20a, miR-19b1, and miR-92-1), is encoded by locus 13q31.3 and is overexpressed as a consequence of 13q31.3 locus amplification107 in several types of lymphoma, including germinal center B-cell-like diffuse large B-cell lymphoma, follicular lymphoma, mantle cell lymphoma,4, 30, 108 anaplastic large cell lymphoma,109 and Burkitt lymphoma,110 but never in activated B-cell-like diffuse large B-cell lymphoma.4 Additionally, the miR-17-92 cluster is expressed more highly in ALK+ anaplastic large cell lymphoma compared with ALK- anaplastic large cell lymphoma,109 supporting a role for miR-17-92 in sustaining the oncogenic characteristics of STAT3 through the ALK-STAT3-microRNA-17-92 pathway in ALK+ anaplastic large cell lymphoma.111 Overexpression of the miR-17-92 cluster correlates with a poorer overall survival in patients with mantle cell lymphoma.108
miR-15a/16-1
Deregulation of miR-15a/16-1, resulting from deletion of chromosome 13q14, is implicated in the pathogenesis of chronic lymphocytic leukemia/small lymphocytic lymphoma, a disease that more typically presents with leukeumic disease rather than lymphomatous disease.112 Deletion of 13q14 and consequent low expression of miR-15a/16-1 have been associated with favorable prognosis for patients with chronic lymphocytic leukemia/small lymphocytic lymphoma, whereas other chromosomal abnormalities, such as 17p deletion, 12q trisomy, and 11q deletion, correlate with a poorer prognosis.113
Other MicroRNAs and MicroRNA-Based Classifiers
High expression of miR-18b and downregulation of the miR-29 family are independent predictors of poor outcome in patients with mantle cell lymphoma.114, 115 Notably, a combination of miR-127-3p with Ki67 can provide a novel prognostic model for mantle cell lymphoma. Similarly, the combination of miR-615-3p and the Mantle Cell Lymphoma International Prognostic Index has prognostic value.116
Using a Bayesian algorithm, Iqbal et al5 developed a 27-miRNA classifier that can distinguish Burkitt lymphoma from diffuse large B-cell lymphoma and an 8-miRNA classifier that separates diffuse large B-cell lymphoma subgroups. The activated B-cell-like diffuse large B-cell lymphoma signature includes miR-155 and miR-542-3p. miR-155 has been known for its association with activated B-cell-like diffuse large B-cell lymphoma as mentioned above; this is the first report of miR-542 in activated B-cell-like diffuse large B-cell lymphoma. Six miRNAs (miR-28-3p, miR-28-5p, miR-129-3p, miR-589, miR-331-5p, and miR-597) are upregulated in germinal center B-cell-like diffuse large B-cell lymphoma. This miRNA classification of diffuse large B-cell lymphoma subgroups has been shown to be 90% concordant with gene expression profiling-based classification and is reproducible in formalin-fixed and paraffin-embedded tissues.5
A set of miRNAs (miR-222, miR-181a, miR-129-5p, and miR-18a) has been shown prognostic value for diffuse large B-cell lymphoma patients,117 whereas another miRNA set was peculiar to hepatitis C virus-associated diffuse large B-cell lymphoma.118 In this hepatitis C virus-associated subgroup, miR-138-5p was associated with longer overall survival and miR-147a, miR-147b and miR-511-5p were associated with shorter overall survival. miR-222 expression has been shown to be consistently associated with an inferior overall survival in lymphoma patients.5
DNA methylation of the miRNA gene promoter has been implicated in lymphomagenesis. Asmar et al119 reported that a large number of miR-34s are downregulated by promoter hypermethylation in diffuse large B-cell lymphoma. Intriguingly, they identified a new TP53/MIR34A 'double hit' diffuse large B-cell lymphoma subgroup, which has concomitant MIR34A methylation and TP53 mutation; this subgroup had significantly poorer overall survival, irrespective of treatment after rituximab. Thus, MIR34A methylation combined with TP53 mutation can be used to identify an aggressive subgroup of diffuse large B-cell lymphoma which may benefit from epigenetic therapy.
Besides tumor biopsy specimens, microRNA can be assessed in serum, plasma and bone marrow smears.120, 121 A five-miRNA serum signature has been shown to be predictive of prognosis for diffuse large B-cell lymphoma patients treated with R-CHOP.122 Tissue miRNAs seem to be more reliable in the detection and staging of cancer, whereas circulating miRNAs show higher stability and can be measured non-invasively.123
In peripheral T-cell lymphomas, some unique diagnostic miRNA classifiers have been constructed. One 7-miRNA signature (miR-512-3p, miR-886-5p, miR-886-3p, miR-708, miR-135b, miR-146a, and miR-155) is mainly implicated in ALK+ anaplastic large cell lymphoma. miR-155 is present at higher levels in ALK− versus ALK+ anaplastic large cell lymphoma.124 Another 11-miRNA signature (miR-210, miR-197, miR-191, miR-512-3p, miR-451, miR-146a, miR-22, miR-455-3p, miR-455-5p, miR-143, and miR-494) can distinguish ALK− anaplastic large cell lymphoma from other peripheral T-cell lymphomas.125
In summary, some miRNA-based diagnostic and prognostic classifiers have been developed in various types of lymphomas and are expected to improve clinical decision making. Studies on lncRNAs in lymphomas remain rare. With further understanding of their biology and function, lncRNA profiling may also contribute to the diagnosis and prognostication of lymphomas.
Immunophenotypic biomarkers
The basic diagnosis, differential diagnosis and classification of lymphomas are commonly based on histopathological features and the results of immunohistochemistry or flow cytometry immunophenotypic analysis. A number of immunophenotypic biomarkers are routinely used, including T-cell markers (CD2, CD3, CD4, CD5, CD7, CD8, and T-cell receptors), B-cell markers (CD19, CD20, CD22, CD79, and Pax-5), cytotoxic markers (such as TIA-1, granzyme B, and perforin), germinal center markers (CD10, Bcl-6, and LMO2), and plasma cell markers (such as CD38, CD138). In addition, certain markers are highly associated with specific diseases such as CD15, CD30 in classical Hodgkin lymphoma; ALK-1, CD30 in anaplastic large cell lymphoma; cyclin D1 and SOX-11 in mantle cell lymphoma; and follicular T helper cell markers including CXCL13 and PD-1 in angioimmunoblastic T-cell lymphoma. Immunophenotypic markers commonly used in lymphoma diagnosis and classification are shown in Figures 1 and 2. Many protein biomarkers also have been shown to predict lymphoma patient outcomes or are useful in guiding personalized therapy. Figure 3 shows the prognostic value of overexpression of Myc, Bcl-2, Bcl-6, and p53 in diffuse large B-cell lymphoma based on a well-organized large cohort of patients.10, 11, 12, 13
CD30
CD30, a member of the tumor necrosis factor receptor superfamily, is a transmembrane cell-surface marker expressed by activated B or T cells in normal tissues and is highly expressed by tumor cells in classical Hodgkin lymphoma and anaplastic large cell lymphoma, and a subset of diffuse large B-cell lymphoma and Epstein-Barr virus-driven lymphoproliferative disorders.126 Immunohistochemical assessment for CD30 is used commonly as a valuable biomarker for classical Hodgkin lymphoma and anaplastic large cell lymphoma diagnosis; soluble CD30 in serum and/or body fluids can independently predict disease progression and poor outcomes of patients with CD30+ lymphoma.126 As a result of the physiological highly restricted distribution of CD30 expression and dysregulated signaling pathway in lymphoma subtypes, brentuximab vedotin, an antibody drug conjugate composed of anti-CD30 linked to monomethyl auristain E, has been shown to be an effective therapeutic drug for patients with CD30+ lymphomas, especially for patients with relapsed/ refractory Hodgkin lymphoma, systemic anaplastic large cell lymphoma, as well as a subset of patients with refractory/resistant CD30+ diffuse large B-cell lymphoma.126
Bcl-6, Bcl-2, and Myc
Bcl-6 has a critical regulatory role in the programming of germinal center B cells and is considered a unique marker for B cells at the germinal center stage of differentiation. Anti-bcl-6 antibody is often used to mark the germinal center B cells in lymphoma diagnosis, but is not specific for germinal center B-cell-like diffuse large B-cell lymphoma because it is also expressed by post-germinal center cells.17, 127 Bcl-6 is also expressed by the neoplastic T-cells of angioimmunoblastic T-cell lymphoma which are derived from normal follicular T helper cells and can be used as a marker of angioimmunoblastic T-cell lymphomas.16 In addition, Bcl-6 expression together with a simple karyotype can be used as a marker of better survival in patients with IG-MYC positive high-grade B-cell lymphomas.128
Myc and Bcl-2 overexpression are attributable to chromosomal translocations such as t(8;14)(q24;q32) and t(14;18)(q32;q21) and are of specific diagnostic value for Burkitt lymphoma and follicular lymphoma, respectively.22, 28 Overexpression of Myc and/or Bcl-2, however, is often identified in lymphomas with the absence of these translocations. Immunohistochemically, data are inconsistent regarding any prognostic value for Bcl-2, Myc, or Bcl-6 expression as a single marker in lymphomas. Other studies, however, have shown that coexpression of Myc/Bcl-2 in diffuse large B-cell lymphoma is associated with aggressive clinical features and inferior outcomes, independent of those cases with cytogenetically proven (traditional) MYC and BCL2 double-hit diffuse large B-cell lymphoma.129 Myc/Bcl-2 coexpression occurs more frequently in activated B-cell-like diffuse large B-cell lymphoma and may explain the poorer prognosis of activated B-cell-like diffuse large B-cell lymphoma,129 whereas Myc/Bcl-6 coexpression occurs in both germinal center B-cell-like diffuse large B-cell lymphoma and activated B-cell-like diffuse large B-cell lymphoma and does not correlate with outcome. Similarly, Myc expression in mantle cell lymphoma is often associated with aggressive histological variants and poorer prognosis.130
Cyclin D1 and SOX-11
Cyclin D1 is overexpressed as a consequence of the t(11;14)(q13;q32) and is a diagnostic hallmark of mantle cell lymphoma.131 Rare cases of mantle cell lymphoma are reported that are negative for cyclin D1, but have a gene expression prolife consistent with mantle cell lymphoma and these tumors can overexpress cyclin D2 or D3. A subset of these cases has a cyclin D2 translocation.132 In addition, SOX-11 is a marker of mantle cell lymphoma independent of cyclin D1.21, 133 Therefore, the combination of cyclin D1 and SOX-11 has utility for the diagnosis of mantle cell lymphoma, and SOX-11 is especially helpful for cyclin D1-negative cases.134 SOX-11 expression in mantle cell lymphoma patients treated with intensive chemotherapy is associated with improved survival. This observation may be explained by the fact that SOX11-target genes may affect transcriptional regulation of WNT and other biological pathways.135
Cyclin D1 is also overexpressed in about 3% of diffuse large B-cell lymphoma cases, which usually have a post-germinal center or activated B-cell phenotype, negative for CD10 and positive for Bcl-6 and multiple myeloma oncogene 1(MUM-1/IRF4); expression of cyclin D1 in diffuse large B-cell lymphoma is not a consequence of t(11;14) as the translocation is absent.131, 136
p53 and MDM2
Whether expression of p53, usually assessed by IHC, can predict survival in lymphoma patients remains inconsistent. In diffuse large B-cell lymphoma patients treated with R-CHOP, p53 overexpression predicted a worse survival and could be used to stratify patients into different prognostic groups.10 Interestingly, in diffuse large B-cell lymphoma patients, MDM2 expression was shown to not be an independent predictor of patient outcome, but MDM2 expression combined with mutated-type p53 expression could predict significantly poorer survival.137
p63 and Cancerous Inhibitor of Protein Phosphatase 2A (CIP2A)
TP73L, also known as p63, is expressed in all cases of primary mediastinal B-cell lymphoma, but not in classical Hodgkin lymphoma, suggesting that TP73L is useful for distinguishing primary mediastinal B-cell lymphoma from mediastinal classical Hodgkin lymphoma.138 CIP2A, a human oncoprotein, is expressed extensively in several cancers including diffuse large B-cell lymphoma. The extent of CIP2A staining is associated with the proliferation rate and the stage of diffuse large B-cell lymphoma, and may be the result of high tumor load during the disease development.139
Immunophenotypic Algorithms
Gene expression profiling can divide diffuse large B-cell lymphoma cases into at least two distinct molecular subtypes: germinal center B-cell-like subtype and activated B-cell-like subtype.140 As gene expression profiling is not routinely available in clinical practice, a number of investigators have developed immunophenotypic algorithms as surrogates for gene expression profiling (Figure 4). Bcl-2, Bcl-6, CD10, MUM-1/IRF4, forkhead box protein 1 (FOXP1), and GC expressed transcript 1 (GCET1) have been integrated into such immunohistochemical algorithms to subclassify diffuse large B-cell lymphoma basing on cell of origin.141, 142, 143, 144 Among these algorithms, the Hans algorithm is most often used and was established on a CHOP-treated cohort of patients.142 The concordance between gene expression profiling and immunohistochemical algorithms, however, is variable. The Hans algorithm matches gene expression profiling-defined subtypes in about 80% of cases. Other algorithms, such as Choi and Visco/Young algorithms, show a higher concordance (~90%) with gene expression profiling results.141, 142, 143, 144 Despite these limitations, these immunohistochemical algorithms are used because they are readily available, simple and of low cost.

Molecular classification of DLBCL by immunophenotypic algorithms (a–f). Gene expression profiling has divided DLBCL into at least two subtypes: GCB and ABC. In an attempt to drive this concept in routine practice, Bcl-2, Bcl-6, CD10, MUM-1, FOXP1, and GCET1 have been integrated into immunohistochemical algorithms for DLBCL diagnostic workup, based on the expression of specific biomarkers at sequential stages of differentiation of mature B-cell through the GC (a–e). ABC, activated B-cell; DLBCL, diffuse large B-cell lymphoma; FOXP1, forkhead box protein 1; GCB, germinal center B-cell; GCET1, germinal center expressed transcript1; GEP, Gene expression profiling; IHC, immunohistochemistry; MUM-1, multiple myeloma oncogene 1 (also known as interferon regulatory factor 4).
Besides serving a role in these classifiers, some of these biomarkers also have independent prognostic value. The expression of LMO2 and GCET1 has been shown to correlate with better survival in patients with diffuse large B-cell lymphoma. By contrast, expression of MUM-1/IFR4 and FOXP1, post-germinal center markers, are markers of poorer prognosis.142, 145 Interestingly, FOXP1 was shown to be a poor prognostic factor in the pre-rituximab era,146 but not in patients treated with rituximab.147
Immunophenotypic Biomarkers Involved in Oncogenic Signaling Pathways
Expression of some components of oncogenic signaling pathways also has been shown to have prognostic significance. Expression of cyclin D2, cyclin D3, protein kinase c-B, caspase-9, and survivin correlate with a worse prognosis in diffuse large B-cell lymphoma.148, 149, 150, 151 In particular, survivin was implicated in the inferior outcome of activated B-cell-like diffuse large B-cell lymphoma patients treated with R-CHOP.152 Constitutive activation of the NF-κB pathway (Figure 5) contributes to lymphomagenesis in several lymphoma types including diffuse large B-cell lymphoma, classical Hodgkin lymphoma, primary mediastinal B-cell lymphoma, and anaplastic large cell lymphoma.153, 154 Expression of components of the NF-κB pathway, such as p50 (NFκB1) and p65 (RelA), has been associated with activated B-cell-like diffuse large B-cell lymphoma and a worse prognosis,40, 155 whereas p52/RelB may identify a subgroup of germinal center B-cell-like diffuse large B-cell lymphoma patients with a good prognosis.156 Nuclear expression of c-Rel was not shown to correlate with REL amplification or a consistent prognostic impact in patients with diffuse large B-cell lymphoma treated with R-CHOP.157, 158 Aberrant activation of the B-cell receptor signaling pathway, leading to the NF-kB, MAPK, and NFAT pathways, has an important role in lymphomagenesis of many types of lymphoma, particularly in chronic lymphocytic leukemia/small lymphocytic lymphoma and diffuse large B-cell lymphoma. Bruton tyrosine kinase (Btk), one of critical components of the B-cell receptor pathway, has become a major therapeutic target. Its inhibitor, ibrutinib, shows promising efficacy in patients with relapsed/refractory chronic lymphocytic leukemia/small lymohocytic lymphoma, mantle lymphoma, follicular lymphoma, activated B-cell-like diffuse large B-cell lymphoma, lymphoplasmacytic lymphoma/Waldenstrom macroglobulinemia, primary diffuse large B-cell lymphoma of the central nervous system, and marginal zone lymphomas which also have aberrant Btk activity.159, 160

Dysregulated signaling pathways involved in lymphomas. Several aberrantly activated regulatory pathways are involved in lymphomagenesis. Among them, the NF-κB and BCR pathways are most commonly aberrantly activated. Some key components of these pathways and relevant upstream and downstream molecules are emerging as biomarkers to yield prognostic and therapeutic information. BAFF-R, B-cell activating factor receptor; BCR, B-cell receptor; BTK, Bruton’s tyrosine kinase; CARD11, caspase recruitment domain family, member 11; IKK, IκB kinase; MALT1, mucosa-associated lymphoid tissue lymphoma translocation protein 1; NEMO, NF-κB essential modifier; NIK, NF-κB-inducing kinase; mTOR, mammalian target of rapamycin; PI3K, phosphatidylinositol 3 kinase; TCR, T-cell receptor; TLRs, Toll-like receptors; TNFR, tumor necrosis factor receptor.
Immunohistochemical Biomarkers Helpful in the Differential Diagnosis of Common Types of Peripheral T-Cell Lymphoma
Biomarkers that can be assessed by immunohistochemistry are extremely helpful for distinguishing between two entities that share morphological and histopathological features, and they can be applied simply as a part of routine clinical practice. For example, there can be overlap between classical Hodgkin lymphoma and angioimmunoblastic T-cell lymphoma and the latter can have Epstein-Barr virus (EBV) -positive large cells that resemble Hodgkin Reed-Sternberg cells both morphologically and phenotypically.161 In this situation, accurate diagnosis may be aided by immunophenotypic expression of CD10, PD-1 and CXCL13 in angioimmunoblastic T-cell lymphoma.162, 163 In addition, CXCL13 and PD-1 are particularly useful in the differential diagnosis between angioimmunoblastic T-cell lymphoma and EBV+ diffuse large B-cell lymphoma, angioimmunoblastic T-cell lymphoma versus EBV+ classical Hodgkin lymphoma, and angioimmunoblastic T-cell lymphoma versus the follicular variant of peripheral T-cell lymphoma, not otherwise specified. Cases of the follicular variant of peripheral T-cell lymphoma, not otherwise specified do not have expansion of follicular dendritic cell meshworks outside the follicles and no prominent inflammatory background, but Hodgkin-like cells can be present.161, 163 SAP, an additional immunohistochemical marker of germinal center T cells, also has diagnostic value for angioimmunoblastic T-cell lymphoma, especially in combination with PD-1 and CXCL13.164 Other follicular helper T-cells biomarkers characteristically expressed by angioimmunoblastic T-cell lymphoma cells include ICOS, CD200, and c-Maf.165, 166, 167 In practice, these immunohistochemical biomarkers are of great importance in the diagnosis of angioimmunoblastic cell lymphoma and the differential diagnosis with other lymphomas.
T-cell-restricted intracellular antigen-1 (TIA-1), granzyme B, and perforin are cytotoxic biomarkers that are commonly used to diagnose NK/T lymphomas. Anaplastic large cell lymphoma is another type of lymphoma in which the neoplastic cells are positive for cytotoxic biomarkers. For anaplastic large cell lymphoma, clusterin is another potentially useful diagnostic marker.168 Granzyme H more recently has been shown to be a biomarker of NK and T-cell lymphoma and may be useful in the differential diagnosis between NK/T lymphomas and other peripheral T-cell lymphomas with cytotoxic features.169
The Jun family (c-Jun, JunB, JunD) is a member of the activator protein-1 (AP1) pathway which is involved in cell differentiation, proliferation, survival and apoptosis.170 c-Jun, JunB, and JunD are overexpressed in several cancers, including lymphomas.171, 172 An early study indicated that c-Jun and JunB were expressed strongly in the tumor cells of classical Hodgkin lymphoma and anaplastic large cell lymphoma, but not in B-cell non-Hodgkin lymphomas, indicating their potential to serve as diagnostic tools and therapeutic targets.171 Increased coexpression of galectin-1 and c-Jun in tumor cells of classical Hodgkin lymphoma and anaplastic large cell lymphoma patients has been observed, suggesting that this combination of biomarkers can distinguish classical Hodgkin lymphoma and anaplastic large cell lymphoma from other lymphomas with similar morphological and molecular features. It seems reasonable to suggest that inhibition of galectin-1, an AP1 target, may represent a potential treatment strategy for patients with classical Hodgkin lymphoma and anaplastic large cell lymphoma.173 Moreover, serum levels of galectin-1 were associated with tumor burden and adverse clinical features in a large cohort of classical Hodgkin lymphoma patients.174
Taken together, immunophenotypic biomarkers, mostly assessed by immunohistochemistry, have important roles in the diagnosis and prognostication of lymphomas as well as serving as effective drug targets. However, due to limitations of immunohistochemistry methods, such as the variable quality of antibodies and the difficulty in standardization, objective scoring and interpretation of staining results, the reproducibility and effectiveness of many immunohistochemistry assays need to be confirmed.
Microenvironment-related biomarkers for prognostication and immunotherapy
The tumor microenvironment refers to the extracellular context in which the malignant cells reside, which is commonly a plethora of non-malignant cells and extracellular matrix surrounding the malignant cells. Overwhelming evidence has shown that tumor cells and benign reactive cells in the microenvironment interact with each other dynamically and reciprocally through a variety of cytokines and chemokines that are secreted or expressed by malignant or tumor-infiltrating non-malignant cells (Figure 6). Many studies also have suggested that the microenvironment influences clinical outcome.7, 175, 176 Subsequently, biomarkers reflecting the microenvironment of lymphomas have been discovered and used to predict the clinical outcome of patients. Improved quantitative immunohistochemistry (multiOmyx and Opal assays), in situ hybridization and gene expression profiling are powerful approaches to investigate microenvironmental biomarkers. Table 3 summarizes some of the microenvironmental biomarkers related to lymphoma patient outcomes.

Schematic representation of cHL showing the interaction between HRS cells and their microenvironment through cytokines/chemokine signaling and a summary of microenvironment-related biomarkers for diagnosis and prognosis in lymphomas. Malignant cells and their extracellular context interact with each other dynamically and reciprocally through a variety of cytokines and chemokines secreted or expressed by malignant cells or tumor-infiltrating non-malignant cells in lymphomas, particularly in cHL. Many benign tumor-infiltrating cells that show diagnostic or prognostic significance in lymphomas can be located or numbered through some specific biomarkers detected by immunohistochemistry or gene expression profiling. APRIL, a proliferation-inducing ligand; BCL11A, B-cell lymphoma/leukemia 11A; BLC, B lymphocyte chemoattractant; CCL, Treg, regulatory T-cell; cHL, classical Hodgkin lymphoma; CSF1, colony stimulating factor 1; CTL, cytotoxic T-cell; FASL, Fas ligand; FDC, follicular dendritic cell; HRS, Hodgkin and Reed-Sternberg; IFNγ, interferon gamma; IL, interleukin; NK, natural killer; PD1, programmed death 1; PDL1, programmed death ligand 1; STAT1, signal transducer and activator of transcription 1; SPARC, secreted protein acidic cysteine-rich; Th1, T helper 1; TNFα, tumor necrosis factor-α.
CD21+ Follicular Dendritic Cells
Classical Hodgkin lymphoma is usually characterized by rare neoplastic cells (often <1%) within abundant reactive cells including follicular dendritic cells that comprise the microenvironment. Alavaikko et al177 reported that absence of CD21+ follicular dendritic cells in classical Hodgkin lymphoma predicted an unfavorable outcome. Another study confirmed this association and further showed that not only the number of CD21+ follicular dendritic cells, but also the extent of destruction of normal lymph node architecture, correlates with prognosis.178
Granzyme B+ Tumor-Infiltrating Cytotoxic T Cells
As a microenvironmental biomarker, granzyme B is expressed by tumor-infiltrating cytotoxic T cells that are present in several lymphoma types. Studies have shown a correlation between the number of tumor-infiltrating cytotoxic T cells and clinical outcome in patients with classical Hodgkin lymphoma or anaplastic large cell lymphoma.179, 180
CD117+ Mast Cells
CD117, expressed strongly by mast cells, can be used to evaluate the numbers of mast cells infiltrating in the microenvironment of lymphomas. One study showed that the number of mast cells was associated with unfavorable outcome of patients with classical Hodgkin lymphoma after primary therapy.181 In contrast, another study showed that mast cell infiltration in diffuse large B-cell lymphoma predicts a more favorable outcome.182
CD68+ or CD163+ Macrophages
CD68 and CD163 are expressed mainly by macrophages and can be detected easily by immunohistochemistry. Several studies have shown that an increased number of CD68+ or CD163+ macrophages is associated with poorer prognosis in patients with classical Hodgkin lymphoma or follicular lymphoma.183, 184 However, there are some inconsistent results,185 suggesting the need to validate study cohorts or methods. For diffuse large B-cell lymphoma, macrophages appear to have a dual, treatment-specific role. CD68+ macrophage numbers together with high pretreatment CD68 mRNA levels can predict a favorable outcome for diffuse large B-cell lymphoma patients treated with chemoimmunotherapy.186 Interestingly, CD163+ macrophages are useful as a prognostic indicator in pediatric classical Hodgkin lymphoma patients and this observation seems to be dependent on EBV status. It was demonstrated that high numbers of CD163+ and granzyme B+ cells are associated with inferior progression-free survival in patients with EBV negative rather than EBV positive cases of classical Hodgkin lymphoma.187
FOXP3+ Regulatory T Cells
An increased number of tumor-infiltrating FOXP3+ regulatory T cells has been shown to convey a better prognosis in many types of lymphoma, including follicular lymphoma, Hodgkin lymphoma and NK/T-cell lymphomas.188, 189, 190 It was speculated that tumor-infiltrating FOXP3+ regulatory T cells might suppress neoplastic cells in a TGF-β-mediated fashion and thereby form an inhibitory tumor microenvironment in lymphomas, at least in NK/T-cell lymphomas.190 A similar predictive trend can work for NK/T-cell lymphoma patients after IMEP chemotherapy alone and IMEP-based chemo- or chemo-radiotherapy.190 In patients with diffuse large B-cell lymphoma, the prognostic impact of tumor-infiltrating FOXP3+ regulatory T cells is debatable.191, 192
PD-1 and PD-L1
PD-1 (CD279) is expressed by tumor-infiltrating T cells in several types of lymphoma, whereas PD-L1 and PD-L2 (CD274 and CD273), the ligands of PD-1, are expressed by the malignant cells and tumor-infiltrating antigen presenting cells. High numbers of PD-1+ infiltrating T cells have been associated with inferior overall survival of classical Hodgkin lymphoma patients, respective of the disease stage.193 Furthermore, the existence of PD-1+ reactive T cells rosettes is recognized as a characteristic of nodular lymphocyte predominant Hodgkin lymphoma.194 In diffuse large B-cell lymphoma or follicular lymphoma, the prognostic value of PD-1+ tumor-infiltrating T-cell subsets is controversial,195, 196 but the expression of PD-L1 in tissue and PD-L1 levels in peripheral blood have been reported to be of independent prognostic or disease monitoring value.197, 198 Importantly, immunotherapeutic trials blocking PD-1 are successfully ongoing in lymphomas and have also seen great progresses in solid tumors. Agents that block PD-L1 are in extensive development.199, 200
CD58 and Tumor Necrosis Factor Receptor Superfamily Member 14 (TNFRSF14)
CD58 is the receptor of CD2 which is expressed mainly by T cells and NK cells.201 Decreased expression of CD58 can be observed in two-thirds of activated B-cell-like diffuse large B-cell lymphoma and one third of germinal center B-cell-like diffuse large B-cell lymphoma. Inactive CD58 may contribute to immune escape by disrupting the interaction between CD58 and CD2 and consequently facilitate other genetic defects.201, 202 Another genetic alteration involved in immune escape is TNFRSF14 which functions as a tumor suppressor and regulates immune responses. TNFRSF14 inactivation (via mutation or deletion) has been reported to be associated with poorer outcomes in patients with follicular lymphoma.203
EBV and Other Viruses
Although the pathological role of EBV infection in some types of lymphoma is well established, the contribution of EBV infection to clinical outcome is controversial. EBV positivity tends to be associated with unfavorable outcome in elderly patients with classical Hodgkin lymphoma, whereas the outcome is more favorable in young patients.204, 205 Additional studies have offered supporting evidence to confirm this trend in classical Hodgkin lymphoma and other lymphomas, like diffuse large B-cell lymphoma.206, 207, 208 EBV positivity is seen in ~5% of diffuse large B-cell lymphoma and a worse outcome was reported in Asian, East European and African American patients, but not in North American patients. EBV positivity also has been reported in occasional cases of peripheral T-cell lymphoma, many cases of anaplastic large cell lymphoma and plasmablastic lymphoma, but clinical outcome in these patients needs better validation.
In addition to EBV, other viruses also have been shown to be associated with lymphomagenesis.209, 210, 211 For example, patients with hepatitis B virus-associated diffuse large B-cell lymphoma have unique clinical features and poorer outcomes. Diffuse large B-cell lymphoma patients infected by hepatitis C virus also show good therapeutic responses to antiviral drugs. Human herpesvirus 8 (also known as Kaposi sarcoma-associated herpesvirus) infection is a characteristic of primary effusion lymphoma which occurs mainly in immunocompromised patients. HHV8 infection is also common in multicentric Castleman disease.
Microenvironment-Related Gene Expression Profiling Signatures
Several microenvironment-related gene expression profiling signatures have been established. STAT1 and ALDH1A1, expressed by macrophages, have been shown to correlate with adverse outcome.212 CD8B1, CD3D, CTSL, CD26, SH2D1A as a cytotoxic T-cell signature was shown to be associated with an inferior outcome in some studies.212, 213, 214 LYZ and STAT are expressed by tissue monocytes and activated macrophages. High levels of LYZ and STAT1 expression were correlated with prolonged failure-free survival and better outcome in patients with classical Hodgkin lymphoma.215
Gene expression profiling-based stromal gene signatures have been identified and shown to be in accord with gene expression profiling-based subgroups of diffuse large B-cell lymphoma. The activated B-cell-like subtype has an unfavorable stromal-2 signature with expression of angiogenesis markers (such as CXCL12, KDR, and CD31). In contrast, the germinal center B-cell-like subtype has a favorable stromal-1 signature with extracellular matrix deposition (biomarkers such as FN1, MMP9, CTGF, and SPARC).216
The interaction between tumor cells and their microenvironment is dynamic and complex, which may lead to uncertainty about the evaluation of microenvironment-related biomarkers. It is necessary to take cellular and matrix factors into consideration when such microenvironmental biomarkers are used.217, 218
Conclusions
The application of new generation detection platforms provides an opportunity for the assessment of genomic and transcriptomic biomarkers in lymphomas. Discovery of molecular biomarkers not only enhances our understanding of pathogenetic mechanisms in lymphomas, but also provides opportunities to refine classification, to improve accuracy of diagnosis, and to stratify the outcomes of lymphoma patients, especially in combination with classical immunophenotypic biomarkers. Nevertheless, the discovery and exploration of additional novel biomarkers lead to challenges as we need to select, validate, and translate these markers into clinical practice. Other factors, such as methods, reproducibility, quality of reagents, data interpretation, and cost efficiency, need to be taken into consideration. In particular, biomarkers used to guide treatment decisions must be reliable and reproducible. The integration of diagnosis, prognostication, and the assessment of therapeutic targets will become the norm in the assessment of lymphomas and these tasks will depend on effective application of diagnostically reliable and therapeutically meaningful biomarkers.
References
Swerdlow SH, Campo E, Harris NL et alWorld Health Organization Classification of Tumours of Haematopoietic and Lymphoid Tissues. LARK: Lyon, 2008.
Hanahan D, Weinberg RA . Hallmarks of cancer: the next generation. Cell 2011;144:646–674.
Scott DW, Gascoyne RD . The tumour microenvironment in B cell lymphomas. Nat Rev Cancer 2014;14:517–534.
Shaffer AL 3rd, Young RM, Staudt LM . Pathogenesis of human B cell lymphomas. Annu Rev Immunol 2012;30:565–610.
Iqbal J, Shen Y, Huang X et al. Global microRNA expression profiling uncovers molecular markers for classification and prognosis in aggressive B-cell lymphoma. Blood 2015;125:1137–1145.
Iqbal J, Wright G, Wang C et al. Gene expression signatures delineate biological and prognostic subgroups in peripheral T-cell lymphoma. Blood 2014;123:2915–2923.
Steidl C, Connors JM, Gascoyne RD . Molecular pathogenesis of Hodgkin's lymphoma: increasing evidence of the importance of the microenvironment. J Clin Oncol 2011;29:1812–1826.
Soldini D, Campo E . New insights into the diagnosis of lymphomas. Ann Oncol 2012;23:x83–x88.
Campo E . Whole genome profiling and other high throughput technologies in lymphoid neoplasms-current contributions and future hopes. Mod Pathol 2013;26:S97–S110.
Xu-Monette ZY, Wu L, Visco C et al. Mutational profile and prognostic significance of TP53 in diffuse large B-cell lymphoma patients treated with R-CHOP: report from an International DLBCL Rituximab-CHOP Consortium Program Study. Blood 2012;120:3986–3996.
Xu-Monette ZY, Dabaja BS, Wang X et al. Clinical features, tumor biology, and prognosis associated with MYC rearrangement and Myc overexpression in diffuse large B-cell lymphoma patients treated with rituximab-CHOP. Mod Pathol 2015;28:1555–1573.
Ye Q, Xu-Monette ZY, Tzankov A et al. Prognostic impact of concurrent MYC and BCL6 rearrangements and expression in de novo diffuse large B-cell lymphoma. Oncotarget 2016;7:2401–2416.
Tzankov A, Xu-Monette ZY, Gerhard M et al. Rearrangements of MYC gene facilitate risk stratification in diffuse large B-cell lymphoma patients treated with rituximab-CHOP. Mod Pathol 2014;27:958–971.
Basso K, Dalla-Favera R . BCL6: master regulator of the germinal center reaction and key oncogene in B cell lymphomagenesis. Adv Immunol 2010;105:193–210.
Ye BH, Lista F, Lo Coco F et al. Alterations of a zinc finger-encoding gene, BCL-6, in diffuse large-cell lymphoma. Science 1993;262:747–750.
Wagner SD, Ahearne M, Ko Ferrigno P . The role of BCL6 in lymphomas and routes to therapy. Br J Haematol 2011;152:3–12.
Capello D, Vitolo U, Pasqualucci L et al. Distribution and pattern of BCL-6 mutations throughout the spectrum of B-cell neoplasia. Blood 2000;95:651–659.
Lossos IS, Jones CD, Warnke R et al. Expression of a single gene, BCL-6, strongly predicts survival in patients with diffuse large B-cell lymphoma. Blood 2001;98:945–951.
Iqbal J, Greiner TC, Patel K et al. Distinctive patterns of BCL6 molecular alterations and their functional consequences in different subgroups of diffuse large B-cell lymphoma. Leukemia 2007;21:2332–2343.
Xu-Monette ZY, Medeiros LJ, Li Y et al. Dysfunction of the TP53 tumor suppressor gene in lymphoid malignancies. Blood 2012;119:3668–3683.
Vose JM . Mantle cell lymphoma: 2013 Update on diagnosis, risk-stratification, and clinical management. Am J Hematol 2013;88:1082–1088.
Meyer N, Penn LZ . MYC - TIMELINE Reflecting on 25 years with MYC. Nat Rev Cancer 2008;8:976–990.
Dang CV . MYC on the path to cancer. Cell 2012;149:22–35.
Hao S, Sanger W, Onciu M et al. Mantle cell lymphoma with 8q24 chromosomal abnormalities: a report of 5 cases with blastoid features. Mod Pathol 2002;15:1266–1272.
Ott G, Rosenwald A, Campo E . Understanding MYC-driven aggressive B-cell lymphomas: pathogenesis and classification. Blood 2013;122:3884–3891.
Savage KJ, Johnson NA, Ben-Neriah S et al. MYC gene rearrangements are associated with a poor prognosis in diffuse large B-cell lymphoma patients treated with R-CHOP chemotherapy. Blood 2009;114:3533–3537.
Barrans S, Crouch S, Smith A et al. Rearrangement of MYC is associated with poor prognosis in patients with diffuse large B-cell lymphoma treated in the era of rituximab. J Clin Oncol 2010;28:3360–3365.
Freedman A . Follicular lymphoma: 2014 update on diagnosis and management. Am J Hematol 2014;89:429–436.
Iqbal J, Sanger WG, Horsman DE et al. BCL2 translocation defines a unique tumor subset within the germinal center B-cell-like diffuse large B-cell lymphoma. Am J Pathol 2004;165:159–166.
Lenz G, Wright GW, Emre NC et al. Molecular subtypes of diffuse large B-cell lymphoma arise by distinct genetic pathways. Proc Natl Acad Sci USA 2008;105:13520–13525.
Kendrick SL, Redd L, Muranyi A et al. BCL2 antibodies targeted at different epitopes detect varying levels of protein expression and correlate with frequent gene amplification in diffuse large B-cell lymphoma. Hum Pathol 2014;45:2144–2153.
Copie-Bergman C, Gaulard P, Leroy K et al. Immuno-fluorescence in situ hybridization index predicts survival in patients with diffuse large B-cell lymphoma treated with R-CHOP: A GELA Study. J Clin Oncol 2009;27:5573–5579.
Iqbal J, Meyer PN, Smith LM et al. BCL2 predicts survival in germinal center B-cell-like diffuse large B-cell lymphoma treated with CHOP-like therapy and rituximab. Clin Cancer Res 2011;17:7785–7795.
Visco C, Tzankov A, Xu-Monette ZY et al. Patients with diffuse large B-cell lymphoma of germinal center origin with BCL2 translocations have poor outcome, irrespective of MYC status: a report from an International DLBCL rituximab-CHOP Consortium Program Study. Haematologica 2013;98:255–263.
Friedberg JW . Double-hit diffuse large B-cell lymphoma. J Clin Oncol 2012;30:3439–3443.
Ngo VN, Young RM, Schmitz R et al. Oncogenically active MYD88 mutations in human lymphoma. Nature 2011;470:115–119.
Choi JW, Kim Y, Lee JH, Kim YS . MYD88 expression and L265P mutation in diffuse large B-cell lymphoma. Hum Pathol 2013;44:1375–1381.
Treon SP, Xu L, Yang G et al. MYD88 L265P somatic mutation in Waldenstrom's macroglobulinemia. N Engl J Med 2012;367:826–833.
Kim Y, Ju H, Kim DH et al. CD79B and MYD88 mutations in diffuse large B-cell lymphoma. Hum Pathol 2014;45:556–564.
Compagno M, Lim WK, Grunn A et al. Mutations of multiple genes cause deregulation of NF-kappaB in diffuse large B-cell lymphoma. Nature 2009;459:717–721.
Kato M, Sanada M, Kato I et al. Frequent inactivation of A20 in B-cell lymphomas. Nature 2009;459:712–716.
Honma K, Tsuzuki S, Nakagawa M et al. TNFAIP3/A20 functions as a novel tumor suppressor gene in several subtypes of non-Hodgkin lymphomas. Blood 2009;114:2467–2475.
Steidl C, Shah SP, Woolcock BW et al. MHC class II transactivator CIITA is a recurrent gene fusion partner in lymphoid cancers. Nature 2011;471:377–381.
Mottok A, Woolcock B, Chan FC et al. Genomic alterations in CIITA are frequent in primary mediastinal large B cell lymphoma and are associated with diminished MHC class II expression. Cell Rep 2015;13:1418–1431.
Pasqualucci L, Trifonov V, Fabbri G et al. Analysis of the coding genome of diffuse large B-cell lymphoma. Nat Genet 2011;43:830–833.
Rimsza LM, Chan WC, Gascoyne RD et al. CIITA or RFX coding region loss of function mutations occur rarely in diffuse large B-cell lymphoma cases and cell lines with low levels of major histocompatibility complex class II expression. Haematologica 2009;94:596–598.
Rimsza LM, Wright G, Schwartz M et al. Accurate classification of diffuse large B-cell lymphoma into germinal center and activated B-cell subtypes using a nuclease protection assay on formalin-fixed, paraffin-embedded tissues. Clin Cancer Res 2011;17:3727–3732.
Scott DW, Wright GW, Williams PM et al. Determining cell-of-origin subtypes of diffuse large B-cell lymphoma using gene expression in formalin-fixed paraffin-embedded tissue. Blood 2014;123:1214–1217.
Collie AM, Nolling J, Divakar KM et al. Molecular subtype classification of formalin-fixed, paraffin-embedded diffuse large B-cell lymphoma samples on the ICEPlex(R) system. Br J Haematol 2014;167:281–285.
Lossos IS, Czerwinski DK, Alizadeh AA et al. Prediction of survival in diffuse large-B-cell lymphoma based on the expression of six genes. N Engl J Med 2004;350:1828–1837.
Alizadeh AA, Gentles AJ, Alencar AJ et al. Prediction of survival in diffuse large B-cell lymphoma based on the expression of 2 genes reflecting tumor and microenvironment. Blood 2011;118:1350–1358.
Love C, Sun Z, Jima D et al. The genetic landscape of mutations in Burkitt lymphoma. Nat Genet 2012;44:1321–1325.
Fernandez V, Salamero O, Espinet B et al. Genomic and gene expression profiling defines indolent forms of mantle cell lymphoma. Cancer Res 2010;70:1408–1418.
Hartmann E, Fernandez V, Moreno V et al. Five-gene model to predict survival in mantle-cell lymphoma using frozen or formalin-fixed, paraffin-embedded tissue. J Clin Oncol 2008;26:4966–4972.
Pastore A, Jurinovic V, Kridel R et al. Integration of gene mutations in risk prognostication for patients receiving first-line immunochemotherapy for follicular lymphoma: a retrospective analysis of a prospective clinical trial and validation in a population-based registry. Lancet Oncol 2015;16:1111–1122.
Eberle FC, Rodriguez-Canales J, Wei L et al. Methylation profiling of mediastinal gray zone lymphoma reveals a distinctive signature with elements shared by classical Hodgkin's lymphoma and primary mediastinal large B-cell lymphoma. Haematologica 2011;96:558–566.
Eberle FC, Salaverria I, Steidl C et al. Gray zone lymphoma: chromosomal aberrations with immunophenotypic and clinical correlations. Mod Pathol 2011;24:1586–1597.
Guiter C, Dusanter-Fourt I, Copie-Bergman C et al. Constitutive STAT6 activation in primary mediastinal large B-cell lymphoma. Blood 2004;104:543–549.
Steidl C, Gascoyne RD . The molecular pathogenesis of primary mediastinal large B-cell lymphoma. Blood 2011;118:2659–2669.
Takahashi H, Feuerhake F, Monti S et al. Lack of IKBA coding region mutations in primary mediastinal large B-cell lymphoma and the host response subtype of diffuse large B-cell lymphoma. Blood 2006;107:844–845.
Iqbal J, Weisenburger DD, Greiner TC et al. Molecular signatures to improve diagnosis in peripheral T-cell lymphoma and prognostication in angioimmunoblastic T-cell lymphoma. Blood 2010;115:1026–1036.
Amin HM, Lai R . Pathobiology of ALK+ anaplastic large-cell lymphoma. Blood 2007;110:2259–2267.
Feldman AL, Dogan A, Smith DI et al. Discovery of recurrent t(6;7)(p25.3;q32.3) translocations in ALK-negative anaplastic large cell lymphomas by massively parallel genomic sequencing. Blood 2011;117:915–919.
Parrilla Castellar ER, Jaffe ES, Said JW et al. ALK-negative anaplastic large cell lymphoma is a genetically heterogeneous disease with widely disparate clinical outcomes. Blood 2014;124:1473–1480.
Vose J, Armitage J, Weisenburger D . International TCLP. International Peripheral T-cell and Natural Killer/T-cell Lymphoma Study: pathology findings and clinical outcomes. J Clin Oncol 2008;26:4124–4130.
Gerber DE, Minna JD . ALK inhibition for non-small cell lung cancer: from discovery to therapy in record time. Cancer cell 2010;18:548–551.
Morice WG, Jevremovic D, Olteanu H et al. Chronic lymphoproliferative disorder of natural killer cells: a distinct entity with subtypes correlating with normal natural killer cell subsets. Leukemia 2010;24:881–884.
Morice WG . The immunophenotypic attributes of NK cells and NK-cell lineage lymphoproliferative disorders. Am J Clin Pathol 2007;127:881–886.
Haedicke W, Ho FC, Chott A et al. Expression of CD94/NKG2A and killer immunoglobulin-like receptors in NK cells and a subset of extranodal cytotoxic T-cell lymphomas. Blood 2000;95:3628–3630.
Streubel B, Vinatzer U, Willheim M et al. Novel t(5;9)(q33;q22) fuses ITK to SYK in unspecified peripheral T-cell lymphoma. Leukemia 2006;20:313–318.
Huang Y, Moreau A, Dupuis J et al. Peripheral T-cell lymphomas with a follicular growth pattern are derived from follicular helper T cells (TFH) and may show overlapping features with angioimmunoblastic T-cell lymphomas. Am J Surg Pathol 2009;33:682–690.
Dawson MA, Kouzarides T . Cancer epigenetics: from mechanism to therapy. Cell 2012;150:12–27.
Shi H, Guo J, Duff DJ et al. Discovery of novel epigenetic markers in non-Hodgkin's lymphoma. Carcinogenesis 2007;28:60–70.
Esteller M . Profiling aberrant DNA methylation in hematologic neoplasms: a view from the tip of the iceberg. Clin Immunol 2003;109:80–88.
Uchida T, Watanabe T, Kinoshita T et al. Mutational analysis of the Cdkn2 (Mts1/P16(Ink4a)) gene in primary B-cell lymphomas. Blood 1995;86:2724–2731.
Gombart AF, Morosetti R, Miller CW et al. Deletions of the cyclin-dependent kinase inhibitor genes P16(Ink4a) and P15(Ink4b) in non-Hodgkins-lymphomas. Blood 1995;86:1534–1539.
Herman JG, Civin CI, Issa JPJ et al. Distinct patterns of inactivation of p15(INK4B) and p16(INK4A) characterize the major types of hematological malignancies. Cancer Res 1997;57:837–841.
Zainuddin N, Kanduri M, Berglund M et al. Quantitative evaluation of p16(INK4a) promoter methylation using pyrosequencing in de novo diffuse large B-cell lymphoma. Leuk Res 2011;35:438–443.
Jiang Y, Hatzi K, Shaknovich R . Mechanisms of epigenetic deregulation in lymphoid neoplasms. Blood 2013;121:4271–4279.
Esteller M, Gaidano G, Goodman SN et al. Hypermethylation of the DNA repair gene O-6-methylguanine DNA methyltransferase and survival of patients with diffuse large B-cell lymphoma. J Natl Cancer Inst 2002;94:26–32.
Guan H, Xie L, Leithauser F et al. KLF4 is a tumor suppressor in B-cell non-Hodgkin lymphoma and in classic Hodgkin lymphoma. Blood 2010;116:1469–1478.
Morin RD, Mendez-Lago M, Mungall AJ et al. Frequent mutation of histone-modifying genes in non-Hodgkin lymphoma. Nature 2011;476:298–303.
Ying CY, Dominguez-Sola D, Fabi M et al. MEF2B mutations lead to deregulated expression of the oncogene BCL6 in diffuse large B cell lymphoma. Nat Immunol 2013;14:1084–1092.
Bodor C, Grossmann V, Popov N et al. EZH2 mutations are frequent and represent an early event in follicular lymphoma. Blood 2013;122:3165–3168.
Morin RD, Johnson NA, Severson TM et al. Somatic mutations altering EZH2 (Tyr641) in follicular and diffuse large B-cell lymphomas of germinal-center origin. Nat Genet 2010;42:181–185.
Lohr JG, Stojanov P, Lawrence MS et al. Discovery and prioritization of somatic mutations in diffuse large B-cell lymphoma (DLBCL) by whole-exome sequencing. Proc Natl Acad Sci USA 2012;109:3879–3884.
Lee HJ, Shin DH, Kim KB et al. Polycomb protein EZH2 expression in diffuse large B-cell lymphoma is associated with better prognosis in patients treated with rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone. Leuk Lymphoma 2014;55:2056–2063.
Heyn H, Esteller M . EZH2: an epigenetic gatekeeper promoting lymphomagenesis. Cancer Cell 2013;23:563–565.
Enjuanes A, Fernandez V, Hernandez L et al. Identification of methylated genes associated with aggressive clinicopathological features in mantle cell lymphoma. PloS One 2011;6:e19736.
Bethge N, Lothe RA, Honne H et al. Colorectal cancer DNA methylation marker panel validated with high performance in non-Hodgkin lymphoma. Epigenetics 2014;9:428–436.
Shaknovich R, Geng H, Johnson NA et al. DNA methylation signatures define molecular subtypes of diffuse large B-cell lymphoma. Blood 2010;116:e81–e89.
Clozel T, Yang S, Elstrom RL et al. Mechanism-based epigenetic chemosensitization therapy of diffuse large B-cell lymphoma. Cancer Discov 2013;3:1002–1019.
Leshchenko VV, Kuo PY, Jiang Z et al. Integrative genomic analysis of temozolomide resistance in diffuse large B-cell lymphoma. Clin Cancer Res 2014;20:382–392.
Palomero T, Couronne L, Khiabanian H et al. Recurrent mutations in epigenetic regulators, RHOA and FYN kinase in peripheral T cell lymphomas. Nat Genet 2014;46:166–170.
Cairns RA, Iqbal J, Lemonnier F et al. IDH2 mutations are frequent in angioimmunoblastic T-cell lymphoma. Blood 2012;119:1901–1903.
Lemonnier F, Couronne L, Parrens M et al. Recurrent TET2 mutations in peripheral T-cell lymphomas correlate with TFH-like features and adverse clinical parameters. Blood 2012;120:1466–1469.
Wang C, McKeithan TW, Gong Q et al. IDH2R172 mutations define a unique subgroup of patients with angioimmunoblastic T-cell lymphoma. Blood 2015;126:1741–1752.
Marques SC, Laursen MB, Bodker JS et al. MicroRNAs in B-cells: from normal differentiation to treatment of malignancies. Oncotarget 2015;6:7–25.
Schetter AJ, Leung SY, Sohn JJ et al. MicroRNA expression profiles associated with prognosis and therapeutic outcome in colon adenocarcinoma. JAMA 2008;299:425–436.
Derrien T, Johnson R, Bussotti G et al. The GENCODE v7 catalog of human long noncoding RNAs: analysis of their gene structure, evolution, and expression. Genome Res 2012;22:1775–1789.
Yarmishyn AA, Kurochkin IV . Long noncoding RNAs: a potential novel class of cancer biomarkers. Front Genet 2015;6:145.
Morris KV, Mattick JS . The rise of regulatory RNA. Nat Rev Genet 2014;15:423–437.
Nana-Sinkam SP, Croce CM . MicroRNA regulation of tumorigenesis, cancer progression and interpatient heterogeneity: towards clinical use. Genome Biol 2014;15:445.
Jardin F, Figeac M . MicroRNAs in lymphoma, from diagnosis to targeted therapy. Curr Opin Oncol 2013;25:480–486.
Eis PS, Tam W, Sun L et al. Accumulation of miR-155 and BIC RNA in human B cell lymphomas. Proc Natl Acad Sci USA 2005;102:3627–3632.
Costinean S, Zanesi N, Pekarsky Y et al. Pre-B cell proliferation and lymphoblastic leukemia/high-grade lymphoma in E mu-miR155 transgenic mice. Proc Natl Acad Sci USA 2006;103:7024–7029.
Ota A, Tagawa H, Karnan S et al. Identification and characterization of a novel gene, C13orf25, as a target for 13q31-q32 amplification in malignant lymphoma. Cancer Res 2004;64:3087–3095.
Rao E, Jiang C, Ji M et al. The miRNA-17 similar to 92 cluster mediates chemoresistance and enhances tumor growth in mantle cell lymphoma via PI3K/AKT pathway activation. Leukemia 2012;26:1064–1072.
Merkel O, Hamacher F, Laimer D et al. Identification of differential and functionally active miRNAs in both anaplastic lymphoma kinase (ALK)+ and ALK- anaplastic large-cell lymphoma. Proc Natl Acad Sci USA 2010;107:16228–16233.
Olive V, Bennett MJ, Walker JC et al. miR-19 is a key oncogenic component of mir-17-92. Gene Dev 2009;23:2839–2849.
Spaccarotella E, Pellegrino E, Ferracin M et al. STAT3-mediated activation of microRNA cluster 17~92 promotes proliferation and survival of ALK-positive anaplastic large cell lymphoma. Haematologica 2014;99:116–124.
Musilova K, Mraz M . MicroRNAs in B-cell lymphomas: how a complex biology gets more complex. Leukemia 2015;29:1004–1017.
Dohner H, Stilgenbauer S, Benner A et al. Genomic aberrations and survival in chronic lymphocytic leukemia. N Engl J Med 2000;343:1910–1916.
Husby S, Ralfkiaer U, Garde C et al. miR-18b overexpression identifies mantle cell lymphoma patients with poor outcome and improves the MIPI-B prognosticator. Blood 2015;125:2669–2677.
Zhao JJ, Lin JH, Lwin T et al. microRNA expression profile and identification of miR-29 as a prognostic marker and pathogenetic factor by targeting CDK6 in mantle cell lymphoma. Blood 2010;115:2630–2639.
Goswami RS, Atenafu EG, Xuan YL et al. MicroRNA signature obtained from the comparison of aggressive with indolent non-Hodgkin lymphomas: potential prognostic value in Mantle-cell lymphoma. J Clin Oncol 2013;31:2903–2911.
Mazan-Mamczarz K, Gartenhaus RB . Role of microRNA deregulation in the pathogenesis of diffuse large B-cell lymphoma (DLBCL). Leuk Res 2013;37:1420–1428.
Augello C, Gianelli U, Savi F et al. MicroRNA as potential biomarker in HCV-associated diffuse large B-cell lymphoma. J Clin Pathol 2014;67:697–701.
Asmar F, Hother C, Kulosman G et al. Diffuse large B-cell lymphoma with combined TP53 mutation and MIR34A methylation: another "double hit" lymphoma with very poor outcome? Oncotarget 2014;5:1912–1925.
Jones K, Nourse JP, Keane C et al. Plasma microRNA are disease response biomarkers in classical Hodgkin lymphoma. Clin Cancer Res 2014;20:253–264.
Takei Y, Ohnishi N, Kisaka M et al. Determination of abnormally expressed microRNAs in bone marrow smears from patients with follicular lymphomas. Springerplus 2014;3:288.
Song G, Gu L, Li J et al. Serum microRNA expression profiling predict response to R-CHOP treatment in diffuse large B cell lymphoma patients. Ann Hematol 2014;93:1735–1743.
Cheng G . Circulating miRNAs: roles in cancer diagnosis, prognosis and therapy. Adv Drug Deliv Rev 2015;81:75–93.
Mehrotra M, Medeiros LJ, Luthra R et al. Identification of putative pathogenic microRNA and its downstream targets in anaplastic lymphoma kinase-negative anaplastic large cell lymphoma. Hum Pathol 2014;45:1995–2005.
Liu C, Iqbal J, Teruya-Feldstein J et al. MicroRNA expression profiling identifies molecular signatures associated with anaplastic large cell lymphoma. Blood 2013;122:2083–2092.
Sotomayor EM, Young KH, Younes A . Clinical roundtable monograph: CD30 in lymphoma: its role in biology, diagnostic testing, and targeted therapy. Clin Adv Hematol Oncol 2014;12:1–22.
Migliazza A, Martinotti S, Chen WY et al. Frequent somatic hypermutation of the 5' noncoding region of the BCL6 gene in B-cell lymphoma. Proc Natl Acad Sci USA 1995;92:12520–12524.
Seegmiller AC, Garcia R, Huang R et al. Simple karyotype and bcl-6 expression predict a diagnosis of Burkitt lymphoma and better survival in IG-MYC rearranged high-grade B-cell lymphomas. Mod Pathol 2010;23:909–920.
Hu S, Xu-Monette ZY, Tzankov A et al. MYC/BCL2 protein coexpression contributes to the inferior survival of activated B-cell subtype of diffuse large B-cell lymphoma and demonstrates high-risk gene expression signatures: a report from The International DLBCL Rituximab-CHOP Consortium Program. Blood 2013;121:4021–4031.
Aukema SM, Siebert R, Schuuring E et al. Double-hit B-cell lymphomas. Blood 2011;117:2319–2331.
Vela-Chavez T, Adam P, Kremer M et al. Cyclin D1 positive diffuse large B-cell lymphoma is a post-germinal center-type lymphoma without alterations in the CCND1 gene locus. Leuk lymphoma 2011;52:458–466.
Salaverria I, Royo C, Carvajal-Cuenca A et al. CCND2 rearrangements are the most frequent genetic events in cyclin D1(-) mantle cell lymphoma. Blood 2013;121:1394–1402.
Rosenwald A, Wright G, Wiestner A et al. The proliferation gene expression signature is a quantitative integrator of oncogenic events that predicts survival in mantle cell lymphoma. Cancer Cell 2003;3:185–197.
Mozos A, Royo C, Hartmann E et al. SOX11 expression is highly specific for mantle cell lymphoma and identifies the cyclin D1-negative subtype. Haematologica 2009;94:1555–1562.
Kuo PY, Leshchenko VV, Fazzari MJ et al. High-resolution chromatin immunoprecipitation (ChIP) sequencing reveals novel binding targets and prognostic role for SOX11 in mantle cell lymphoma. Oncogene 2015;34:1231–1240.
Ok CY, Xu-Monette ZY, Tzankov A et al. Prevalence and clinical implications of cyclin D1 expression in diffuse large B-cell lymphoma (DLBCL) treated with immunochemotherapy: a report from the International DLBCL Rituximab-CHOP Consortium Program. Cancer 2014;120:1818–1829.
Xu-Monette ZY, Moller MB, Tzankov A et al. MDM2 phenotypic and genotypic profiling, respective to TP53 genetic status, in diffuse large B-cell lymphoma patients treated with rituximab-CHOP immunochemotherapy: a report from the International DLBCL Rituximab-CHOP Consortium Program. Blood 2013;122:2630–2640.
Zamo A, Malpeli G, Scarpa A et al. Expression of TP73L is a helpful diagnostic marker of primary mediastinal large B-cell lymphomas. Mod Pathol 2005;18:1448–1453.
Lilja L, Haapasaari KM, Bloigu R et al. Increased expression of CIP2A in aggressive subtypes of B-cell lymphoma. Histopathology 2013;63:438–439.
Alizadeh AA, Eisen MB, Davis RE et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature 2000;403:503–511.
Choi WWL, Weisenburger DD, Greiner TC et al. A new immunostain algorithm classifies diffuse large B-cell lymphoma into molecular subtypes with high accuracy. Clin Cancer Res 2009;15:5494–5502.
Hans CP, Weisenburger DD, Greiner TC et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood 2004;103:275–282.
Visco C, Li Y, Xu-Monette ZY et al. Comprehensive gene expression profiling and immunohistochemical studies support application of immunophenotypic algorithm for molecular subtype classification in diffuse large B-cell lymphoma: a report from the International DLBCL Rituximab-CHOP Consortium Program Study. Leukemia 2012;26:2103–2113.
Meyer PN, Fu K, Greiner TC et al. Immunohistochemical methods for predicting cell of origin and survival in patients with diffuse large B-cell lymphoma treated with rituximab. J Clin Oncol 2011;29:200–207.
Chang CC, McClintock S, Cleveland RP et al. Immunohistochemical expression patterns of germinal center and activation B-cell markers correlate with prognosis in diffuse large B-cell lymphoma. Am J Surg Pathol 2004;28:464–470.
Banham AH, Connors JM, Brown PJ et al. Expression of the FOXP1 transcription factor is strongly associated with inferior survival in patients with diffuse large B-cell lymphoma. Clin Cancer Res 2005;11:1065–1072.
Nyman H, Jerkeman M, Karjalainen-Lindsberg ML et al. Bcl-2 but not FOXP1, is an adverse risk factor in immunochemotherapy-treated non-germinal center diffuse large B-cell lymphomas. Eur J Haematol 2009;82:364–372.
Filipits M, Jaeger U, Pohl G et al. Cyclin D3 is a predictive and prognostic factor in diffuse large B-cell lymphoma. Clin Cancer Res 2002;8:729–733.
Hans CP, Weisenburger DD, Greiner TC et al. Expression of PKC-beta or cyclin D2 predicts for inferior survival in diffuse large B-cell lymphoma. Mod Pathol 2005;18:1377–1384.
Adida C, Haioun C, Gaulard P et al. Prognostic significance of survivin expression in diffuse large B-cell lymphomas. Blood 2000;96:1921–1925.
Muris JJF, Cillessen SAGM, Vos W et al. Immunohistochemical profiling of caspase signaling pathways predicts clinical response to chemotherapy in primary nodal diffuse large B-cell lymphomas. Blood 2005;105:2916–2923.
Liu ZY, Xu-Monette ZY, Cao X et al. Prognostic and biological significance of survivin expression in patients with diffuse large B-cell lymphoma treated with rituximab-CHOP therapy. Mod Pathol 2015;28:1297–1314.
Jost PJ, Ruland J . Aberrant NF-kappa B signaling in lymphoma: mechanisms, consequences, and therapeutic implications. Blood 2007;109:2700–2707.
Gasparini C, Celeghini C, Monasta L, Zauli G . NF-kappa B pathways in hematological malignancies. Cell Mol Life Sci 2014;71:2083–2102.
Bavi P, Uddin S, Bu R et al. The biological and clinical impact of inhibition of NF-kappa B-initiated apoptosis in diffuse large B cell lymphoma (DLBCL). J Pathol 2011;224:355–366.
Ok CY, Xu-Monette ZY, Li L et al. Evaluation of NF-kappa B subunit expression and signaling pathway activation demonstrates that p52 expression confers better outcome in germinal center B-cell-like diffuse large B-cell lymphoma in association with CD30 and BCL2 functions. Mod Pathol 2015;28:1202–1213.
Odqvist L, Montes-Moreno S, Sanchez-Pacheco RE et al. NF kappa B expression is a feature of both activated B-cell-like and germinal center B-cell-like subtypes of diffuse large B-cell lymphoma. Mod Pathol 2014;27:1331–1337.
Li L, Xu-Monette ZY, Ok CY et al. Prognostic impact of c-Rel nuclear expression and REL amplification and crosstalk between c-Rel and the p53 pathway in diffuse large B-cell lymphoma. Oncotarget 2015;6:23157–23180.
Niemann CU, Wiestner A . B-cell receptor signaling as a driver of lymphoma development and evolution. Semin Cancer Biol 2013;23:410–421.
Wiestner A . Targeting B-Cell receptor signaling for anticancer therapy: the Bruton's tyrosine kinase inhibitor ibrutinib induces impressive responses in B-cell malignancies. J Clin Oncol 2013;31:128–130.
Nicolae A, Pittaluga S, Venkataraman G et al. Peripheral T-cell lymphomas of follicular T-helper cell derivation with Hodgkin/Reed-Sternberg cells of B-cell lineage: both EBV-positive and EBV-negative variants exist. Am J Surg Pathol 2013;37:816–826.
Quintanilla-Martinez L, Fend F, Moguel LR et al. Peripheral T-cell lymphoma with Reed-Sternberg-like cells of B-cell phenotype and genotype associated with Epstein-Barr virus infection. Am J Surg Pathol 1999;23:1233–1240.
Jaffe ES, Nicolae A, Pittaluga S . Peripheral T-cell and NK-cell lymphomas in the WHO classification: pearls and pitfalls. Mod Pathol 2013;26:S71–S87.
Roncador G, Garcia Verdes-Montenegro JF, Tedoldi S et al. Expression of two markers of germinal center T cells (SAP and PD-1) in angioimmunoblastic T-cell lymphoma. Haematologica 2007;92:1059–1066.
Marafioti T, Paterson JC, Ballabio E et al. The inducible T-cell co-stimulator molecule is expressed on subsets of T cells and is a new marker of lymphomas of T follicular helper cell-derivation. Haematologica 2010;95:432–439.
Dorfman DM, Shahsafaei A . CD200 (OX-2 membrane glycoprotein) is expressed by follicular T helper cells and in angioimmunoblastic T-cell lymphoma. Am J Surg Pathol 2011;35:76–83.
Bisig B, Thielen C, Herens C et al. c-Maf expression in angioimmunoblastic T-cell lymphoma reflects follicular helper T-cell derivation rather than oncogenesis. Histopathology 2012;60:371–376.
Saffer H, Wahed A, Rassidakis GZ et al. Clusterin expression in malignant lymphomas: a survey of 266 cases. Mod Pathol 2002;15:1221–1226.
Bisig B, Gaulard P, de Leval L . New biomarkers in T-cell lymphomas. Best Pract Res Clin Haematol 2012;25:13–28.
Shaulian E . AP-1-The Jun proteins: oncogenes or tumor suppressors in disguise? Cell Signal 2010;22:894–899.
Mathas S, Hinz M, Anagnostopoulos I et al. Aberrantly expressed c-Jun and JunB are a hallmark of Hodgkin lymphoma cells, stimulate proliferation and synergize with NF-kappa B. EMBO J 2002;21:4104–4113.
Rassidakis GZ, Thomaides A, Atwell C et al. JunB expression is a common feature of CD30+lymphomas and lymphomatoid papulosis. Mod Pathol 2005;18:1365–1370.
Rodig SJ, Ouyang J, Juszczynski P et al. AP1-dependent galectin-1 expression delineates classical hodgkin and anaplastic large cell lymphomas from other lymphoid malignancies with shared molecular features. Clin Cancer Res 2008;14:3338–3344.
Ouyang J, Plutschow A, von Strandmann EP et al. Galectin-1 serum levels reflect tumor burden and adverse clinical features in classical Hodgkin lymphoma. Blood 2013;121:3431–3433.
Giordano M, Croci DO, Rabinovich GA . Galectins in hematological malignancies. Curr Opin Hematol 2013;20:327–335.
de Jong D, Fest T . The microenvironment in follicular lymphoma. Best Pract Res Clin Haematol 2011;24:135–146.
Alavaikko MJ, Blanco G, Aine R et al. Follicular dendritic cells have prognostic relevance in Hodgkins-disease. Am J Clin Pathol 1994;101:761–767.
Baur AS, Meuge-Moraw C, Michel G et al. Prognostic value of follicular dendritic cells in nodular sclerosing Hodgkin's disease. Histopathology 1998;32:512–520.
ten Berge RL, Oudejans JJ, Dukers DF et al. Percentage of activated cytotoxic T-lymphocytes in anaplastic large cell lymphoma and Hodgkin's disease: an independent biological prognostic marker. Leukemia 2001;15:458–464.
Oudejans JJ, Jiwa NM, Kummer JA et al. Activated cytotoxic T cells as prognostic marker in Hodgkin's disease. Blood 1997;89:1376–1382.
Molin D, Edstrom A, Glimelius I et al. Mast cell infiltration correlates with poor prognosis in Hodgkin's lymphoma. Br J Haematol 2002;119:122–124.
Hedstrom G, Berglund M, Molin D et al. Mast cell infiltration is a favourable prognostic factor in diffuse large B-cell lymphoma. Br J Haematol 2007;138:68–71.
Qian BZ, Pollard JW . Macrophage diversity enhances tumor progression and metastasis. Cell 2010;141:39–51.
Tan KL, Scott DW, Hong FX et al. Tumor-associated macrophages predict inferior outcomes in classic Hodgkin lymphoma: a correlative study from the E2496 Intergroup trial. Blood 2012;120:3280–3287.
Sanchez-Espiridion B, Martin-Moreno AM, Montalban C et al. Immunohistochemical markers for tumor associated macrophages and survival in advanced classical Hodgkin's lymphoma. Haematologica 2012;97:1080–1084.
Riihijarvi S, Fiskvik I, Taskinen M et al. Prognostic influence of macrophages in patients with diffuse large B-cell lymphoma: a correlative study from a Nordic phase II trial. Haematologica 2015;100:238–245.
Barros MH, Hassan R, Niedobitek G . Tumor-associated macrophages in pediatric classical Hodgkin lymphoma: association with Epstein-Barr virus, lymphocyte subsets, and prognostic impact. Clin Cancer Res 2012;18:3762–3771.
Carreras J, Lopez-Guillermo A, Fox BC et al. High numbers of tumor-infiltrating FOXP3-positive regulatory T cells are associated with improved overall survival in follicular lymphoma. Blood 2006;108:2957–2964.
Alvaro T, Lejeune M, Salvado MT et al. Outcome in Hodgkin's lymphoma can be predicted from the presence of accompanying cytotoxic and regulatory T cells. Clin Cancer Res 2005;11:1467–1473.
Kim WY, Jeon YK, Kim TM et al. Increased quantity of tumor-infiltrating FOXP3-positive regulatory T cells is an independent predictor for improved clinical outcome in extranodal NK/T-cell lymphoma. Ann Oncol 2009;20:1688–1696.
Hasselblom S, Sigurdadottir M, Hansson U et al. The number of tumour-infiltrating TIA-1+ cytotoxic T cells but not FOXP3+ regulatory T cells predicts outcome in diffuse large B-cell lymphoma. Br J Haematol 2007;137:364–373.
Lee NR, Song EK, Jang KY et al. Prognostic impact of tumor infiltrating FOXP3 positive regulatory T cells in diffuse large B-cell lymphoma at diagnosis. Leuk Lymphoma 2008;49:247–256.
Muenst S, Hoeller S, Dirnhofer S et al. Increased programmed death-1+tumor-infiltrating lymphocytes in classical Hodgkin lymphoma substantiate reduced overall survival. Hum Pathol 2009;40:1715–1722.
Nam-Cha SH, Roncador G, Sanchez-Verde L et al. PD-1, a follicular T-cell marker useful for recognizing nodular lymphocyte-predominant Hodgkin lymphoma. Am J Surgl Pathol 2008;32:1252–1257.
Carreras J, Lopez-Guillermo A, Roncador G et al. High numbers of tumor-infiltrating Programmed Cell Death 1-positive regulatory lymphocytes are associated with improved overall survival in follicular lymphoma. J Clin Oncol 2009;27:1470–1476.
Wahlin BE, Aggarwal M, Montes-Moreno S et al. A unifying microenvironment model in follicular lymphoma: outcome is predicted by Programmed Death-1-Positive, regulatory, cytotoxic, and helper T cells and macrophages. Clin Cancer Res 2010;16:637–650.
Rossille D, Gressier M, Damotte D et al. High level of soluble programmed cell death ligand 1 in blood impacts overall survival in aggressive diffuse large B-Cell lymphoma: results from a French multicenter clinical trial. Leukemia 2014;28:2367–2375.
Kiyasu J, Miyoshi H, Hirata A et al. Expression of programmed cell death ligand 1 is associated with poor overall survival in patients with diffuse large B-cell lymphoma. Blood 2015;126:2193–2201.
Xia Y, Medeiros LJ, Young KH . Signaling pathway and dysregulation of PD1 and its ligands in lymphoid malignancies. Biochim Biophys Acta 2015;1865:58–71.
Ansell SM, Lesokhin AM, Borrello I et al. PD-1 blockade with nivolumab in relapsed or refractory Hodgkin's lymphoma. N Engl J Med 2015;372:311–319.
Challa-Malladi M, Lieu YK, Califano O et al. Combined genetic inactivation of beta2-Microglobulin and CD58 reveals frequent escape from immune recognition in diffuse large B cell lymphoma. Cancer cell 2011;20:728–740.
Pasqualucci L, Trifonov V, Fabbri G et al. Analysis of the coding genome of diffuse large B-cell lymphoma. Nat Genet 2011;43:830–837.
Cheung KJ, Johnson NA, Affleck JG et al. Acquired TNFRSF14 mutations in follicular lymphoma are associated with worse prognosis. Cancer Res 2010;70:9166–9174.
Diepstra A, van Imhoff GW, Schaapveld M et al. Latent Epstein-Barr virus infection of tumor cells in classical Hodgkin's lymphoma predicts adverse outcome in older adult patients. J Clin Oncol 2009;27:3815–3821.
Jarrett RF, Stark GL, White J et al. Impact of tumor Epstein-Barr virus status on presenting features and outcome in age-defined subgroups of patients with classic Hodgkin lymphoma: a population-based study. Blood 2005;106:2444–2451.
Meyer RM . EBV DNA: a Hodgkin lymphoma biomarker? Blood 2013;121:3541–3542.
Montes-Moreno S, Odqvist L, Diaz-Perez JA et al. EBV-positive diffuse large B-cell lymphoma of the elderly is an aggressive post-germinal center B-cell neoplasm characterized by prominent nuclear factor-kB activation. Mod Pathol 2012;25:968–982.
Nicolae A, Pittaluga S, Abdullah S et al. EBV-positive large B-cell lymphomas in young patients: a nodal lymphoma with evidence for a tolerogenic immune environment. Blood 2015;126:863–872.
Deng L, Song Y, Young KH et al. Hepatitis B virus-associated diffuse large B-cell lymphoma: unique clinical features, poor outcome, and hepatitis B surface antigen-driven origin. Oncotarget 2015;6:25061–25073.
Peveling-Oberhag J, Arcaini L, Hansmann ML et al. Hepatitis C-associated B-cell non-Hodgkin lymphomas. Epidemiology, molecular signature and clinical management. J Hepatol 2013;59:169–177.
Christenson ES, Teply B, Agrawal V et al. Human herpesvirus 8-related primary effusion lymphoma after liver transplantation. Am J Transplant 2015;15:2762–2766.
Sanchez-Aguilera A, Montalban C, De la Cueva P et al. Tumor microenvironment and mitotic checkpoint are key factors in the outcome of classic Hodgkin lymphoma. Blood 2006;108:662–668.
Sanchez-Espiridion B, Sanchez-Aguilera A, Montalban C et al. A TaqMan low-density array to predict outcome in advanced Hodgkin's lymphoma using paraffin-embedded samples. Clin Cancer Res 2009;15:1367–1375.
Steidl C, Lee T, Shah SP et al. Tumor-associated macrophages and survival in classic Hodgkin's lymphoma. N Engl J Med 2010;362:875–885.
Sanchez-Espiridion B, Montalban C, Lopez A et al. A molecular risk score based on 4 functional pathways for advanced classical Hodgkin lymphoma. Blood 2010;116:E12–E17.
Lenz G, Wright G, Dave SS et al. Stromal gene signatures in large-B-cell lymphomas. N Engl J Med 2008;359:2313–2323.
Xia Y, Medeiros LJ, Young KH . Immune checkpoint blockade: Releasing the brake towards hematological malignancies. Blood Rev 2015 [Epub ahead of print].
Young KH, Medeiros LJ, Chan WC . Diffuse large B-cell lymphoma. In: Orazi A, Weiss LM, Foucar K, Knowles DM, eds. Neoplastic Hematopathology. Lippincott Willaims & Wilkins: Philadelphia, PA, USA, 2014, pp 502–565.
Acknowledgements
This study was supported by the National Cancer Institute/National Institutes of Health (R01CA138688 and 1RC1CA146299 to KHY). RFS is a recipient of pathology scholarship award. KHY is supported by The University of Texas MD Anderson Cancer Center Lymphoma Moonshot Program, Institutional Research and Development Fund, an Institutional Research Grant Award, an MD Anderson Cancer Center Lymphoma Specialized Programs on Research Excellence (SPORE) Research Development Program Award, an MD Anderson Cancer Center Myeloma SPORE Research Development Program Award, a Gundersen Lutheran Medical Foundation Award, the University Cancer Foundation via the Sister institution network Fund at The University of Texas MD Anderson Cancer Center, and partially supported by the National Cancer Institute/National Institutes of Health (P50CA136411 and P50CA142509), and by the MD Anderson Cancer Center Support Grant CA016672.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
KHY receives research support from Roche Molecular System, Gilead Sciences Pharmaceutical, Seattle Genetics, Dai Sanyo Pharmaceutical, Adaptive Biotechnology, Incyte Pharmaceutical, and HTG Molecular Diagnostics.
Rights and permissions
About this article

Cite this article
Sun, R., Medeiros, L. & Young, K. Diagnostic and predictive biomarkers for lymphoma diagnosis and treatment in the era of precision medicine. Mod Pathol 29, 1118–1142 (2016). https://doi.org/10.1038/modpathol.2016.92
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/modpathol.2016.92
This article is cited by
-
Molecular complexity of diffuse large B-cell lymphoma: a molecular perspective and therapeutic implications
Journal of Applied Genetics (2024)
-
An Investigation into Cell-Free DNA in Different Common Cancers
Molecular Biotechnology (2023)
