
Abstract
Objective:
To assess the risk of neonatal mortality and morbidity in vertex–vertex second twins according to mode of delivery and birth weight.
Study design:
Data from a historical cohort study based on a twin registry in the US (1995–1997) were used. Multivariate logistic regression was used to control for maternal age, race, marital status, cigarette smoking during pregnancy, parity, medical complications, gestational age, and other confounders.
Results:
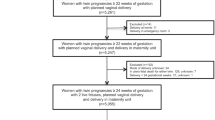
A total of 86 041 vertex–vertex second twins were classified into two groups: second twins delivered by cesarean section after cesarean delivery of first twin (C–C) (43.0%), second twins whose co-twins delivered vaginally (V–X) (57.0%). In infants of birth weight ⩾2500 g group, the risks of noncongenital anomaly-related death (adjusted odds ratio (aOR): 4.64, 95% confidence interval (95% CI): 1.90, 13.92), low Apgar score (aOR: 2.39, 95% CI: 1.43, 4.14), and ventilation use (aOR: 1.31, 95% CI: 1.18, 1.47) were higher in the V–X group compared with the C–C group. No asphyxia-related neonatal deaths occurred in C–C group, whereas the incidence of this death was 0.04% in the V–X group.
Conclusion:
The risks of neonatal mortality and morbidity are increased in vertex–vertex second twins with birth weight ⩾2500 g whose co-twins delivered vaginally compared with second twins delivered by cesarean section after cesarean delivery of first twin.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Blondel B, Kaminski M . Trends in the occurrence, determinants, and consequences of multiple births. Semin Perinatol 2002; 26: 239–249.
Power WP, Wampler NS . Further defining the risks confronting twins. Am J Obstet Gynecol 1996; 175: 1522–1528.
Rydhstroem H . Should all twins be delivered by caesarean section? A preliminary report. Twin Res 2001; 4: 156–158.
Smith GC, Pell JP, Dobbie R . Birth order, gestational age, and risk of delivery related perinatal death in twins: retrospective cohort study. BMJ 2002; 325: 1004–1009.
Wen SW, Fung Kee Fung K, Oppenheimer L, Demissie K, Yang Q, Walker M . Neonatal mortality in second twin according to cause of death, gestational age, and mode of delivery. Am J Obstet Gynocol 2004; 191: 778–783.
Wen SW, Fung Kee Fung K, Oppenheimer L, Demissie K, Yang Q, Walker M . Neonatal morbidity in second twin according to gestational age at birth and mode of delivery. Am J Obstet Gynocol 2004; 191: 773–777.
Wen SW, Fung Kee Fung K, Oppenheimer L, Demissie K, Yang Q, Walker M . Occurrence and clinical predictors of emergent cesarean delivery for second twin. Obstet Gynecol 2004; 103: 413–419.
Chervenak FA, Johnson RE, Berkowitz RL, Hobbins JC . Intrapartum external version of the second twin. Obstet Gynecol 1983; 62: 160–165.
Crawford JS . A prospective study of 200 consecutive twin deliveries. Anaesthesia 1987; 42: 33–43.
Divon MY, Marin MJ, Pollack RN, Katz NT, Henderson C, Aboulafia Y et al. Twin gestation: fetal presentation as a function of gestational age. Am J Obstet Gynecol 1993; 168: 1500–1502.
Kelsick F, Minkoff H . Management of the breech second twin. Am J Obstet Gynecol 1982; 144: 783–786.
Thompson SA, Lyons TJ, Makowski EL . Outcomes of twin gestation at the University of Colorado Health Science centre. J Reproduct Med 1987; 32: 328–329.
Laros RK, Dattel BJ . Management of twin pregnancy; the vaginal route is still safe. Am J Obstet Gynecol 1998; 158: 1330–1338.
Piekarski P, Czajkowski K, Maj K, Milewczyk P . Neonatal outcome depending on the mode of delivery and fetal presentation in twin gestation (abstract). Ginekol Pol 1997; 68: 187–192.
Boggess KA, Chisholm CA . Delivery of the nonvertex second twin: a review of the literature. Obstet Gynecol Surv 1997; 52: 728–735.
Blickstein I . Cesarean section for all twins? J Perinat Med 2000; 28: 169–174.
Anonymous. Special problems of multiple gestations. Int J Gynaecol Obstet 1999; 64: 323–333.
Barrett J, Bocking A . The SOGC consensus statement on management of twin pregnancies (Part I). J SOGC 2000; 91: 519–532.
National Center for Health Statistics. 1995–1997 Matched Multiple Birth Data Set. NCHS CD-ROM Series 21, No. 12. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention: Hyattsville, Maryland; 2000.
Cole S, Hartford RB, Bersjo P, McCarthy B . International collaborative effort (ICE) in birth weight, plurality, perinatal and infant mortality. Acta Obstet Gynecol Scand 1989; 68: 113–117.
Yang Q, Wen SW, Chen Y, Krewski D, Fung Kee Fung K, Walker M . Neonatal mortality and morbidity in vertex–nonvertex second twins according to mode of delivery and birth weight. Am J Obstet Gynecol 2005; 192: 840–847.
Sullivan CA, Harkins D, Seago DP, Roberts WE, Morrison JC . Cesarean delivery for the second twin in the vertex–vertex presentation: operative indications and predictability. South Med J 1998; 91: 155–158.
Huston P, Naylor CD . Health services research: reporting on studies using secondary data sources. Can Med Assoc J 1996; 155: 1697–1702.
Millimet D . What is the difference between ‘endogeneity’ and ‘sample selection bias’? Frequently Asked Questions (FAQ) for STATA, http://www.stata.com/support/faqs/stat/bias.html.
Wen SW, Joseph KS, Kramer MS, Demissie K, Oppenheimer L, Liston R, et al., For the Fetal and Infant Mortality Study Group. Canadian Perinatal Surveillance System. Recent secular trends in fetal and infant outcomes among post-term pregnancies. Chron Dis Can 2001; 22: 1–5.
Greig P, Veille J, Morgan T, Henderson L . The effect of presentation and mode of delivery on neonatal outcome in the second twin. Am J Obstet Gynecol 1992; 167: 901–906.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yang, Q., Wen, S., Chen, Y. et al. Neonatal mortality and morbidity in vertex–vertex second twins according to mode of delivery and birth weight. J Perinatol 26, 3–10 (2006). https://doi.org/10.1038/sj.jp.7211408
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jp.7211408
Keywords
This article is cited by
-
Birth management and fetal outcome in multiple gestation: analysis of 1.444 births
Archives of Gynecology and Obstetrics (2018)
-
Perinatal Outcome of the Second Twin at a Tertiary Care Center in India
The Journal of Obstetrics and Gynecology of India (2016)
-
Elective cesarean delivery: when is it justified?
Journal of Perinatology (2006)
