
Abstract
OBJECTIVE: To investigate pulse oximetry in neonates who require arterial access as represented by the clinical data recorded to manage their care.
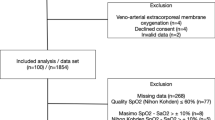
STUDY DESIGN: Analysis of simultaneous SpO2 and SaO2 from: 7-year historical NICU data (N=31,905); 4-month prospective NICU data (N=566); verification data using two hemoximeters (N=52); and NICU data from two collaborating centers (N=95 and 168). The bias function (SpO2−SaO2) was regressed against the measured “gold” standard, SaO2.
RESULTS: A significant negative correlation was found for each of the data sets between the bias function and SaO2. This bias was similar for devices from several manufacturers (Datex-Ohmeda, Masimo, Nellcor, and Spacelabs). Maximum operational performance occurred with peaks between 92 and 97% SaO2, but declined markedly above and below this narrow range. In all, 71 to 95% of patients exhibited data with significant bias.
CONCLUSION: These operational data suggest that with the methodology and devices currently in use, SpO2 values in most all neonates who require arterial lines inaccurately correlate with measured arterial saturation.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others

References
Hay Jr WW, Brockway JM, Eyzaguirre M . Neonatal pulse oximetry: accuracy and reliability. Pediatrics 1989;83:717–722.
Sardesai S, Durand M, McEvoy C, Johnson C, Maarek JM . Pulse oximetry in newborn infants with birth weights of 620 to 4285 grams receiving dopamine and dobutamine. J Perinatol 1996;16:31–34.
Rajadurai VS, Walker AM, Yu VY, Oates A . Effect of fetal haemoglobin on the accuracy of pulse oximetry in preterm infants. J Paediatr Child Health 1992;28:43–46.
Zubrow AB, Henderson GW, Imaizumi SO, Pleasure JR . Pulse oximetry in sick premature infants and the effects of phototherapy and radiant warmers on the oxygen saturation readout. Am J Perinatol 1990;7:75–78.
Walsh MC, Noble LM, Carlo WA, Martin RJ . Relationship of pulse oximetry to arterial oxygen tension in infants. Crit Care Med 1987;15:1102–1105.
Thilo EH, Andersen D, Wasserstein ML, Schmidt J, Luckey D . Saturation by pulse oximetry: comparison of the results obtained by instruments of different brands. J Pediatr 1993;122:620–626.
Brockway J, Hay Jr WW . Prediction of arterial partial pressure of oxygen with pulse oxygen saturation measurements. J Pediatr 1998;133:63–66.
Gupta R, Yoxall CW, Subhedar N, Shaw NJ . Individualised pulse oximetry limits in neonatal intensive care. Arch Dis Child Fetal Neonatal Ed 1999;81:F194–F196.
Severinghaus JW, Naifeh KH, Koh SO . Errors in 14 pulse oximeters during profound hypoxia. J Clin Monit 1989;5:72–81.
Fanconi S . Reliability of pulse oximetry in hypoxic infants. J Pediatr 1988;112:424–427.
Praud JP, Carofilis A, Bridey F, Lacaille F, Dehan M, Gaultier CL . Accuracy of two wavelength pulse oximetry in neonates and infants. Pediatr Pulmonol 1989;6:180–182.
Hay Jr WW, Rodden DJ, Collins SM, Melara DL, Hale KA, Fashaw LM . Reliability of conventional and new pulse oximetry in neonatal patients. J Perinatol 2002;22:360–366.
Lebecque P, Shango P, Stijns M, Vliers A, Coates AL . Pulse oximetry versus measured arterial oxygen saturation: a comparison of the Nellcor N100 and the Biox III. Pediatr Pulmonol 1991;10:132–135.
Schmitt HJ, Schuetz WH, Proeschel PA, Jaklin C . Accuracy of pulse oximetry in children with cyanotic congenital heart disease. J Cardiothorac Vasc Anesth 1993;7:61–65.
Boxer RA, Gottesfeld I, Singh S, LaCorte MA, Parnell Jr VA, Walker P . Noninvasive pulse oximetry in children with cyanotic congenital heart disease. Crit Care Med 1987;15:1062–1064.
Carter BG, Carlin JB, Tibballs J, Mead H, Hochmann M, Osborne A . Accuracy of two pulse oximeters at low arterial hemoglobin–oxygen saturation. Crit Care Med 1998;26:1128–1133.
Gehring H, Hornberger C, Matz H, Konecny E, Schmucker P . The effects of motion artefact and low perfusion on the performance of a new generation of pulse oximeters in volunteers undergoing hypoxemia. Respir Care 2002;47:48–60.
Parath M, Sinha P, Dudenhoused JW, Lurrkus AK . Systematic instrumental errors between oxygen saturation analysers in fetal blood during deep hypoxemia. Clin Chim Acta 2001;307:151–157.
Mannheimer PD . Design and validation of pulse oximetry for low saturation. Anesth Analg 2002;94(Suppl 1):S21–S25.
Mannheimer PD, Casciani JR, Fein ME, Nierlich SL . Wavelength selection for low-saturation pulse oximetry. IEEE Trans Biomed Eng 1997;44:148–158.
Aoyagi T, Miyasaka K . The theory and applications of pulse spectrophotometry. Anesth Analg 2002;94(Suppl 1):S93–S95.
Author information
Authors and Affiliations
Additional information
These data were presented in part as a Late Breaker Abstract at the Pediatric Academic Societies mdash; Society for Pediatric Research Meeting, May 2002, Baltimore, MD, USA. An FDA Medical Device Report (#1024269) was filed with Med Watch on March 5, 2002.
Rights and permissions
About this article
Cite this article
Gerstmann, D., Berg, R., Haskell, R. et al. Operational Evaluation of Pulse Oximetry in NICU Patients with Arterial Access. J Perinatol 23, 378–383 (2003). https://doi.org/10.1038/sj.jp.7210944
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jp.7210944
This article is cited by
-
Racial discrepancy in pulse oximeter accuracy in preterm infants
Journal of Perinatology (2022)
-
Betreuung des gesunden Neugeborenen in Kreißsaal und Kinderzimmer
Monatsschrift Kinderheilkunde (2018)
-
Pulsoxymetriescreening bei Neugeborenen auf kritische angeborene Herzfehler
Monatsschrift Kinderheilkunde (2014)
-
Moving from experience to evidence: changes in US Neonatal Resuscitation Program based on International Liaison Committee on Resuscitation Review
Journal of Perinatology (2008)
-
The contribution of pulse oximetry to the early detection of congenital heart disease in newborns
European Journal of Pediatrics (2006)
