
Abstract
OBJECTIVE: To estimate the extent that prenatal care (PNC) retains its protective influence against prematurity, low birth weight (LBW), and small for gestational age (SGA) status in infants exposed to illicit drug use (IDU) in pregnancy.
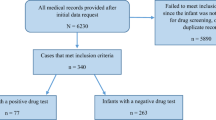
STUDY DESIGN: This was a prospective cohort analysis including 6673 women residents of the District of Columbia (Washington, DC, USA) delivering at four city hospitals. Women were screened in the immediate postpartum period. Levels of PNC were established according to American College of Obstetrics and Gynecology guidelines and the Kotelchuck index. PNC and IDU were compared between subgroups. Adjusted relative risks for prematurity, LBW and SGA, controlling for maternal and gestational ages, were calculated in different groups according to IDU and level of PNC.
RESULTS: IDU was identified in 13% of mothers screened. PNC was classified as none (6%), inadequate (10%), intermediate (20%), and adequate (64%). The highest risk for prematurity, LBW, or SGA occurred in infants born to mothers with no PNC and positive IDU in pregnancy (prematurity OR=12.05, 95% CI: 8.99 to 16.16; LBW OR=14.76, 95% CI: 11.03 to 19.75; SGA OR=9.20, 95% CI: 5.32 to 15.92). As PNC levels increased, significant reductions in risk for prematurity and LBW (not for SGA) in IDU-exposed infants were observed. Risk for SGA in IDU-exposed infants reduced significantly when PNC was introduced.
CONCLUSIONS: In infants exposed to IDU, a reduction in risk for prematurity, LBW, and SGA, was consistently demonstrated with improved levels of PNC. In high-risk populations, health care should seek to reach mothers early, especially those identified at risk for IDU, and deliver PNC to them effectively.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Chasnoff IJ . Cocaine and Pregnancy: Clinical and methodological issues. Clin Perinatol 1991;18: 113–123.
Robins LN, Mills JL, Krulewitch C, et al. Effects of in utero exposure to street drugs. Am J Public Health 1993;83:3–32.
American Academy of Pediatrics, American College of Obstetricians and Gynecologists. Guidelines for Perinatal Care. 3rd ed. Elk Grove, IL: American Academy of Pediatrics; 1992. p. 296.
Kotelchuck M . The adequacy of prenatal care utilization index: its US distribution and association with low birthweight. Am J Public Health 1994;84:1486–1489.
Fink A, Yano EM, Goya D . Prenatal programs: what the literature reveals. Obstet Gynecol 1992;80:867–872.
Broekhuizen FF, Utrie J, Van Mullem CV . Drug use or inadequate prenatal care? Adverse pregnancy outcome in an urban setting. Am J Obstet Gynecol 1992;166:1747–1756.
Funkhouser AW, Butz AM, Feng TI, et al. Prenatal care and drug use in pregnant women. Drug Alcohol Dependence 1993;33:1–9.
ACOG. Standards for Obstetric-Gynecologic Services. 6th ed. Washington, DC: American College of Obstetricians and Gynecologists; 1985.
Kotelchuck M . An evaluation of the Kessner Adequacy of Prenatal Care Index and a proposed Adequacy of Prenatal Care Utilization Index. Am J Public Health 1994;84:1414–1420.
Mehta C, Patel N . StatXact 3 for Windows; Statistical Software for Exact Nonparametric Inference. Cambridge, MA: Cytel Software Corporation; 1996.
State Center for Health Statistics — Department of Health. Briefing paper on the 1996 infant mortality rate for the District of Columbia. Washington, D.C: State Center for Health Statistics — Department of Health; 1996.
Guyer B, Strobino DM, Ventura SJ, et al. Annual summary of vital statistics — 1996. Pediatrics 1997;100:905–918.
Phelps DL, Brown DR, Tung B, et al. Twenty-eight day survival rates of 6676 neonates with birth weights of 1250 grams or less. Pediatrics 1991;87:7–17.
Sumits T, Bennet R, Gould J . Maternal risks for very low birth weight infant mortality. Pediatrics 1996;98:236–241.
Schwartz IL . Low-birth-weight effects of demographic and socioeconomic variables and prenatal care in Pima county, Arizona. West J Med 1990;152:725–728.
Beeram MR, Young M, Abedin M . Effect of maternal illicit drug use on the mortality of very low birth weight infants. J Perinatology 1995;15:456–462.
Feldman JG, Minkoff HL, McCalla S, et al. A cohort study on the impact of perinatal drug use on prematurity in an inner-city population. Am J Public Health 1992;82:726–728.
Fitzsimmons J, Tunis S, Webster D, et al. Pregnancy in a drug-abusing population. Am J Drug Alcohol Abuse 1986;12:247–255.
Habel L, Kaye K, Lee J . Trends in reporting of maternal drug abuse and infant mortality among drug-exposed infants in New York City. Women Health 1990;16:41–58.
Lindsay MK, Carmichael S, Peterson H, et al. Correlation between self-reported cocaine use and urine toxicology in an inner-city population. J Natl Med Assoc 1997;89:57–60.
Day NL, Cottreau CM, Richardson GA . The epidemiology of alcohol, marijuana, and cocaine use among women of childbearing age and pregnant women. Clin Obstetr Gynecol. 1993;36:232–245.
NIDA (National Institute on Drug Abuse). The Washington, DC Metropolitan Area Drug Study—Prevalence of drug use among DC women delivering livebirths in DC hospitals: 1992. Washington, DC: US Department of Health and Human Services Public Health Services, National Institutes of Health; 1992.
Jacobson SA, Chiodo LM, Sokol RJ, Jacobson JL . Validity of maternal report of prenatal alcohol, cocaine, and smoking in relation to neurobehavioral outcome. Pediatrics 2002;109(5):815–825.
Handler A, Kistin N, Davis F, et al. Cocaine use during pregnancy: perinatal outcomes. Am J Epidemiol 1991;133:818–825.
Jacobson JL, Jacobson SW, Sokol RJ, et al. Effects of alcohol use, smoking, and illicit drug use on fetal growth in black infants. J Pediatr 1994;127:757–764.
Finnegan LP . Perinatal morbidity and mortality in substance using families: effects and intervention strategies. Bull on Narcotics 1994;46:19–43.
Berenson AB, Wilkinson GS, Lopez LA . Effects of prenatal care on neonates born to drug-using women. Substance Use Misuse 1996;31:1063–1076.
Chazotte C, Youchah J, Freda MC . Cocaine use during pregnancy and low birth weight: the impact of prenatal care and drug treatment. Semin Perinatol. 1995;19:293–300.
MacGregor SN, Keith LG, Bachcha JA, et al. Cocaine abuse during pregnancy outcomes. Obstet Gynecol 1989;74:882–885.
Mastrogiannis DS, Decavales GO, Verman U, et al. Perinatal outcome after recent cocaine usage. Obstet Gynecol 1990;76:8–11.
Racine A, Joyce T, Anderson R . The association between prenatal care and birth weight among women exposed to cocaine in New York City. JAMA 1993;270:1581–1586.
Chasnoff IJ, Neumann K, Thornton C, et al. Screening for substance use in pregnancy: a practical approach for the primary care physician. Am J Obstet Gynecol 2001;184:752–758.
Wiemann CM, Berenson AB, Landwehr BM . Racial and ethnic correlates of tobacco, alcohol and illicit drug use in a pregnant population. J Reprod Med 1995;40:571–578.
Acknowledgements
This work was Supported by grants (U18-HD30447, U18-HD30458, U18-HD30450, U18-HD30445, U18-HD31919, U18-HD30454, and U18-HD31206) from the NICHD and the NIH ORMH.
A Cooperative Agreement funded by The NIH Office of Research on Minority Health and The National Institute of Child Health and Human Development supported this study. The following institutions and investigators participated in the NIH-DC Initiative to Reduce Infant Mortality in Minority Populations in the District of Columbia: The Children's National Medical Center — P.C. Scheidt (Principal Investigator), The D.C. Department of Public Health — B.J. Hatcher (Principal Investigator), D.C. General Hospital — L. Johnson (Principal Investigator), Georgetown University Medical Center — K.N. Sivasubramanian (Principal Investigator), Howard University — B.D. Wesley (Principal Investigator), The University of the District of Columbia — V. Melnick (Principal Investigator), The Research Triangle Institute — A.V. Rao (Principal Investigator), The NICHD—H.W. Berendes (Program Officer), A.A. Herman (Scientific Coordinator), B.K. Wingrove (Program Coordinator).
Other participating institutions were Columbia Hospital for Women Medical Center and The George Washington University Medical Center.
We thank Dr. Michele Kiely, the NICHD program officer, for her valuable comments and suggestions on an earlier draft of this paper.
Author information
Authors and Affiliations
Additional information
Participating institutions are listed in the acknowledgements.
Rights and permissions
About this article
Cite this article
El-Mohandes, A., Herman, A., Nabil El-Khorazaty, M. et al. Prenatal Care Reduces the Impact of Illicit Drug use on Perinatal Outcomes. J Perinatol 23, 354–360 (2003). https://doi.org/10.1038/sj.jp.7210933
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jp.7210933
This article is cited by
-
They Will Never Forget How You Made Them Feel: Implementing Harm Reduction in the Perinatal Setting
Maternal and Child Health Journal (2023)
-
Racial and Ethnic Differences in Urine Drug Screening on Labor and Delivery
Maternal and Child Health Journal (2022)
-
Developmental exposure to Δ9-tetrahydrocannabinol (THC) causes biphasic effects on longevity, inflammation, and reproduction in aged zebrafish (Danio rerio)
GeroScience (2020)
-
Risk of preterm and early term birth by maternal drug use
Journal of Perinatology (2019)
-
Marijuana use and pregnancy: prevalence, associated characteristics, and birth outcomes
Archives of Women's Mental Health (2016)
