
Abstract
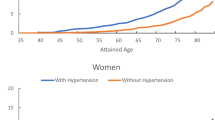
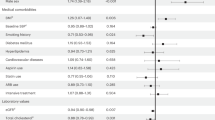
The aim was to examine the risk profiles and prognosis of treated and untreated hypertensive subjects and examine to what degree confounding by indication was present in a population-based cohort study with up to 30-year follow-up. The study population consisted of 9328 men and 10 062 women, aged 33–87 years at the time of attendance from 1967 to 1996. The main outcome measures were myocardial infarction (MI), cardiovascular disease (CVD) mortality and all-cause mortality. Comparing the risk profiles between treated and untreated subjects entering the study showed significantly higher values for some risk factors for treated subjects. During the first 10 years, hypertensive men without treatment, compared with those treated, had a significantly lower risk of suffering MI, CVD and all-cause mortality, hazard ratio (HR) 0.72 (95% CI; 0.57, 0.90), 0.75 (95% CI; 0.59, 0.95) and 0.81 (95% CI; 0.61, 0.98), respectively. No significant differences in outcome were seen during the following 20 years. In identically defined groups of women, no significant differences in mortality were seen between groups. Subgroup analysis, at two stages of the study 5 years apart, revealed that some cardiovascular risk factors had a higher prevalence in hypertensive men who were treated at the later stage, compared with those who remained untreated (P=0.004). In conclusion, hypertensive treated men had a worse prognosis during the first 10 years of follow-up than untreated ones, which is most likely due to worse baseline risk profile. Hypertensive men that were treated at a later stage had a worse risk profile than those not treated at a later stage.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Kannel WB . Elevated systolic blood pressure as a cardiovascular risk factor. Am J Cardiol 2000; 85: 251–255.
Klag MJ et al. Blood pressure and end-stage renal disease in men. N Engl J Med 1996; 334: 13–18.
Mosterd A et al. Trends in the prevalence of hypertension, antihypertensive therapy, and left ventricular hypertrophy from 1950 to 1989. N Engl J Med 1999; 340: 1221–1227.
Burt VL et al. Prevalence of hypertension in the US adult population. Results from the Third National Health and Nutrition Examination Survey, 1988–1991. Hypertension 1995; 25: 305–313.
Hansson L, Lloyd A, Anderson P, Kopp Z . Excess morbidity and cost of failure to achieve targets for blood pressure control in Europe. Blood Press 2002; 11: 35–45.
Collins R et al. Blood pressure, stroke, and coronary heart disease. Part 2, short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet 1990; 335: 827–838.
Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP). SHEP Cooperative Research Group. JAMA 1991; 265: 3255–3264.
Coope J, Warrender TS . Randomised trial of treatment of hypertension in elderly patients in primary care. Br Med J (Clin Res Ed) 1986; 293: 1145–1151.
Medical Research Council trial of treatment of hypertension in older adults: principal results. MRC Working Party. BMJ 1992; 304: 405–412.
Kannel WB, Sorlie P, McNamara PM . Prognosis after initial myocardial infarction: the Framingham study. Am J Cardiol 1979; 44: 53–59.
Sigurdsson E et al. Long-term prognosis of different forms of coronary heart disease: The Reykjavik Study. Int J Epidemiol 1995; 24: 58–68.
Thurmer HL, Lund-Larsen PG, Tverdal A . Is blood pressure treatment as effective in a population setting as in controlled trials? Results from a prospective study. J Hypertens 1994; 12: 481–490.
Sytkowski PA, D'Agostino RB, Belanger AJ, Kannel WB . Secular trends in long-term sustained hypertension, long-term treatment, and cardiovascular mortality. The Framingham Heart Study 1950 to 1990. Circulation 1996; 93: 697–703.
Andersson OK et al. Survival in treated hypertension: follow up study after two decades. BMJ 1998; 317: 167–171.
Miettinen OS . The need for randomization in the study of intended effects. Stat Med 1983; 2: 267–271.
Walker AM, Stampfer MJ . Observational studies of drug safety. Lancet 1996; 348: 489.
Grobbee DE, Hoes AW . Confounding and indication for treatment in evaluation of drug treatment for hypertension. BMJ 1997; 315: 1151–1154.
Sigurdsson E, Thorgeirsson G, Sigvaldason H, Sigfusson N . Prevalence of coronary heart disease in Icelandic men 1968–1986. The Reykjavik Study. Eur Heart J 1993; 14: 584–591.
Jonsdottir LS, Sigfusson N, Sigvaldason H, Thorgeirsson G . Incidence and prevalence of recognised and unrecognised myocardial infarction in women. The Reykjavik Study. Eur Heart J 1998; 19: 1011–1018.
Rose G, McCartney P, Reid DD . Self-administration of a questionnaire on chest pain and intermittent claudication. Br J Prev Soc Med 1977; 31: 42–48.
Rose GA, Blackburn H . Cardiovascular population studies: Methods. World Health Organization: Geneva, 1966.
Rose GA, Blackburn H . Cardiovascular Survey Methods. WHO: Geneva, 1968.
The World Health Organization MONICA Project (monitoring trends and determinants in cardiovascular disease): a major international collaboration. WHO MONICA Project Principal Investigators. J Clin Epidemiol 1988; 41: 105–114.
Sigfusson N et al. Decline in ischaemic heart disease in Iceland and change in risk factor levels. BMJ 1991; 302: 1371–1375.
Bjornsson OJ et al. Survey of serum lipid levels in Icelandic Men aged 34–61 years. An epidemiological and statistical evaluation. Acta Med Scand 1977; 616(Suppl): 1–150.
Sigurdsson E, Sigfusson N, Sigvaldason H, Thorgeirsson G . Silent ST-T changes in an epidemiologic cohort study—a marker of hypertension or coronary heart disease, or both: The Reykjavik study. J Am Coll Cardiol 1996; 27: 1140–1147.
Cox DR . Regression models and lifetables. J Roy Statist Soc 1972; 34: 187–220.
MacMahon S et al. Blood pressure, stroke, and coronary heart disease. Part 1, prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet 1990; 335: 765–774.
Gebsky V, Leung O, McNeil D, Lunn D . Statistical package for interactive data analysis (SPIDA), 6th Edn. Statistical computing lab, Macquarie University, NSW Australia, 1992.
Fahey TP, Peters TJ . What constitutes controlled hypertension? Patient based comparison of hypertension guidelines. BMJ 1996; 313: 93–96.
Psaty BM et al. Assessment and control for confounding by indication in observational studies. J Am Geriatr Soc 1999; 47: 749–754.
Sigfusson N . Hypertension in middle-aged men. Acta Med Scand 1986; 710(Suppl): 1–131.
Acknowledgements
We thank all the employees of the Icelandic Heart Preventive Clinic (Hjartavernd) for their skilful contribution to the data collection. The Medical Faculty and the Research Fund of the University of Iceland and the Icelandic Research Council supported this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gudmundsson, L., Johannsson, M., Thorgeirsson, G. et al. Risk profiles and prognosis of treated and untreated hypertensive men and women in a population-based longitudinal study The Reykjavik Study. J Hum Hypertens 18, 615–622 (2004). https://doi.org/10.1038/sj.jhh.1001725
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jhh.1001725
Keywords
This article is cited by
-
Mortality in persons with undetected and diagnosed hypertension, type 2 diabetes, and hypothyroidism, compared with persons without corresponding disease - a prospective cohort study; The HUNT Study, Norway
BMC Family Practice (2017)
-
Observational study and participant-level meta-analysis on antihypertensive drug treatment-related cardiovascular risk
Hypertension Research (2017)
-
Cardiovascular mortality among a cohort of hypertensive and normotensives in Rio de Janeiro - Brazil - 1991–2009
BMC Public Health (2015)
-
Stroke Risk in Treated Hypertension Based on Home Blood Pressure: the Ohasama Study
American Journal of Hypertension (2010)
-
Association of Hypertension Treatment and Control With All-Cause and Cardiovascular Disease Mortality Among US Adults With Hypertension
American Journal of Hypertension (2010)
