
Abstract
Objective: Recent studies indicate that abdominal fat accumulation, in particular intra-abdominal fat, is related to impaired endothelial function in young healthy volunteers. The aim of this study was to examine whether the distribution of body fat depots is related to impaired endothelial function in older men.
Methods: Cross-sectional sample of 38 older (68±1 y) sedentary (VO2max=2.4±0.1 l/min) men. Flow-mediated endothelial dependent vasodilation (EDD) was assessed in the brachial artery in response to reactive hyperemia using high-resolution ultrasound. Abdominal subcutaneous and visceral fat depots were assessed by computed tomography scan (CT-scan) at the L4–L5 region in the supine position. Percentage body fat was assessed via dual-energy X-ray absorptiometry (DEXA).
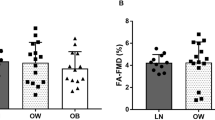
Results: Flow-mediated percentage change in brachial artery was 7.6±0.7%, suggesting an impaired flow-mediated EDD. Using simple linear regression analysis, there were no statistically significant relationship observed between flow-mediated EDD and the indices of total and abdominal adiposity (percentage body fat=29.3±0.9%, r=−0.11; total abdominal fat area=465±23 cm2, r=−0.1; intra-abdominal fat area=200±14 cm2, r=−0.14; subcutaneous fat area=265±13 cm2, r=−0.05; BMI=29.3±0.9 kg/m2, r=−0.07; and waist to hip ratio=0.98±0.01, r=−0.20).
Conclusion: These findings suggest that in older sedentary men there is no clear correlation between adiposity and body fat distribution and impairment of flow-mediated endothelium dependent vasodilation.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout






Similar content being viewed by others


References
Flavahan NA, Vanhoutte PM . Endothelial cell signaling and endothelial dysfunction Am J Hypertension 1995 8: 28S–241S.
Arcaro G, Zamboni M, Rossi L, Turcato E, Covi G, Armellini F, Bosello O, Lechi A . Body fat distribution predicts the degree of endothelial dysfunction in uncomplicated obesity Int J Obes Relat Metab Disord 1999 23: 936–942.
Baldeweg SE, Pink AM, Yudkin JS, Coppack SW . The relationship between obesity, vascular reactivity and endothelial dysfunction in subjects with non-insulin dependent diabetes mellitus Int J Obes Relat Metab Disord 2000 24: S134–S135.
Perticone F, Ceravolo R, Candigliota M, Ventura G, lacopino S, Sinopoli F, Mattioli PL . Obesity and body fat distribution induce endothelial dysfunction by oxidative stress: protective effect of vitamin C Diabetes 2001 50: 159–165.
Hashimoto M, Akishita M, Eto M, Kozaki K, Ako J, Sugimoto N, Yoshizumi M, Toba K, Ouchi Y . The impairment of flow-mediated vasodilatation in obese men with visceral fat accumulation Int J Obes Relat Metab Disord 1998 22: 477–484.
Steinberg HO, Chaker H, Leaming R, Johnson A, Brechtel G, Baron AD . Obesity/insulin resistance is associated with endothelial dysfunction: implications for the syndrome of insulin resistance J Clin Invest 1996 97: 2601–2610.
Kissebah AH, Krakower GR . Regional adiposity and morbidity Physiol Rev 1994 74: 761–811.
Peiris AN, Sothmann MS, Hoffmann RG, Hennes MI, Wilson CR, Gustafson AB, Kissebah AH . Adiposity, fat distribution, and cardiovascular risk Ann Intern Med 1989 110: 867–872.
Despres JP, Moorjani S, Lupien PJ, Tremblay A, Nadeau A, Bouchard C . Regional distribution of body fat, plasma lipoproteins, and cardiovascular disease Arteriosclerosis 1990 10: 497–511.
Hogikyan RV, Galecki AT, Pitt B, Halter JB, Greene DA, Supiano MA . Specific impairment of endothelium-dependent vasodilation in subjects with type 2 diabetes independent of obesity J Clin Endocrinol Metab 1998 83: 1946–1952.
Taddei S, Virdis A, Mattei P, Ghiadoni L, Gennari A, Fasolo CB, Sudano I, Salvetti A . Aging and endothelial function in normotensive subjects and patients with essential hypertension Circulation 1995 91: 1981–1987.
Taddei S, Virdis A, Mattei P, Ghiadoni L, Fasolo CB, Sudano I, Salvetti A . Hypertension causes premature aging of endothelial function in humans Hypertension 1997 29: 736–743.
Gerhard M, Roddy MA, Creager SJ, Creager MA . Aging progressively impairs endothelium-dependent vasodilation in forearm resistance vessels of humans Hypertension 1996 27: 849–853.
Celermajer DS, Sorensen KE, Spiegelhalter DJ, Georgakopoulos D, Robinson J, Deanfield JE . Aging is associated with endothelial dysfunction in healthy men years before the age-related decline in women J Am Coll Cardiol 1994 24: 471–476.
Corretti MC, Plotnick GD, Vogel RA . The effects of age and gender on brachial artery endothelium-dependent vasoactivity are stimulus-dependent Clin Cardiol 1995 18: 471–476.
Taddei S, Virdis A, Ghiadoni L, Mattei P, Sudano I, Bernini G, Pinto S, Salvetti A . Menopause is associated with endothelial dysfunction in women Hypertension 1996 28: 576–582.
Mauriege P, Prud'homme D, Marcotte M, Yoshioka M, Trembly A, Bouchard C, Nadeau A, Depres J . Regional differences in adipose tissue metabolism between sedentary and endurance-trained women Am J Physiol Endocrinol Metab 1996 273: E497–E506.
National Diabetes Data Group. Report of the expert committee on the diagnosis and classification of diabetes mellitus Diabetes Care 1997 20: 1183–1201.
Ryan AS, Nicklas BJ . Age-related changes in fat deposition in mid-thigh muscle in women: relationships with metabolic cardiovascular disease risk factors Int J Obes Relat Metab Disord 1999 23: 126–132.
Nicklas BJ, Ryan AS, Katzel LI . Lipoprotein subfractions in women athletes: effects of age, visceral obesity and aerobic fitness Int J Obes Relat Metab Disord 1999 23: 41–47.
Friedewald WT, Levy RF, Fredrickson DS . Estimations of concentrations of low density lipoprotein cholesterol in plasma, without use of preparative ultracentrifuge Clin Chem 1972 18: 499–502.
Meyers D, Goldberg AP, Coon PJ, Drinkwater DT, Bleecker ER . Relationship of obesity and physical fitness to cardiopulmonary and metabolic function in healthy older men J Gerontol 1991 46: M57–M65.
Corretti MC, Plotnick GD, Vogel RA . Technical aspects of evaluating brachial artery vasodilation using high-frequency ultrasound Am J Physiol 1995 268: H1397–H1404.
Cosentino F, Luscher TF . Endothelial dysfunction in diabetes mellitus J Cardiovasc Pharmac 1998 32 (Suppl 3): S54–S61.
Tschudi MR, Barton M, Bersinger NA, Moreau P, Cosentino F, Noll G, Malinski T, Luscher TF . Effects of age on kinetics of nitric oxide release in rat aorta and pulmonary artery J Clin Invest 1996 98: 899–905.
Perticone F, Ceravolo R, Candigliota M, Ventura G, Iacopino S, Sinopoli F, Mattioli PL . Obesity and body fat distribution induce dysfunction by oxidative stress: protective effect of vitamin C Diabetes 2001 50: 159–165.
Hirai N, Kawano H, Hirashima O, Motoyama T, Moriyama Y, Sakamoto T, Kugiyama K, Ogawa H, Nakao K, Yasue H . Insulin resistance and endothelial dysfunction in smokers: effects of vitamin C Am J Physiol Heart Circul Physiol 2000 279: H1172–H1178.
Rywik TM, Blackman MR, Yataco AR, Waitkevicius PV, Zink RC, Cottrell EH, Wright JG, Katzel LI, Fleg JL . Enhanced endothelial vasoreactivity in endurance-trained older men J Appl Physiol 1999 87: 2136–2142.
Acknowledgements
We would like to thank the patients who participated in this study. We would also like to thank the staff at the Department of Veterans Affairs Baltimore Geriatric Research, Education and Clinical Center for screening and recruiting. This work was supported by the Department of Veteran Affairs Baltimore Geriatric Research, Education and Clinical Center, Baltimore, Maryland; the University of Maryland Claude D Pepper Older Americans Independence Center (NIA P60 AG12583), a K24 mid-career development grant (K24 AG00930), an NIH training grant (T32 AG00219), and by a Special Emphasis Research Career Award (NIA K01 AG00657).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Joseph, L., Ryan, A., Sorkin, J. et al. Body fat distribution and flow-mediated endothelium-dependent vasodilation in older men. Int J Obes 26, 663–669 (2002). https://doi.org/10.1038/sj.ijo.0801972
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ijo.0801972
