
Abstract
OBJECTIVE: To examine demographic, behavioral and dietary correlates of frequency of fast food restaurant use in a community-based sample of 891 adult women.
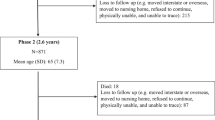
DESIGN: A survey was administered at baseline and 3 y later as part of a randomized, prospective intervention trial on weight gain prevention.
SUBJECTS: Women (n=891) aged 20–45 y who enrolled in the Pound of Prevention study.
MEASUREMENTS: Frequency of fast food restaurant use, dietary intake, demographic and behavioral measures were self-reported. Dietary intake was measured using the 60-item Block Food Frequency Questionnaire. Body weight and height were directly measured.
RESULTS: Twenty-one percent of the sample reported eating ≥3 fast food meals per week. Frequency of fast food restaurant use was associated with higher total energy intake, higher percentage fat energy, more frequent consumption of hamburgers, French fries and soft drinks, and less frequent consumption of fiber and fruit. Frequency of fast food restaurant use was higher among younger women, those with lower income, non-White ethnicity, greater body weight, lower dietary restraint, fewer low-fat eating behaviors, and greater television viewing. Over 3 y, increases in frequency of fast food restaurant use were associated with increases in body weight, total energy intake, percentage fat intake, intake of hamburgers, French fries and soft drinks, and with decreases in physical activity, dietary restraint and low-fat eating behaviors. Intake of several other foods, including fruits and vegetables, did not differ by frequency of fast food restaurant use.
CONCLUSION: Frequency of fast food restaurant use is associated with higher energy and fat intake and greater body weight, and could be an important risk factor for excess weight gain in the population.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others


References
US Department of Health and Human Services . Healthy People 2000: National Health promotion and disease prevention objective US Department of Health and Human Services, Public Health Service: Washington DC 1988.
McDowell MA, Briefel RR, Alaimo R, Bischof AM, Caughman CR, Carroll MD, Loria CM, Johnson CL . Energy and macronutrient intakes of persons ages 2 months and over in the United States: Third National Health and Nutrition Examination Survey, Phase 1, 1988–91 Advance Data From Vital and Health Statistics, no. 255, National Center for Health Statistics: Hyattsville, MD 1994.
Borrud L, Wilkinson-Enns C, Mickle S . What we eat: USDA surveys food consumption changes CNI 1997 18: 4–5.
Hill J, Peters J . Environmental contributions to the obesity epidemic Science 1998 280: 1371–1374.
Shah M, Jeffery R . Is obesity due to overeating and inactivity, or to a defective metabolic rate: a review Ann Behav Med 1991 13: 73–81.
Kruczmarski RJ, Flegal KM, Campbell SM, Johnson CL . Increasing prevalence of overweight among US adults: the National Health and Nutrition Examination Surveys, 1960–1991 JAMA 1994 272: 205–211.
Flegal KM, Harlan WR, Landis JR . Secular trends in body mass index and skinfold thickness with socioeconomic factors in young adult women Am J Clin Nutr 1988 48: 535–543.
Flegal KM, Harlan WR, Landis JR . Secular trends in body mass index and skinfold thickness with socioeconomic factors in young adult men Am J Clin Nutr 1988 48: 544–551.
Shah M, Hannan PJ, Jeffery RW . Secular trend in body mass index in the adult population of three communities from the upper mid-western part of the USA: the Minnesota Heart Health Program Int J Obes 1991 15: 499–503.
Biing-Hwan L, Frazao E . Nutritional quality of foods at and away from home. Food review. US Government Printing Office, Food and Rural Economics Division, Economics Research Service, USDA 1997, pp 33–40.
USDA continuing survey of food intakes by individuals, 1994–1996 US Department of Agriculture, Economic Research Service: Washington DC 1997.
Sheridan M, McPherrin E . Fast food and the American diet American Council of Science and Health: New York 1983.
Putnam J, Allshouse J . Food consumption, prices, and expenditures, 1996, SB-928 US Department of Agriculture, Economic Research Service: Washington, DC April 1996.
Shannon BM, Parks SC . Fast foods: a perspective on their nutritional impact J Am Diet Assoc 1980 76: 242–247.
Guenther PM, Ricart G . Effects of eating at food service establishments on the nutritional quality of women's diets Top Clin Nutr 1989 4: 41–45.
Haines PS, Popkin BM, Guilkey DK . Methods of patterning eating behaviors of American women J Nutr Educ 1990 22: 124–132.
Greecher CP, Shannon B . Impact of fast food meals on nutrient intake of two groups J Am Diet Assoc 1977 70: 368–372.
Eck-Clemens LH, Slawson DL, Klesges RC . The effect of eating out on quality of diet in premenopausal women J Am Diet Assoc 1999 99: 442–444.
Schwenk NE . Trends in food and alcohol consumption away from home Family Econ Nutr Rev 1995 8: 30–40.
Ries CP, Kline K, Weaver SO . Impact of commercial eating on nutrient adequacy J Am Diet Assoc 1987 87: 463–468.
Consumer Reports. Where's the beef? Consumer Reports 1984 July: 367–373.
Jeffery RW, French SA . Epidemic obesity in the US: are fast foods contributing? Am J Public Health 1998 88: 277–280.
Jeffery RW, French SA . Prevention of weight gain in adults: the Pound of Prevention Study Am J Public Health 1999 89: 747–751.
Block G, Hartman AM, Dresser CM, Carroll MD, Gannon J, Gardener L . A data-based approach to diet questionnaire design and testing Am J Epidemiol 1986 124: 453–469.
Mares-Perlman JA, Klein BE, Klein R, Ritter LL, Fisher MR, Freudenheim JL . A diet history questionnaire ranks nutrient intakes in middle-aged and older men and women similarly to multiple food records J Nutr 1993 123: 489–501.
Block G, Woods M, Potosky A, Clifford C . Validation of a self-administered diet history questionnaire using multiple diet records J Clin Epidemiol 1990 43: 1327–1335.
Block G, Thompson FE, Hartman AM, Larkin FA, Guire KE . Comparison of two dietary questionnaires validated against multiple dietary records collected during a 1-year period J Am Diet Assoc 1992 92: 686–693.
Coates RJ, Eley JW, Block G, Gunter EW, Sowell Al, Grossman C, Greenberg RS . An evaluation of a food frequency questionnaire for assesing dietary intake of specific carotenoids and vitamin E among low-income black women Am J Epidemiol 1991 134: 658–371.
Jacobs DR, Hahn LP, Haskell WL, Pirie P, Sidney S . Validity and reliability of short physical activity history: CARDIA and the Minnesota Heart Health Program J Cardiopulmon Rehab 1989 9: 448–459.
Stunkard AJ, Messick S . The three factor eating questionnaire to measure dietary restraint, disinhibition, and hunger J Psychosom Res 1985 29: 71–83.
Laessle RG, Tuschl RJ, Kotthaus BC, Pirke KM . A comparison of the validity of three scales for the assessment of dietary restraint J Abnorm Psychol 1989 98: 504–507.
Tuschl RJ, Platte P, Laessle RG, Stichler W, Pirke KM . Energy expenditure and everyday eating behavior in healthy young women Am J Clin Nutr 1990 52: 81–86.
Kristal AR, White E, Shattuck AL, Curry S, Anderson GL, Fowler A, Urban N . Long-term maintenance of a low-fat diet: durability of fat-related dietary habits in the Women's Health Trial J Am Diet Assoc 1992 92: 553–559.
SAS Institute Inc . SAS/STAT software: changes and enhancements through release 6.12 SAS Institute: Cary, NC 1997.
Cohen J, Cohen P . Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences Erlbaum: Hillsdale, NJ 1975, pp 72–73, 413–423.
Consumer Reports. Fast food for fat-watchers Consumer Rep 1993 September 574–578.
Kramer L . Taco Bell ‘lightens up’ on Border Lights. Taco Bell amends its Border Lights menu and launches Lighten Up Nation's Restaurant News 1996 30: 1.
Jekanowski M . Causes and consequences of fast food sales growth USDA/ERS Food Rev 1999 22: 11–16.
Liquid candy: how soft drinks are harming American's health. Center for Science in the Public Interest: Washington, DC, 1998.
Harnack L, Stang J, Story M . Soft drink consumption among US children and adolescents: nutritional consequences J Am Diet Assoc 1999 99: 436–441.
Story M, Faulkner P . The prime time diet: a content analysis of eating behavior and food messages in television program content and commercials Am J Public Health 1990 80: 738–740.
Kotz K, Story M . Food advertisements during children's Saturday morning television programming: are they consistent with dietary recommendations? J Am Diet Assoc 1994 94: 1296–1300.
Zenith teams with McDonald's in Monopoly promo . Brandweek 2000 41: 90 (Article A61408896).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
French, S., Harnack, L. & Jeffery, R. Fast food restaurant use among women in the Pound of Prevention study: dietary, behavioral and demographic correlates. Int J Obes 24, 1353–1359 (2000). https://doi.org/10.1038/sj.ijo.0801429
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ijo.0801429
Keywords
This article is cited by
-
Impact of Changes in Chain Restaurant Calories over Time on Obesity Risk
Journal of General Internal Medicine (2020)
-
A computer-based approach for analyzing consumer demands in electronic word-of-mouth
Electronic Markets (2017)
-
Fast-food and full-service restaurant consumption and daily energy and nutrient intakes in US adults
European Journal of Clinical Nutrition (2016)
-
Effects of a mindfulness-based intervention on mindful eating, sweets consumption, and fasting glucose levels in obese adults: data from the SHINE randomized controlled trial
Journal of Behavioral Medicine (2016)
-
Fast Food Intake in Relation to Employment Status, Stress, Depression, and Dietary Behaviors in Low-Income Overweight and Obese Pregnant Women
Maternal and Child Health Journal (2016)
