
Abstract
We examined the contribution of transforming growth factor (TGF)-β-T-cell signaling to aldosterone (aldo)/salt-induced fibrosis in the kidneys and the hearts of FVB/N wild-type (WT) or transgenic (Tg) mice expressing a dominant-negative TGF-β type II receptor in T cells (hCD2-ΔkTβRII). Animals received aldo through osmotic minipumps and had access to either 1% NaCl (aldo/NaCl group) or tap water (vehicle group) for 4 weeks. Systolic blood pressure was measured during this period via a tail cuff. The animals were then killed, and urine, blood, kidneys and hearts were collected. Systolic blood pressure did not differ between the groups. Aldo/NaCl enhanced renal, cardiac and left ventricular weight in WT animals slightly, but only renal weight was increased in Tg animals. Urinary protein excretion was enhanced in Tg animals (fourfold) and increased further in WT (twofold) and Tg (1.8-fold) mice on aldo/NaCl treatment. Aldo/NaCl increased interstitial fibrosis in the kidneys (1.5-fold) and the hearts of WT (2.5-fold) animals. Under control conditions, Tg mouse cardiac (3.2-fold) and renal (1.7-fold) tissues were slightly more fibrotic compared with WT, and this condition was not further aggravated by aldo/NaCl. Aldo/NaCl-induced mRNA expression of renal fibronectin (10.7-fold in WT) but not of renal collagen mRNA expression (WT: Col1a1 7.7-fold; Col3a1, 3.1-fold; and Col4a1 3.3-fold) was abrogated in Tg animals. In hearts, aldo/NaCl-induced plasminogen activator inhibitor-1 mRNA (twofold) expression depended on TGF-β-T-cell signaling. Our results indicate that (i) aldo/NaCl can induce renal and cardiac damage in the absence of blood pressure changes, (ii) the elimination TGF-β-T-cell cross-talk leads to renal and cardiac fibrosis but does not exacerbate aldo/NaCl-induced damage and (iii) the pathological aldo/NaCl effect is modified, in part, by TGF-β-T-cell cross-talk.
Similar content being viewed by others


Introduction
It has been shown that counteracting angiotensin II action prevents cardiovascular events and the progression of renal failure in patients with vascular and hypertensive diseases.1 Recently, the mineralocorticoid receptor (MR) and its ligand, aldosterone (aldo), have gained attention because both have been identified as important pathogenic mediators of end-organ damage, independent of the angiotensin II type 1 receptor and its ligand.2, 3 Rocha et al.4 demonstrated that eplerenone, an aldo antagonist, was able to prevent angiotensin II/salt-induced vascular inflammation in the rat heart. This vascular inflammation is at least, in part, mediated through a mechanism not related to blood pressure or renal sodium retention.5, 6, 7, 8
Aldo binds to the MR, which belongs to the nuclear receptor superfamily and acts as a ligand-dependent transcription factor.9 Under physiological conditions, aldo enhances sodium reabsorption in the distal nephron of the kidney and enhances potassium excretion, an effect facilitated by aldo-induced Na+ reabsorption.10 MR can be detected in epithelial cells and in non-epithelial tissues, such as cardiomyocytes, vascular smooth muscle cells, endothelial cells and some cells of the immune system, including dendritic cells; inappropriate activation in these cells can have pathophysiological consequences.11, 12, 13 For example, inappropriate MR activation induces renal fibrosis, which is accompanied by increased transforming growth factor-β (TGF-β) expression at sites of fibrosis in the damaged kidneys and moderately increased monocyte/macrophage infiltration.14 This increase in infiltrating immune cells is a main feature of renal fibrosis15 and is involved in cardiac fibrosis.6, 13 When MR is deleted in monocytes/macrophages, the increased infiltration of immune cells persists, whereas the blood pressure increase on MR stimulation and cardiac fibrosis is reduced after 8 weeks.16 T cells may also contribute to aldo/NaCl-mediated fibrosis because the adoptive transfer of T cells to RAG1−/− (T and B cell null) mice restored the hypertensive phenotype in mineralocorticoid/NaCl-treated mice.17
One important effect of pathological MR activation is enhanced TGF-β expression, for example, in cardiomyocytes and the kidney.18, 19, 20, 21, 22 TGF-β may enhance matrix protein expression by a direct action in renal or cardiovascular tissue, but it could also modulate inflammatory pathways and thereby promote fibrosis and tissue remodeling (for review, see ref. 23, 24). Previous studies have demonstrated the requirement of the active form of TGF-β in mediating the effects of aldo in neonatal cardiomyocytes.25 Conversely, TGF-β exerts anti-inflammatory properties, as shown in atherosclerosis, by regulating the survival of lymphocytes, natural killer cells and dendritic cells.22 Additionally, TGF-β exerts multifunctional effects on T cells (for review, see ref. 26, 27). It has recently been shown that aldo promotes Th17-polarized immune responses through the modulation of dendritic cell function, resulting in enhanced TGF-β secretion.12 This secretion may contribute to the inflammatory damage leading to hypertension and cardiovascular disease.
Mice with a loss-of-function mutation in the TGF-β signaling cascade show up to 100% embryonic lethality depending on the genetic background; surviving mice are characterized by a multifocal inflammatory response.26 Therefore, we used a mouse model in which the TGF-β pathway is interrupted solely in T cells.28, 29, 30 These transgenic (Tg) mice express a dominant-negative TGF-β type II receptor that lacks the intracellular kinase domain responsible for the activation of the signaling cascade and is under the control of the human CD2 promoter in T cells.30 These mice have been shown to be more susceptible to collagen-induced arthritis and autoimmune hepatitis, and less susceptible to airway hyperreactivity, with a shift in the activated T cell phenotype toward Th1 cells.28, 29, 30
The aim of our study was to investigate whether the role of TGF-β in aldo/NaCl-induced renal and cardiac damage depends on cross-talk with T cells and whether this effect is mediated by the activated MR.
Methods
Animals
Mice were housed in a room maintained at 22±2 °C and exposed to a 12-h dark/light cycle. All procedures performed on animals were done in accordance with the guidelines of the American Physiological Society and were approved by the Landesverwaltungsamt Sachsen-Anhalt, Halle, Germany; the permission number was 42502-02-691 MLU.
The generation and characterization of Tg hCD2-ΔkTβRII mice is described elsewhere.28 All Tg lines were established and maintained as heterozygotes on an FVB/N wild-type (WT) background. Detailed information is available at http://www.jaxmice.jax.org/strain/001800.html. Non-Tg littermates (WT) were used as controls. Aldo/NaCl treatment was performed by infusion of aldo (0.6 μg per day and g body weight (BW)) or vehicle via osmotic minipumps. Plasma aldo levels were significantly higher in aldo-treated animals (WT 11.09±2.07 nmol l−1 and Tg 14.80±1.52 nmol l−1; N=5 animals per group) compared with vehicle-treated animals (WT 4.42±0.83 nmol l−1, N=4; Tg 3.89±0.72 nmol l−1, N=6), but they did not differ between genotypes, demonstrating the successful delivery of aldo. The 6-month-old animals of 27±2 g BW were trained for blood pressure measurements for 14 days before blood pressure measurements were recorded for 35 days. After 7 days, animals underwent minipump implantation. For implantation, the animals were anesthetized with esketamine (50 mg per kg BW, Pfizer, Karlsruhe, Germany) and xylazine (5 mg per kg BW, Bayer Healthcare, Leverkusen, Germany). The mice had free access to standard chow and to either 1% NaCl (aldo/NaCl group) or tap water (vehicle group).
Measurement of blood pressure and urinary protein excretion
After a 2-week training period, baseline (day 0) blood pressure was measured daily for 1 week. To acclimate the animals to the procedure, blood pressure was measured twice weekly by tail cuff using external tail pulse detection (ADI instruments, Spechbach, Germany) in awake animals after surgery. The average of 7–15 measurements was taken as the representative pressure for a single animal. At 28 days after surgery, blood pressure was measured for the final time, and the animals were killed the following morning. When the mice were killed, spontaneous urine was collected to determine the protein/creatinine ratio. The Bio-Rad Protein Assay (Bio-Rad Laboratories, Munich, Germany) was used to measure the protein content. Creatinine was measured via the Jaffé reaction, as published previously.31
Organ harvesting
Immediately after death, kidneys and hearts were excised, carefully freed from adjacent tissue and weighed. Subsequently, the left ventricle was separated and weighed. Furthermore, tibia length was measured for normalization of organ weights. Portions of the kidneys and the left ventricles were immediately snap frozen in liquid nitrogen for later RNA extraction, whereas the remaining portions were placed in a 3% paraformaldehyde solution for fixation. Tissues were dehydrated by bathing in increasing concentrations of methanol or isopropanol. After embedding in paraffin, 3 μm sections were cut.
Determination of blood parameters
The following parameters were analyzed in the animal blood samples: aldo (Aldosterone ELISA, IBL, Hamburg, Germany), glucose (Accu Chek, Roche, Mannheim, Germany), hematocrit, blood cell distribution and plasma urea (QuantiChrom Urea Assay, BioTrend, Cologne, Germany). Hematocrit was determined via differential centrifugation and is expressed in v/v %. For blood cell distribution, blood smears were stained with the May-Gruenwald stain (Roth, Karlsruhe, Germany) and microscopically analyzed.
Kidney and heart inflammation and fibrosis
The degree of interstitial fibrosis was determined by evaluation of the Sirius red–stained area, utilizing a point counting technique as described elsewhere.32
Glomerulosclerosis was evaluated in kidney sections stained with periodic acid-Schiff's reagent. A score of 0–4, based on the sclerotic area of the glomerulus, was used according to Raij et al.33 At least 50 glomeruli per section were evaluated, and the glomerulosclerosis index is given as the mean score per animal.
Gene expression
RNA was isolated using the RNeasy Mini Kit from Qiagen (Hilden, Germany) according to the manufacturer's instructions. Subsequently, the remaining DNA was digested with DNase I. Reverse transcription was performed with 1 μg RNA and random primers using qScript from Quanta Biosciences (Gaithersburg, MD, USA) according to the manufacturer's protocol. Additionally, each sample was analyzed without reverse transcription. The signals obtained without reverse transcription were negligible (<1%). Finally, real-time amplification was performed with the Stratagene Mx3005P using the Platinum SYBR Green kit (Invitrogen, Karlsruhe, Germany) according to the manufacturer's instructions. The primers used are given in Table 1. Quantitative PCR efficiency was >90%. All primers for genes of interest were intron spanning and have been validated by reverse transcriptase PCR and gel electrophoresis. Furthermore, the primers were validated by melting curve analysis. The relative expression of the genes of interest was calculated according to the 2−ΔΔCt method first described in Applied Biosystems User Bulletin no. 2 (P/N 4303859; http://www.3.appliedbiosystems.com/cms/groups/mcb_support/documents/generaldocuments/cms_040980.pdf), using the 18S signal for normalization. The mean of the values from WT animals was set 100% for each gene (=control), and subsequently, all values for each gene were expressed as % of control. Each sample was analyzed in triplicate. To calculate the increase in mRNA expression, the value of each treated animal was compared with the mean mRNA expression of the respective control group. All values are expressed as fold induction with the respective standard error of the mean. The ‘expected additive effect’ was calculated by summing the mean increase in gene expression upon aldo/NaCl treatment in WT animals and the mean expression level of the appropriate gene in Tg-untreated animals. A common pathway was assumed if the effects of the transgene and the treatment were not additive.
Analysis of data
A two-way analysis of variance, followed by a Bonferroni correction, was used to test the significance of differences between groups. A P-value <0.05 was considered significant. The procedures were carried out using SPSS18 software (IBM Corporation, Somers, NY, USA). Values are displayed as mean±standard error of the mean.
Results
Basic physiological parameters and systolic blood pressure
As shown in Table 2, BW, tibia length and leukocyte distribution were not significantly different in any of the groups. Furthermore, no remarkable differences in blood glucose concentration or hematocrit were observed.
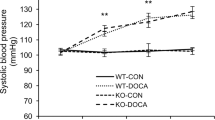
Systolic blood pressure, as measured with the pulse-based tail-cuff technique, was not significantly different among the four groups (Figure 1). In WT animals, the aldo/NaCl treatment slightly increased the systolic blood pressure. Nevertheless, plasma aldo levels were significantly higher in aldo-treated animals (see Methods), demonstrating the successful delivery of aldo. These data indicate that the aldo/NaCl-induced effects in our study do not result from changes in blood pressure.

Effect of aldosterone/NaCl treatment on systolic blood pressure in wild-type (WT) and hCD2-ΔkTβRII (transgenic, Tg) mice measured via a tail cuff. No significant increase in blood pressure was detected among the four groups (N=4–6 animals per group).
Organ weights
In WT animals, aldo/NaCl led to the expected increase in kidney, heart and left ventricular weight adjusted to tibia length (Table 3). Under control conditions, organ weight in Tg animals was not different from WT animals. In Tg animals, aldo/NaCl induced a significant increase in kidney weight but not in heart weight normalized to tibia length (Table 3). Thus, macroscopically, the heart but not the kidney is protected when T cell TGF-β-RII is knocked down.
Interstitial fibrosis
To further elucidate the mechanisms underlying the differences in organ weights, the percentage of Sirius red-stained area per field was evaluated. In the kidneys of WT animals, the accumulation of extracellular matrix proteins on aldo/NaCl treatment was significantly elevated (1.5-fold, Table 3). In Tg mice, the amount of renal extracellular matrix was elevated under control (1.7-fold) conditions compared with WT controls and did not increase further during aldo/NaCl treatment. The relatively high values for Sirius red staining can be explained by the age of the animals (6–7 months). The glomerular injury score, assessed according to Raij et al.,33 was not significantly different among the four groups.
In the hearts of WT animals, the Sirius red-stained interstitial area increased on aldo/NaCl treatment (2.5-fold, Table 3). Under control conditions, the hearts of Tg animals showed a marked increase of Sirius red-stained area (3.2-fold) that did not increase further during aldo/NaCl treatment (Figure 2).

Representative pictures of Sirius red-stained sections of renal fibrosis (magnification × 40) from (a) wild-type (WT), control, (b) transgenic (Tg), control, (c) WT, WT/NaCl and (d) Tg, aldosterone (aldo)/NaCl animals treated with aldo/NaCl. Change in Sirius red-stained area in kidneys (e) and hearts (f) among the four groups. A full color version of this figure is available at the Hypertension Research journal online.
Thus, the effects of aldo/NaCl and TGF-β-RII knockdown were not additive, indicating a common pathway.
Proteinuria and blood urea
To obtain a basic overview with respect to kidney function, spontaneous urine was collected on the day of killing and normalized to urinary creatinine. In WT animals, urinary protein content increased slightly on aldo/NaCl treatment (Table 3). In Tg animals, protein excretion was elevated under control conditions and showed a trend for further increase during aldo/NaCl treatment (Table 3, Figure 3). To distinguish between glomerular and tubular protein loss, we separated urinary proteins by SDS-polyacrylamide gel electrophoresis and stained the gel with silver according to Blum et al.34 Proteins ranging in mass from 20 to 130 kDa were detected (Figure 3), indicating a mild, combined tubulo-glomerular proteinuria. The plasma urea content did not significantly differ among the four experimental groups (Table 3). These data suggest a mild tubulo-interstitial damage without significant excretory restriction. Again, the effects of aldo/NaCl and dominant-negative TGF-β-RII were not additive, indicating a common pathway.

A representative SDS-polyacrylamide gel electrophoresis of urinary proteins in mice. Urine samples of each animal were normalized for creatinine and separated on 12% gels. Proteins were visualized by silver staining (N=4–6 animals per group). See Table 3 for quantitative information about urinary protein content.
Effects on mRNA expression in kidney and heart
Finally, we investigated the mRNA expression of several genes reported to be relevant in aldo/NaCl-induced renal and cardiac injury. Aldo/NaCl treatment induced a similar increase of TGF-β mRNA in the heart and the kidneys of WT animals (2.1±0.5-fold, P<0.05). As shown in Table 4, aldo/NaCl enhanced the expression of fibronectin-1 (Fn-1), collagen I (Col1a1), collagen III (Col3a1) and collagen IV (Col4a1) in WT animals, indicating the stimulation of extracellular matrix generation. These data are consistent with the Sirius red data (Table 3). In Tg mice, Fn-1 and Col1a1 mRNA expression was enhanced under control conditions, indicating stimulated matrix synthesis. Aldo/NaCl treatment in Tg animals significantly elevated Col1a1 and Col4a1 mRNA levels and showed a trend toward increased Col3a1 mRNA expression but did not affect Fn-1, indicating a partial protective effect. Major changes in proinflammatory gene expression were not observed (Table 4). In contrast to the changes in renal gene expression, cardiac monocyte chemoattractant protein-1, tumor necrosis factor-α and plasminogen activator inhibitor-1 mRNA abundance increased on aldo/NaCl exposure in WT but not Tg animals (Table 5), indicating a primary inflammatory response that may depend on aldo-TGF-β-T-cell cross-talk. Cardiac profibrotic gene expression showed only minor changes (Table 5).
Discussion
Background
TGF-β is known to be involved in aldo/NaCl-induced damage of renal and cardiac tissue, although the precise mechanism is not completely understood. TGF-β has the ability to inhibit T cell function and therefore reduce inflammatory events. However, TGF-β has also been shown to induce Th17 polarization of CD4+ T cells, mediating inflammatory events. Thus, TGF-β may also exert proinflammatory actions.35 Furthermore, it has been demonstrated that aldo induces Th17 polarization via enhanced TGF-β secretion.12 In the present study, we investigated whether the TGF-β responsiveness of T cells affects the aldo/NaCl-induced alterations of renal and cardiac tissue homeostasis, and, if so, whether TGF-β signaling promotes or antagonizes this effect. We addressed this question using a mouse model overexpressing a truncated TGF-β type II receptor in T cells, rendering the cells non-responsive to TGF-β. All observed effects were independent of changes in blood pressure.
Tg phenotype
In Tg animals under control conditions, the basic parameters were not different from WT animals, except for a slight but significant increase in blood glucose. As the blood glucose concentration was measured in non-starving animals and the detected amount was still in the physiological range known for this mouse strain, no further investigations were made.
Not unexpectedly, Tg animals showed enhanced interstitial fibrosis (Sirius red staining) under control conditions, most probably because of the absence of the tonic inhibitory action of TGF-β on T cells. Organ weights were not significantly affected by the genotype. These findings are in agreement with the data obtained by quantitative PCR, which demonstrated an increase in FN-1, Col1a1 and chemokine ligand-5 (CCL-5) mRNA in the kidney.
Basic physiological parameters and systolic blood pressure
In contrast to our study, the majority of studies of aldo/NaCl-induced end-organ damage have used C57BL/6 mice and performed a subtotal nephrectomy. We decided to perform the experiments without artificially reducing renal function. Thus, the difference in the genetic background and the avoided nephrectomy may account for the lack of a hypertensive effect of aldo/NaCl. There is growing evidence that the genetic background of mice is important for the development and progression of hypertension,36, 37, 38 whereas reno-cardiovascular fibrosis, for example, in the DOC/salt model, is not necessarily secondary to hypertension. In addition, the protective effect of spironolactone for renal function was not related to decreased blood pressure and instead was related to an amelioration of the inflammatory status. Similar findings were reported by Fiebeler et al.39 in a Tg rat model of hypertension We are aware of the fact that measurement of blood pressure via tail cuff is not as precise as telemetry. However, because we decided to minimize additional treatment, this approach appeared to be the appropriate method.
Interestingly, hematocrit was increased in Tg animals treated with aldo/NaCl. But, as the hematocrit is still in the physiological range known for this strain, no further investigations were made.
Organ weight and fibrosis
Aldo/NaCl treatment increased renal weight in WT and Tg animals, whereas interstitial matrix deposition increased only in WT animals. These data show (i) that aldo/NaCl might damage renal tissue independently of high blood pressure or antecedent reduction in renal mass and that (ii) the effect on renal mass seems to be independent of TGF-β-T-cell communication. Furthermore, the profibrotic effect of impaired TGF-β communication was not additive to the aldo/NaCl effect, indicating a possible common pathway. In contrast to the kidney, cardiac hypertrophy appears to depend on intact TGF-β signaling, although the profibrotic effect of impaired TGF-β communication was again not additive with the aldo/NaCl effect. Thus, under control conditions, TGF-β might prevent renal and cardiac fibrosis via interaction with T cells. This interaction is also required for the profibrotic action of aldo/NaCl.
Renal and cardiac gene expression
In agreement with the histological findings, aldo/NaCl treatment and impaired TGF-β-T-cell communication each enhanced collagen expression, whereas their effects were not additive (Table 4). Of note, renal Fn-1 mRNA expression was affected differentially in two genotypes, and TGF-β-T-cell communication appeared to be required for Fn-1 induction in the kidney. Surprisingly, CCL-5 expression was highest in the kidneys of Tg control animals. Cardiac gene expression showed a different response pattern, with plasminogen activator inhibitor-1 induction depending on TGF-β-T-cell communication. Plasminogen activator inhibitor-1 is known to, in part, mediate the profibrotic effects of aldo/NaCl.22 Thus, TGF-β-T-cell communication is required for certain, but not for all, aldo/NaCl-induced pathological changes in gene expression. However, the relative importance of this pathway seems to be organ specific.
Role of TGF-β in aldo/NaCl-induced organ damage
The data presented here do not form a conclusive picture of the precise role of TGF-β-T-cell cross-talk during aldo/NaCl-induced organ damage because they are phenomenological in nature and require further in-depth analysis. However, some conclusions can be drawn. First, impaired TGF-β responsiveness of T cells appears to exert a slight profibrotic effect, most probably due to immune cell disinhibition. These data are in line with the findings that mice Tg for the dominant-negative TGF-β-RII show enhanced lymphocyte infiltration and ‘spontaneous’ T cell activation,26 with a shift to a Th1 phenotype in the strain used in this study.28, 29, 30 In addition, TGF-β is required for the maintenance of normal T-cell quiescence.26 Second, in the context of aldo/NaCl, impaired TGF-β responsiveness does not lead to an exacerbation of the pathological changes. Thus, TGF-β does not serve as a negative feedback regulator. Third, impaired TGF-β responsiveness exerted a partial protective effect, indicating that TGF-β, in the context of aldo/NaCl, acts in part via a stimulatory modulation of the immune system and not directly on organ tissue. Cardiac hypertrophy was abolished in Tg animals, an effect that might be partially explained by diminished aldo/NaCl-induced matrix synthesis. Kidneys were less well protected, considering protein excretion and weight. These parameters were clearly independent of T cell TGF-β responsiveness. However, in the kidney, Fn-1 induction was reduced in Tg animals, and the effects on collagen were at least not additive. Thus, some pathological events within the kidney may depend on T cell TGF-β responsiveness.
In future studies analyzing the underlying mechanisms of aldo/TGF-β/T cell interaction, blood pressure should be examined via telemetry, and urine composition should be evaluated using metabolic cages.
Possible mechanisms
At present, we can only speculate on the detailed mechanisms underlying the cross-talk between aldosterone, TGF-β and T cells. It has been shown that 30% of T cells at sites of aortic fibrosis in mice treated with aldo/NaCl are CD4 and CD8 negative, although they are α/β positive.17 Such α/β-positive T cells are proinflammatory and produce interleukin-17, a potent proinflammatory cytokine involved in autoimmune disorders.17, 40 The recruitment of these T cells to the place of fibrosis and their polarization to Th17 was induced, in part, by TGF-β derived from dendritic cells because T cells do not express the MR.12 Th17 polarization makes TGF-β a stimulatory cytokine for T cells. If these events also occurred in our model, then they would explain the function of TGF-β as a partial mediator of aldo/NaCl-induced tissue damage. Future, in-depth analysis is now required to unveil the cellular and molecular mechanisms of renal and cardiac fibrosis modulated by aldo via T cells further.
References
Fiebeler A, Haller H . Participation of the mineralocorticoid receptor in cardiac and vascular remodeling. Nephron Physiol 2003; 94: 47–50.
Pitt B, Zannad F, Remme WJ, Cody R, Castaigne A, Perez A, Palensky J, Wittes J . The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med 1999; 341: 709–717.
Pitt B, Remme W, Zannad F, Neaton J, Martinez F, Roniker B, Bittman R, Hurley S, Kleiman J, Gatlin M . Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med 2003; 348: 1309–1321.
Rocha R, Martin-Berger CL, Yang P, Scherrer R, Delyani J, McMahon E . Selective aldosterone blockade prevents angiotensin II/salt-induced vascular inflammation in the rat heart. Endocrinology 2002; 143: 4828–4836.
Dorrance AM . Are macrophages the foot soldiers in the war waged by aldosterone against the heart? Hypertension 2009; 54: 451–453.
Nakamura T, Kataoka K, Fukuda M, Nako H, Tokutomi Y, Dong YF, Ichijo H, Ogawa H, Kim-Mitsuyama S . Critical role of apoptosis signal-regulating kinase 1 in aldosterone/salt aldosterone/salt-induced cardiac inflammation and fibrosis. Hypertension 2009; 54: 544–551.
Schiffrin EL . Effects of aldosterone on the vasculature. Hypertension 2006; 47: 312–318.
Young M, Funder JW . Eplerenone, but not steroid withdrawal, reverses cardiac fibrosis in deoxycorticosterone/salt-treated rats. Endocrinology 2004; 145: 3153–3157.
Farman N . Molecular and cellular determinants of mineralocorticoid selectivity. Curr Opin Nephrol Hypertens 1999; 8: 45–51.
Remuzzi G, Cattaneo D, Perico N . The aggravating mechanisms of aldosterone on kidney fibrosis. J Am Soc Nephrol 2008; 19: 1459–1462.
Fels J, Oberleithner H, Kusche-Vihrog K . Menage a trois: aldosterone, sodium and nitric oxide in vascular endothelium. Biochim Biophys Acta 2010; 1802: 1193–1202.
Herrada AA, Contreras FJ, Marini NP, Amador CA, Gonzalez PA, Cortes CM, Riedel CA, Carvajal CA, Figueroa F, Michea LF, Fardella CE, Kalergis AM . Aldosterone promotes autoimmune damage by enhancing Th17-mediated immunity. J Immunol 2010; 184: 191–202.
Rickard AJ, Funder JW, Fuller PJ, Young MJ . The role of the glucocorticoid receptor in mineralocorticoid/salt-mediated cardiac fibrosis. Endocrinology 2006; 147: 5901–5906.
Chun TY, Chander PN, Kim JW, Pratt JH, Stier Jr CT . Aldosterone, but not angiotensin II, increases profibrotic factors in kidney of adrenalectomized stroke-prone spontaneously hypertensive rats. Am J Physiol Endocrinol Metab 2008; 295: E305–E312.
Sun GP, Kohno M, Guo P, Nagai Y, Miyata K, Fan YY, Kimura S, Kiyomoto H, Ohmori K, Li DT, Abe Y, Nishiyama A . Involvements of Rho-kinase and TGF-beta pathways in aldosterone-induced renal injury. J Am Soc Nephrol 2006; 17: 2193–2201.
Rickard AJ, Morgan J, Tesch G, Funder JW, Fuller PJ, Young MJ . Deletion of mineralocorticoid receptors from macrophages protects against deoxycorticosterone/salt-induced cardiac fibrosis and increased blood pressure. Hypertension 2009; 54: 537–543.
Guzik TJ, Hoch NE, Brown KA, McCann LA, Rahman A, Dikalov S, Goronzy J, Weyand C, Harrison DG . Role of the T cell in the genesis of angiotensin II induced hypertension and vascular dysfunction. J Exp Med 2007; 204: 2449–2460.
Juknevicius I, Segal Y, Kren S, Lee R, Hostetter TH . Effect of aldosterone on renal transforming growth factor-beta. Am J Physiol Renal Physiol 2004; 286: F1059–F1062.
Lai L, Chen J, Hao CM, Lin S, Gu Y . Aldosterone promotes fibronectin production through a Smad2-dependent TGF-beta1 pathway in mesangial cells. Biochem Biophys Res Commun 2006; 348: 70–75.
Marney AM, Brown NJ . Aldosterone and end-organ damage. Clin Sci (Lond) 2007; 113: 267–278.
Sun Y, Zhang J, Zhang JQ, Ramires FJ . Local angiotensin II and transforming growth factor-beta1 in renal fibrosis of rats. Hypertension 2000; 35: 1078–1084.
Wolf G . Renal injury due to renin-angiotensin-aldosterone system activation of the transforming growth factor-beta pathway. Kidney Int 2006; 70: 1914–1919.
Derynck R, Zhang YE . Smad-dependent and Smad-independent pathways in TGF-beta family signalling. Nature 2003; 425: 577–584.
Ruiz-Ortega M, Rodriguez-Vita J, Sanchez-Lopez E, Carvajal G, Egido J . TGF-beta signaling in vascular fibrosis. Cardiovasc Res 2007; 74: 196–206.
Chun TY, Bloem LJ, Pratt JH . Aldosterone inhibits inducible nitric oxide synthase in neonatal rat cardiomyocytes. Endocrinology 2003; 144: 1712–1717.
Gorelik L, Flavell RA . Transforming growth factor-beta in T-cell biology. Nat Rev Immunol 2002; 2: 46–53.
Letterio JJ, Roberts AB . Regulation of immune responses by TGF-beta. Annu Rev Immunol 1998; 16: 137–161.
Schramm C, Protschka M, Kohler HH, Podlech J, Reddehase MJ, Schirmacher P, Galle PR, Lohse AW, Blessing M . Impairment of TGF-beta signaling in T cells increases susceptibility to experimental autoimmune hepatitis in mice. Am J Physiol Gastrointest Liver Physiol 2003; 284: G525–G535.
Schramm C, Herz U, Podlech J, Protschka M, Finotto S, Reddehase MJ, Kohler H, Galle PR, Lohse AW, Blessing M . TGF-beta regulates airway responses via T cells. J Immunol 2003; 170: 1313–1319.
Schramm C, Kriegsmann J, Protschka M, Huber S, Hansen T, Schmitt E, Galle PR, Blessing M . Susceptibility to collagen-induced arthritis is modulated by TGFbeta responsiveness of T cells. Arthritis Res Ther 2004; 6: R114–R119.
Gekle M, Volker K, Mildenberger S, Freudinger R, Shull GE, Wiemann M . NHE3 Na+/H+ exchanger supports proximal tubular protein reabsorption in vivo. Am J Physiol Renal Physiol 2004; 287: F469–F473.
Rangan GK, Tesch GH . Quantification of renal pathology by image analysis. Nephrology (Carlton ) 2007; 12: 553–558.
Raij L, Azar S, Keane W . Mesangial immune injury, hypertension, and progressive glomerular damage in Dahl rats. Kidney Int 1984; 26: 137–143.
Blum H, Beier H, Gross HJ . Improved silver staining of plant proteins, RNA and DNA in polyacrylamide gels. Electrophoresis 1987; 8: 93–99.
Dong C . Diversification of T-helper-cell lineages: finding the family root of IL-17-producing cells. Nat Rev Immunol 2006; 6: 329–333.
Hartner A, Cordasic N, Klanke B, Veelken R, Hilgers KF . Strain differences in the development of hypertension and glomerular lesions induced by deoxycorticosterone acetate salt in mice. Nephrol Dial Transplant 2003; 18: 1999–2004.
Hein L, Barsh GS, Pratt RE, Dzau VJ, Kobilka BK . Behavioural and cardiovascular effects of disrupting the angiotensin II type-2 receptor in mice. Nature 1995; 377: 744–747.
Ichiki T, Labosky PA, Shiota C, Okuyama S, Imagawa Y, Fogo A, Niimura F, Ichikawa I, Hogan BL, Inagami T . Effects on blood pressure and exploratory behaviour of mice lacking angiotensin II type-2 receptor. Nature 1995; 377: 748–750.
Fiebeler A, Schmidt F, Muller DN, Park JK, Dechend R, Bieringer M, Shagdarsuren E, Breu V, Haller H, Luft FC . Mineralocorticoid receptor affects AP-1 and nuclear factor-kappab activation in angiotensin II-induced cardiac injury. Hypertension 2001; 37: 787–793.
Umemura M, Kawabe T, Shudo K, Kidoya H, Fukui M, Asano M, Iwakura Y, Matsuzaki G, Imamura R, Suda T . Involvement of IL-17 in Fas ligand-induced inflammation. Int Immunol 2004; 16: 1099–1108.
Acknowledgements
This study was supported by the Deutsche Forschungsgemeinschaft DFG GE 905/14-1 and the Wilhelm-Roux-Programme of the Medical School, Universität Halle-Wittenberg.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Schreier, B., Rabe, S., Schneider, B. et al. Aldosterone/NaCl-induced renal and cardiac fibrosis is modulated by TGF-β responsiveness of T cells. Hypertens Res 34, 623–629 (2011). https://doi.org/10.1038/hr.2011.16
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2011.16
Keywords
This article is cited by
-
A new face among our Associate Editors
Hypertension Research (2023)
-
Synergy of epidermal growth factor (EGFR) and angiotensin II (AT1R) receptor determines composition and temporal pattern of transcriptome variation
Cellular and Molecular Life Sciences (2022)
-
miR-221 and -222 target CACNA1C and KCNJ5 leading to altered cardiac ion channel expression and current density
Cellular and Molecular Life Sciences (2020)
-
Knockout of vascular smooth muscle EGF receptor in a mouse model prevents obesity-induced vascular dysfunction and renal damage in vivo
Diabetologia (2020)
-
Iron restriction inhibits renal injury in aldosterone/salt-induced hypertensive mice
Hypertension Research (2015)
