

Key Points
- Flexible laryngoscopy reveals some unique aspects of swallowing and complements the fluoroscopy procedure.
- The fiberoptic endoscopic evaluation of swallowing (FEES) procedure is a comprehensive evaluation of the oropharyngeal phase of swallowing that can reveal the nature of the problem and guide management, improving efficacy and outcome. In addition, this technique can be used as a biofeedback tool in therapy.
- FEES is a safe, valid, and reliable procedure that can be used in patient populations, in different settings, and for different purposes.
Introduction
In 1988, the first published description of the use of flexible laryngoscopy to evaluate oropharyngeal dysphagia was published by Langmore, Schatz, and Olsen.1 The procedure, known as fiberoptic endoscopic evaluation of swallowing (FEES), was developed as a secondary procedure, to be done when videofluoroscopy was not available or convenient, such as for patients in the intensive care unit (ICU) or in a nursing home, or for patients who were extremely obese. Over the years, however, as the value of laryngoscopy has become appreciated for its unique view of the larynx, its ability to identify salient findings, and its value in guiding treatment, FEES has become a standard procedure in many swallowing disorders clinics. This review describes the FEES procedure, the findings gleaned from the exam, and its role in treatment and management of patients with dysphagia, and discusses the evidence for its validity, reliability, usefulness, and efficacy.
The Process of Normal Swallowing Viewed Endoscopically
The swallow is divided into the oral, pharyngeal, and esophageal phases, depending on where the bolus is seen. With flexible laryngoscopy, the structures in view include the nasopharynx, oropharynx, and hypopharynx, with a particularly good view of the larynx. The body and front of the tongue as well as the oral cavity are not seen. Thus, the oral stage is only partially evaluated, whereas the pharyngeal stage is the center of attention. Similarly, because laryngoscopy has only limited ability to assess upper esophageal sphincter (UES) opening and doesn't extend far into the esophagus, the esophageal phase is not assessed in the FEES examination. Transnasal endoscopy, esophagoscopy, or fluoroscopy would assume that role.
What aspects of the oropharyngeal swallow and what structural movements can be seen endoscopically versus fluoroscopically? A simultaneous endoscopic and fluoroscopic examination, shown in Video 1, highlights some of the differences.
Video 1: Normal subject swallowing as viewed from a simultaneous fluoroscopy and endoscopy study.

If you view the studies in slow motion, you will be able to correlate some movements such as epiglottal retroflexion and arytenoid anterior tilt. If you view the last swallow slowly, you will be able to appreciate the normal sequence of events as the airway closes for the swallow.
Oral Preparation of the Bolus: The Oral Preparatory Phase
When food is delivered to the mouth, oral preparation begins. The tongue moves a solid bolus from side to side as it is chewed and formed into a cohesive bolus. Pureed food and liquids are contained in the middle of the mouth. Fluoroscopy can visualize this stage nicely, whereas endoscopy can only infer what is transpiring from movements of the base of tongue. However, as sometimes happens during this oral preparatory phase, some of the bolus leaks or falls into the hypopharynx. This premature spillage is captured immediately with endoscopy as the bolus falls over the base of tongue. The endoscopist can see where the bolus falls as well as the laryngeal or pharyngeal response to this spillage.
Oral Transfer Stage
Once the oral preparatory phase has ended, the swallow begins. It used to be thought that the oral and pharyngeal stages of swallowing were clearly separated but it is now appreciated that the initiation of the swallow entails both oral and pharyngeal movements. In fact, oral preparation, oral transfer, and the initiation of the swallow may be intertwined, especially with food. Palmer et al.2, 3 has demonstrated a normal pattern of chewing and transporting masticated food to the valleculae, before the swallow is initiated. The transitional phase does not last long, however, because within a matter of seconds after "dumping" food to the valleculae, the person swallows the contents in the valleculae along with the bolus in the mouth. Pureed food may show this pattern of transport (dumping) to the valleculae, even without mastication. However, liquids have no such preswallow transport stage and are swallowed as a whole. Endoscopy captures any transport or dumping of food that occurs at the onset of the swallow. It also visualizes the head of the liquid bolus if it enters the oropharynx prior to initiation of the swallow.
Structural Movements Marking the Onset of the Swallow
Several structures move nearly simultaneously to mark the onset of the swallow, including base of tongue retraction, hyolaryngeal elevation, velopharyngeal closure, pharyngeal contraction, UES opening, and airway closure. Fluoroscopy captures many of these, whereas endoscopy captures fewer specific movements. Endoscopy does visualize velopharyngeal closure at the onset of the swallow very well if the scope is positioned within the nares. With a view of the hypopharynx (HP), the laryngoscope captures the onset of tongue base retraction, epiglottal retroflexion, and lateral pharyngeal wall squeeze, but only briefly before the view is obliterated by "whiteout." Video 2 shows several of these movements in a series of water swallows executed by a normal individual.
Video 2: Normal subject: water swallows seen endoscopically.

Note the tongue retraction and lateral pharyngeal wall medialization as the swallow develops.
With a close view of the larynx, endoscopy can also capture the laryngeal movements that comprise airway closure. Laryngeal closure for swallowing is typically described in textbooks as occurring from inferior to superior, with the vocal folds adducting first and the epiglottis covering the arytenoids and glottis last. To precisely define this important event, Van Daele et al.,4 Ohmae et al.,5 and Shaker et al.6 have all used endoscopy along with fluoroscopy, or electromyography (EMG) to determine the order of events that act to close the airway for swallowing. Although Shaker et al. found that the predominant pattern of closure was true vocal cord (TVC) adduction first (66% of the swallows), Ohmae et al. found a different predominant order of events. They found that arytenoid adduction was the first event to be observed (86% of the time) and that TVC closure was not yet achieved as the view was lost endoscopically. They assumed that glottic closure was achieved at some point in the swallow but did not have the tools to determine this. Flaherty et al.7 used magnetic resonance imaging to study the relationship of laryngeal closure and laryngeal elevation. They reported that vocal cord (VC) adduction was not complete until the peak of laryngeal elevation. Gay and colleagues8 used EMG to compare thyroarytenoid (TA) activity as well as several laryngeal elevators. They found a variable order of events.
In light of these disparate reports, Van Daele et al.4 reported on a simultaneous endoscopy and EMG study to clarify the order of events. Using four normal, healthy subjects, they placed bipolar hooked-wire electrodes on several muscles, including the TA, posterior cricoarytenoid (PCA), which is the only muscle to abduct the vocal cords, and the suprahyoid musculature. A flexible laryngoscope was then inserted to a point just above the epiglottis for half of the swallows and just above the arytenoids for half of the swallows. The subjects drank 10-mL swallows of grape juice 10 times. Two of the subjects also drank 10 mL of grape juice 10 times using the super-supraglottic swallow (hold breath tightly, then swallow). Results showed the following general order of events for a normal swallow: (1) arytenoid adduction and tilt with cessation of PCA activity (2) hyolaryngeal elevation, and (3) vocal cord closure. The authors hypothesized that the initial medialization of the arytenoids was a passive event, caused by inhibition of the PCA. Arytenoid adduction was the first movement to signal the onset of the swallow, occurring as much as 340 msec before laryngeal elevation. The vocal cords did not completely contact each other until the larynx was at least halfway to its peak elevation. In contrast, for the super-supraglottic swallows, where the subjects were voluntarily holding their breath tightly prior to swallowing, the order of events was reversed. The TA muscle was activated much earlier and caused vocal cord closure simultaneously with tight arytenoid medialization. This contraction was sustained throughout the swallow. These two patterns can be seen in Video 3.
Video 3: Normal airway closure at the onset of the swallow.
The first three swallows show normal airway closure. Note the arytenoids mark the onset of the swallow and cover the glottis before the vocal folds fully adduct. Normal airway closure at the onset of the swallow is seen if the subject holds his breath tightly before he swallows (the supra-superglottic swallow). Note the vocal folds actively adduct in this condition prior to the swallow.
These findings have tremendous clinical implications. The vocal cords do not provide the first and most important level of airway protection for swallowing, as widely presumed. Rather, it appears that the arytenoid and aryepiglottic folds closing medially and lunging forward to cover the glottis provide the most important line of defense against penetration and aspiration. A super-supraglottic swallow provides an early mode of protection, recruiting early closure of the vocal cords and "double" protection for those persons at risk for aspirating.
The Completion of the Swallow
After this brief look at the onset of the swallow, there is a period of about 0.5 to 0.6 seconds where the pharyngeal air space is obliterated by tissue contacting other tissue and the bolus passing through. The light from the distal end of the endoscope is reflected back to the eyepiece, resulting in whiteout. During this period, the hyolaryngeal complex completes its elevation, the epiglottis completely retroflexes, the pharyngeal constrictors squeeze the bolus into the open UES, and the bolus passes into the esophagus. When the swallow is over, all structures return to rest quickly and the air space reopens, yielding a view of the hypopharynx (HP) again. If the swallow has been a normal one, there will be no residue left in the HP. The bolus may never have been seen! This will not be the case for most patients with dysphagia, however, as will be described shortly.
In Figure 1, the order of events making up the swallow is depicted, showing the relative time of onset and offset and duration of key movements and muscular contractions. The period of whiteout can be appreciated in gray shadow. Most of the key movements are seen at their onset via endoscopy, but very soon the view is lost to whiteout. The chronologic order of (1) airway closure, (2) base of tongue/hyolaryngeal elevation, and (3) pharyngeal closure can be seen, although they clearly overlap.
Figure 1: Order of events in swallowing.

Timeline of order of events in swallowing as compiled from needle electromyography (EMG), endoscopy, fluoroscopy, and submental EMG. Whiteout*: time period the videoendoscopic image is obscured owing to pharyngeal closure. Genioglossal*: EMG activity in the genioglossal muscle using intramuscular hooked wire electrodes. Mylohyoid*: EMG activity in the mylohyoid muscle using intramuscular hooked wire electrodes. Geniohyoid*: EMG activity in the geniohyoid muscle using intramuscular hooked wire electrodes. Submental**: EMG activity from submental surface electrodes. Hyoid ascent***: Elevation of the hyoid from ultrasound images. Hyoid descent***: Descent of the hyoid from ultrasound images. Epiglottic movement***: Time period the epiglottis begins inversion, remains inverted, and returns to normal position as seen via videoendoscopy. Superior constrictor*,**: EMG activity in the superior constrictor muscle using intramuscular hooked wire electrodes. Longitudinal pharyngeal musculature*: EMG activity in the posterior faucial pillars using intramuscular hooked wire electrodes. Cricopharyngeal relaxation*,**: Decrease in EMG activity in the cricopharyngeus muscle using intramuscular hooked wire electrodes. Arytenoids medializing*: Time period representing the movement of the arytenoids toward the midline as seen via videoendoscopy. Arytenoids medialized*: Time period the arytenoids remain in the midline during a swallow as seen with a combination of videoendoscopy and fluoroscopy. Arytenoids tilted/vestibular closure****: Time period the arytenoids begin movement toward the base of the epiglottis and remain there resulting in vestibular closure as seen via fluoroscopy. Thyroarytenoid*,**: EMG activity in the thyroarytenoid muscle using intramuscular hooked wire electrodes. Interarytenoid**: EMG activity in the interarytenoid muscle using intramuscular hooked wire electrodes. Key: *McCulloch et al., unpublished data; **Perlman AL, Palmer PM, McCulloch TM, Van Daele DJ. Electromyographic activity from human laryngeal, pharyngeal and submental muscles during swallowing. J Appl Physiol 1999;86(5):1663 –1669. ***Perlman AL, Van Daele DJ. Simultaneous videoendoscopic and ultrasound measures of swallowing. J Med Speech Lang Pathol 1993;1(4):223 –232. ****Shaker R, Dodds WJ, Dantas RO, Hogan WJ, Arndorfer RC. Coordination of deglutitive glottic closure with oropharyngeal swallowing. Gastroenterology 1990;98:1478–1484. Note: Dashed and thin lines represent standard deviations. (Source: Langmore53 with permission from Thieme New York)
Clinical Decision Making: Which Examination Is Indicated?
Once a patient has been identified as having a suspected oropharyngeal dysphagia, the referring physician and the dysphagia specialist, usually a speech–language pathologist, need to determine which examination will be most useful. In many cases, either a modified barium swallow (MBS) or a FEES examination will be helpful in revealing the nature of the problem. Table 1 lists some of the common indications for each examination.

Some indications are logistic, such as equipment availability. Other indications are based on the nature of the suspected problem. For example, if the problem is one of foreign-body sensation localized to the suprasternal notch, the preferred examination is an MBS combined with a regular barium swallow (for a likely diagnosis of esophageal dysphagia or gastroesophageal reflux disease). If the problem is aspiration of thin liquids after surgery, the preferred examination is FEES (to look at vocal cord mobility and airway closure).
A recurrent theme of this review is that both examinations are valuable. The examiner should have both procedures available so that the appropriate one can be used with each patient. The following list describes some of the unique findings from a FEES and fluoroscopy study:
- Only fluoroscopy: visualizes bolus during height of the swallow; analyzes oral phase (esophageal phase), completeness of tongue retraction, UES opening, laryngeal elevation, extent of aspiration, submucosal changes (osteophytes, metal plates from surgery, etc.).
- Only endoscopy: visualizes secretions; directly assesses sensation; directly views surface anatomy, mucosal abnormalities (edema, erythema), effect of altered anatomy on bolus flow and airway protection, glottic closure, path of the bolus clearly, location of bolus within the hypopharynx.
The Fiberoptic Endoscopic Evaluation of Swallowing Procedure
Otolaryngologists view the HP and larynx in patients with swallowing complaints. They typically assess vocal cord mobility and airway protection, but that is the extent of the physiologic assessment for swallowing function. Their primary purpose in examining many patients is to rule out an anatomically based problem such as cancer, which is causing the dysphagia. They may infer a poor swallow in patients with excess secretions in the HP. This examination is not a FEES procedure.
The FEES protocol, as established by Langmore et al.,1 is a comprehensive evaluation of swallowing, including three major components: (1) structural movement, sensory status, and anatomic support for swallowing; (2) ability to swallow food and liquid; and (3) response to postural, dietary, or behavioral alterations to alter the path of the bolus or the way it is swallowed. The FEES exam has a similar purpose as the modified barium swallow—to identify and describe the swallow and to test some interventions to alleviate a dysphagia.
The FEES protocol, last revised in 2004, is presented in Table 2. It guides the examiner through the three phases of the examination.
Preparing for the Examination
After interviewing the patient, the examiner may choose to perform a FEES examination. Preparation for the examination includes gathering some supplies and equipment. Supplies include food and liquid, food coloring (blue or green), lubricant for the sheath of the endoscope, alcohol prep pads, spoons and straw, gloves, and, if indicated, a nasal decongestant (Figure 2).

If the patient is an outpatient or in a rehabilitation setting, the examination will likely be done in the clinic. Inpatients, and especially ICU patients, are often done at bedside. Figures 3 and 4 shows both of these settings with a FEES examination in progress. Note the position of the monitor and the method of holding the endoscope for a FEES examination. In my opinion, this "fishing pole" technique has been most successful owing to the ability of examiners to move around and to position the scope away from their face. It provides the greatest comfort and endurance for an examination that may take 15 minutes or longer to complete.
Figure 3: Inpatient FEES examination.

Setup of a FEES examination being done on an inpatient who has a tracheotomy and needs to be tested in bed. Equipment: Pentax laryngoscope, camera and light source, VCR/Mini-DV recorder and video monitor.
Figure 4: Outpatient FEES examination.

Setup of an outpatient FEES examination showing the patient and examiner viewing the monitor as the patient eats. Equipment: Pentax laryngoscope, camera and light source, VCR/Mini-DV recorder and video monitor.
The Fiberoptic Endoscopic Evaluation of Swallowing Protocol
Part I: Preswallowing Tasks
In the first phase, the examiner assesses the anatomy of the patient as it relates to support of normal swallowing, notes the status of any standing secretions, directly assesses movement of key structures, and assesses sensorimotor function within the region. All of these observations help the clinician determine the potential of the patient to execute a normal swallow, and explain any dysphagic patterns that may present.
Notes regarding anatomy. Surface anatomy within the nasopharynx, oropharynx, and hypopharynx can be viewed directly in the FEES procedure with an eye to its ability to support normal swallowing. Altered anatomy from trauma, surgery, or congenital conditions has an impact on the bolus path, ability to clear the bolus, and ability to keep it out of the nose and airway. Foreign bodies and masses are noted and referred to otolaryngology.
Status of standing secretions. The presence of excess secretions within the HP is important to note. Their consistency reveals their source and how long they have been present. Their location helps to predict the ability of the patient to swallow food and liquid. Murray et al.9 showed that the presence of excess standing secretions within the laryngeal vestibule that are not cleared spontaneously by the patient are highly predictive of aspiration of food or liquids. They indicate either a reduced sensory awareness of the secretions (and of a bolus) or reduced ability to clear the secretions (and a bolus) when a swallow is attempted.
Rating of movements. Key structural movements needed for swallowing are assessed in Part I of the FEES protocol as they are executed in nonswallow, phonatory tasks: base of tongue retraction, velopharyngeal port closure, laryngeal closure, laryngeal elevation, and pharyngeal wall medialization. Later on, when the patient is given food and liquid to eat/drink, these same movements are rated again. A preswallow assessment is needed, however, because the view during the actual swallow is fleeting. Epiglottal retroflexion is seen only during swallowing, however, and this movement needs to be identified during the swallowing portion of the examination by the examiner when reviewing the study to determine whether it occurred.
Sensory testing. In addition to assessing structural movement, the examiner assesses sensory physiology as it relates to swallowing. There are several indications throughout the FEES procedure of integrity of this function. Does the patient sense the endoscope in the throat? Does the patient sense leakage of bolus, residue, penetration, or aspiration? Finally, if desired, the examiner can directly assess the patient's response to a direct stimulus. One quick way to assess this is for the examiner to lightly touch the aryepiglottic fold or the tip of the epiglottis and ask if the patient feels it. A normal individual will have a sudden and distinct perception when touched and give a positive response or a cough. An alternative to direct touch is for the examiner to administer a formal sensory test, whereby an air pulse is delivered to the aryepiglottic region, which, at threshold, will evoke a laryngeal adductor reflex (LAR). If the FEES examination includes this formal test of the LAR, it is known as a FEES sensory test (FEESST) examination.10 It requires a flexible laryngoscope that has a second open port or an endosheath that has an open port to deliver the air pulse. It also requires a source of air that can be calibrated, such as the Sensory System produced by Kay-Pentax (Morristown, NJ).
Part II: Ability to Swallow Food and Liquid
The major part of the examination is spent directly assessing swallowing of food and liquid. Here, the protocol is not specified, as the choice is up to the examiner. Examinations have different purposes and patients require different protocols. My preference is to include a few standard swallows with almost every patient, for example, to usually include a 5-cc bolus of applesauce, a 5-mL drink of thin liquid, and a bite of cracker (about half the cracker) in most exams. This makes comparisons among patients easier when judging the presence and severity of spillage, and bolus clearance. Then, the examiner would continue with whatever consistency and bolus size of foods and liquids were appropriate to assess or were reported by the patient to be problematic. It is recommended that outpatients bring in their own food to test, and that the lunch tray be used to assess swallowing with inpatients. At the end of the examination, if there has been any question of presence of aspiration with liquids, the patient should be given one final liquid bolus of milk or a liquid with barium powder mixed in it. This is done because barium coats the mucosa well and leaves behind a trace of its path. If the patient has aspirated, evidence of it is seen clearly on the subglottic shelf and in the laryngeal vestibule.
As an outcome of a FEES examination, the examiner formulates an accurate impression and makes realistic recommendations. Thus, it is important that the examiner understand how the patient eats in real life. One way to determine this is to devote part of the testing session to having the patient self-feed with no instructions as to bolus size, rate of eating, and when to swallow. If there is residue left after the swallow in the HP, the examiner should not tell the patient to swallow a second time, but rather should ask if the food is gone, noting the patient's sensitivity. The patient is allowed to take further food to see if the residue accumulates and how the patient handles it.
Therapeutic Interventions
When examiners have a good idea of the nature of the problem, they can then begin to intervene with a variety of appropriate strategies. Understanding the nature of the problem leads the examiner to the rational use of the best strategy, but there is some trial and error involved as well. One great advantage of the FEES examination is the extended time available to test any of a number of different postures, bolus consistencies and sizes, delivery methods, or behavioral changes. The examiner may ask the patient to dry swallow or take a liquid wash to see its effect on reducing residue. The patient may be taught a new way of swallowing, using the image on the monitor as biofeedback. He may be taught a breath-hold maneuver in which the VCs are tightly shut prior to the swallow. The patient may be taught a controlled swallow in which the liquid is contained in the mouth for 1 or 2 seconds before it is let go to initiate the swallow. The following list illustrates some of the possible compensatory and rehabilitative techniques that can be taught to patients during this initial FEES evaluation:
1. Examples of compensatory techniques
- Modify bolus volume, consistency, viscosity
- Change method of food/liquid delivery
- Modify sequence of delivery
- Change rate of food/liquid delivery
- Alter behavior (e.g., dry/ clearing swallows, postural changes)
2. Examples of rehabilitative techniques
- Swallow maneuvers (supraglottic swallow; effortful swallow)
- Exercises (to increase strength of muscle groups)
- Sensory stimulation techniques (thermal-tactile stimulation; low-level electrical stimulation)
Abnormal Findings from the Fiberoptic Endoscopic Evaluation of Swallowing Procedure
Much information from a FEES examination can be identified as the examination proceeds. The bolus can be seen spilling into the hypopharynx prior to the swallow, residue can be seen after the swallow, and the response of the patient to material in the laryngeal vestibule can be appreciated. However, a more meaningful interpretation usually requires the examiner to analyze the study afterward by replaying the recorded study. Abnormal findings from part I of the FEES examination help to explain the dysphagia. In part II, four major types of dysphagic patterns typically occur: (1) inability to prepare the food orally, (2) inability to initiate the swallow in a timely and coordinated manner, (3) inadequate airway protection or velopharyngeal (VP) closure during the swallow, and (4) incomplete bolus clearance. These problems can all be demonstrated on a FEES examination, although oral-stage problems are also dependent on clinical observations of the patient.
Abnormal Part I Findings
The variety of anatomic or physiologic problems that may be seen in a FEES exam is endless. An experienced examiner is more likely to detect subtle abnormalities that may be missed by the novice. They are important because they not only explain the dysphagia, but also provide a rationale for the treatment plan. Some of this information is also identified during swallowing, and this redundancy is valuable. For example, a sluggish laryngeal closure maneuver will likely be reflected in a delayed initiation of the swallow. Excess secretions in the laryngeal vestibule that are not sensed by the patient are likely to be associated with aspiration of food or liquid.9 Reduced pharyngeal squeeze puts a patient at higher risk for aspirating food.11
Recent research has highlighted the potential benefit of sensory testing, done as part of the FEESST examination. Severely reduced or absent sensation in the laryngopharynx was found to be significantly associated with aspiration of liquids in one study,12 and it may also be highly associated with laryngopharyngeal reflux.13 The reliability of elicitation of the LAR, as described in the original protocol, has been questioned by some researchers,14 but the contribution of the LAR to swallowing integrity is well accepted.
Figure 5 illustrates some examples of abnormal findings from a FEES examination that would be considered part I findings because they are seen before any food or liquid is given to the patient.
Figure 5: Photographs of part I findings.
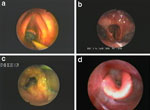
a: Intubation trauma. Note irregular mucosa at posterior commissure. b: Resected epiglottis. c: Feeding tube directed down airway. d: Edema and excess thick secretions post–radiation therapy.
Abnormal Part II Findings
Once patients begin to eat and drink, their "dysphagia profile" emerges. The four most common patterns, seen in patients with dysphagia secondary to any underlying pathology, are as follows:
1. Reduced ability to prepare the food orally. Problems in the oral stage are identified from a combination of clinical observation of the patient eating, oral motor examination, and interview. Rate of eating, bolus size taken, masticatory pattern, and time taken to masticate are all readily apparent. The FEES examination can also identify the pharyngeal consequences of an oral-stage problem. For example, food or liquid may leak into the HP prematurely or poorly masticated food may be left behind in the HP as residue after the swallow. The examiner must be aware that it is normal for food to be transported to the valleculae during the masticatory phase for a variable length of time prior to swallowing it, but it is unusual for it to fall lower in the pharynx and certainly will not penetrate the laryngeal vestibule.15
2. Inability to initiate the swallow in a timely and coordinated manner. Problems at the onset of the swallow are extremely common in patients with neurologic disorders. The demented patient may eat compulsively without giving the pharyngeal and laryngeal structures time to prepare for the swallow. Alternatively, the patient may have difficulty initiating the swallow and hold the bolus in the mouth for an excessive amount of time. Patients with Parkinson's disease sometimes manifest a tongue-pumping pattern in which they struggle to initiate the swallow. The most serious consequence of any of these deficits is that the bolus spills into the larynx before the airway has closed and the bolus is aspirated. The FEES procedure can visualize this problem directly because whiteout has not yet obliterated the view.
Pharyngeal delay is a temporal measure that has been used to quantify this problem. It is a measure of how long the bolus is in the pharynx before the swallow begins. This time can be readily calculated from endoscopy as well as fluoroscopy. Research has established that some spillage is normal, especially with solid food or when specific instructions are not given to "swallow now."3, 15 As a result, the cutoff for normal versus pharyngeal delay has become clouded. More research needs to be done, using different conditions (e.g., measured bolus size and instructions to swallow vs. casual eating) and with different age groups. For the present, rather than focusing solely on a temporal measure of delay, the examiner should appreciate all the factors that allow one person to aspirate more easily than another. The length of time the bolus is in the pharynx, combined with how low the bolus spills, the bolus size, and the significant influence of anatomy on directing the path of the bolus, will cumulatively determine whether a person will run into trouble at the initiation of the swallow. Although it is not uncommon for a bolus to spill into the pharynx before the swallow begins, it is not normal for every bolus to spill to the pyriforms or for a bolus to sit in the pharynx for several (5+) seconds. If the sensory system is intact, including its connections to higher cortical centers, the swallow will always be triggered when the bolus touches the laryngeal rim, and thus penetration will be rare and aspiration will be prevented. Finally, it goes without saying that this problem is more likely to occur with liquids than food, simply because liquids flow faster and are more likely to spill into the laryngeal vestibule if the system is sluggish to respond to the presence of a bolus in the hypopharynx.
Video 4 show two examples of mistimed initiation of the swallow, resulting in aspiration.
Video 4: Aspiration before the swallow.
a: The first clip shows a patient as had his epiglottis resected. He is taking his first liquid bolus after surgery. The initiation of the swallow appears delayed. Because the vallecular pocket has been eliminated by removal of the epiglottis, the small amount of liquid given to him spills directly into the laryngeal vestibule before the swallow is triggered. b: The second clip shows a patient after a stroke who is not timing the onset of the swallow the bolus flow. He directs the bolus into his pharynx a few seconds before initiating the swallow and the bolus falls directly into the laryngeal vestibule.
3. Inadequate airway protection and velopharyngeal valving during the swallow. Inadequate laryngeal or velopharyngeal valving results in misdirection of the bolus. Of these valves, the laryngeal valve is most critical, because it can lead to aspiration of material during the swallow. The underlying pathophysiology may be weakness or incomplete closure of the laryngeal structures (epiglottic retroversion, arytenoids covering the glottis, and vocal fold adduction). Sometimes, however, the problem lies with mistiming the bolus flow with airway closure or with delayed laryngeal elevation, which facilitates airway closure. This problem is really an extension of the previously described problem of delayed or mistimed initiation of the swallow.
To sort this out, the results from part I of the FEES examination should be referenced. In this preswallow part of the exam, adequacy of glottic closure at the level of the true vocal folds was directly assessed. In addition, the briskness of laryngeal movements was appreciated, giving the examiner an idea of response time to bolus spillage.
Penetration or aspiration of the bolus during the height of the swallow is unlikely to be directly viewed during a FEES examination because of whiteout. Evidence of penetration or aspiration will need to be seen by residue of bolus in the laryngeal vestibule, on the vocal folds, or below the glottis on the subglottic shelf. Because liquids are most likely to leak into the laryngeal vestibule, it is imperative that a liquid that leaves residue be used during the examination. Barium coats the mucosa well and can be used for this test.
Video 5 shows an example of aspiration during the swallow. The bolus used is barium and it is clearly seen subglottally after the swallow.
Video 5: Aspiration during the swallow in a patient with dysphagia.

This patient has reduced ability to clear the bolus through the hypopharynx (HP) and to close the laryngeal vestibule completely during the swallow. He aspirates barium liquid and has no overt response to the aspiration (silent aspiration).
In addition to laryngeal valving, velopharyngeal valving keeps the bolus from flowing to the nasopharynx and into the nasal passages. This sphincter can be directly assessed during the swallow by withdrawing the tip of the endoscope to the nasal passage and viewing the VP port during the swallow. A photo of this view is seen in Figure 6.
4. Incomplete bolus clearance. A common type of problem in patients with oropharyngeal dysphagia is incomplete bolus propulsion, evidenced by residue of bolus left behind after the swallow. If the residue is sufficient or if it is not cleared and builds up with subsequent bolus swallows, it eventually leaks into the laryngeal vestibule and is aspirated. This is especially apt to occur at the onset of a new swallow, as the larynx begins to elevate and the pharyngeal walls begin to contract. It is also more likely to be a problem with solid food than with liquids, and with sticky food or small bits of food that can get stuck in the crevices of the pharynx. Liquids can pool in recesses but otherwise fall to the distal pharynx simply by gravity.
The cause of incomplete bolus clearance might be insufficient muscular contraction—base of tongue, pharyngeal walls—to move the bolus caudally to the open UES or insufficient laryngeal elevation, which decreases UES opening diameter. Alternatively, the cause can be anatomically based, with an obstruction to bolus flow caused by the presence of a foreign body or an anatomically resected or reconstructed structure. The excellent view of surface anatomy in a FEES examination should reveal any anatomically based problem.
The presence of residue, the patient's reaction to the residue, and the path it eventually takes are clearly seen by endoscopy. If the problem is underlying weakness, identifying the specific source of weakness is sometimes difficult and requires some analysis. Fortunately, the location of the residue points to the source of the problem. For example, if residue is left on the base of tongue, one can assume this region was not squeezed completely against the posterior pharyngeal wall. Research using simultaneous manometry and fluoroscopy has supported the relationship between location of residue and source of the problem.16, 17, 18, 19
Video 6 shows an example of aspiration after the swallow in a patient who cannot clear the bolus through the HP during the swallow and aspirates as he reopens the airway.
Video 6: Aspiration after the swallow.

This clip shows a patient post-radiation therapy for head and neck cancer who has severely reduced ability to drive and clear the bolus through the HP. As the airway opens up, he aspirates the residue.
Use of Fiberoptic Endoscopic Evaluation of Swallowing to Manage Patient with Dysphagia
In addition to being an excellent diagnostic tool, FEES has distinct advantages when it comes to management of patients with dysphagia. During the FEES evaluation, interventions are trialed for their potential benefit and the results are seen immediately. Reevaluations can be done as often as needed at the convenience of the examiner to monitor progress, to assess the continued benefit of an intervention, or to guide a dietary change. Patients who are transitioning from NPO (nothing by mouth) to PO status (or vice versa) can be monitored regularly with serial FEES exams.20 After the examination, the recorded study can be used to educate patients about the nature of their problem. The added presence of family members, nurses, or referring physicians facilitates better understanding of the swallowing problem, joint decision making, and better compliance with recommendations.
Flexible laryngoscopy can also be used directly as a treatment tool, separate from the evaluation process. With patients scoped and facing the monitor during the treatment session, the visual image provides direct on-line feedback to them about their swallowing behavior or their ability to move laryngeal, pharyngeal, or base of tongue muscles. It can also be used to increase their awareness of residue, spillage, penetration, or aspiration. The value of biofeedback cannot be underestimated, as it is an excellent tool for learning motor behaviors. Denk and Kaider21 found that when endoscopy was used with head and neck cancer patients to teach them swallow strategies, they progressed faster than the patients who did not have the benefit of endoscopic biofeedback.
This author has found endoscopy extremely useful to teach patients some exercises to strengthen the muscles used in swallowing. A set of exercises using base of tongue, laryngeal, and pharyngeal muscles are routinely taught to patients, using endoscopy as biofeedback to ensure that the patient is performing the exercises accurately. In addition, new swallowing behaviors such as using a controlled swallow or a super-supraglottic swallow can be taught more efficiently using endoscopy as biofeedback. Video 7 illustrates such a biofeedback session.
Video 7: Exercises and biofeedback with endoscopy.
Patient performing tongue, laryngeal, and pharyngeal exercises, using endoscopy as biofeedback to monitor his movements.
Establishing the Safety, Validity, Usefulness, and Efficacy of the Fiberoptic Endoscopic Evaluation of Swallowing Procedure
For an assessment tool to survive and become an established part of clinical practice, it needs to meet certain criteria. It needs to be safe, valid, reliable, useful, and efficacious. Research over the past 15 years has shown that the FEES procedure does meet these criteria.
Safety
When FEES was initiated, there were legitimate concerns about its safety. Although otolaryngologists had done flexible laryngoscopy for years, the fact that speech–language pathologists, who were not trained to provide emergency medical care, were being trained to assume the role of the endoscopist was of concern to some people. Also, the dysphagia patient population included some very fragile, unstable elderly patients in settings such as the ICU, as well as young children and even infants. The need for topical anesthesia was questioned. All of these concerns have largely been put to rest. The examination is done with necessary medical backup and in a protected medical environment. When the need for topical anesthesia arises, qualified medical personnel apply it.
In four studies specifically looking at safety, the rate of complications was less than 1%.22, 23, 24, 25 Moreover, none of the complications was serious. The most common complications were epistaxis and vasovagal response. Therefore, the conclusion is that FEES is a safe examination in any medical setting, with any of the populations reported to date.
There have been some concerns raised about the possibility of a speech–language pathologist missing a cancer within the structures viewed. That is indeed possible, but the purpose of this examination is not to identify medical pathology but to study the person's ability to swallow. If the question of cancer is raised, the patient needs a flexible laryngoscopic examination performed by an otolaryngologist. Alternatively, the otolaryngologist may choose to view recorded FEES studies and screen for that possibility. The roles of the otolaryngologist and speech pathologist in performing or interpreting FEES need to be worked out at the local level. Although national associations may not always agree, individual speech pathologists and otolaryngologists continue to work together, generally in a collegial relationship and in support of one other.
Validity
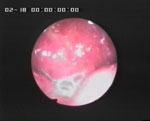
Does FEES accurately identify abnormal swallow events? How sensitive is this procedure? When FEES was first done, it was compared to the standard procedure for oropharyngeal dysphagia, which was the modified barium swallow study, using fluoroscopy. Langmore et al.23 performed both examinations on 21 persons. They tabulated the presence of four salient findings related to the bolus (aspiration, penetration, spillage, residue) on each patient's examination from both the FEES and the MBS study. Results showed a very acceptable level of sensitivity (0.88 or greater), specificity (0.50 or greater), positive predictive value (0.69 or greater), and negative predictive value (0.63 or greater) for FEES as compared to the results of the MBS study done on the same persons. Since that initial study, at least eight other research groups have compared similar findings from the two examinations.19, 24, 25, 26, 27, 28, 29, 30 Most of these studies have concluded that FEES and fluoroscopy have a high level of agreement, especially when it comes to detecting aspiration. None of the studies, however, has compared findings using both tools simultaneously. This would be the best test of higher sensitivity and specificity. This study begs to be done. Our own series of simultaneous studies suggests that each tool misses some findings with regard to location of the bolus, and that FEES is particularly sensitive at discriminating laryngeal penetration as opposed to pharyngeal residue. This is illustrated in Figure 7 where the same view of residue is seen via endoscopy and fluoroscopy after a bolus swallow in a neurologically impaired patient.
Figure 7: Sensitivity of FEES to penetration vs. residue.

Simultaneous study showing penetration vs. residue from two perspectives. a: Fluoroscopy view showing location of bolus. b: Endoscopy view showing location of bolus.
As a result of the high reported level of agreement between the two examinations, the use of the term gold standard to refer to the MBS study has been challenged by three researchers.31, 32, 33 They concluded that neither one of these examinations represents the "truth" and each one provides a valid assessment. However, when either one of the instrumental examinations is compared to a clinical, noninstrumental examination, then the instrumental examination can rightfully be called the gold standard because it is clear that instrumentation adds sensitivity and specificity to the assessment.
Although the presence of spillage, residue, penetration, and aspiration is visualized with either tool, there are many other findings that are important for the examiner to identify. Research studies comparing the value or sensitivity of FEES versus fluoroscopy to identify these other findings are limited.28 Table 2 lists some other findings that are unique to fluoroscopy and endoscopy. Clearly, both examinations are valuable.
Standardization of the Protocol and Scoring System
One way to strengthen the validity, reliability, and usefulness of an examination is to standardize the protocol and scoring of results. This enables clinicians and researchers to use a common language when describing the findings of the exam or the severity and nature of dysphagia in a particular patient. The FEES protocol was standardized by Langmore in 1988, and soon after it was copyright protected. This copyright has now expired, but the protocol is still in wide usage. The protocol is seen in Table 2. The scoring of a FEES examination has not yet been standardized and neither has the MBS study.
Reliability
High interjudge and intrajudge reliability is an important step in standardizing an examination and partly reflects the ease with which the test can be scored. Reliability has been established for two parameters of swallowing that can be scored from an MBS study: the Penetration-Aspiration Scale (PAS)34 and the swallow efficiency ratio.35 The PAS has also been submitted to reliability testing from a FEES examination36 and found to have a similar level of reliability as it did when applied to an MBS study. No other parameters of a FEES examination have been submitted to reliability testing. This would be a useful project and significant contribution to the field.
There is much work to be done in the area of standardization, validity, and reliability testing for both the MBS and FEES procedures. The lack of data in this regard is startling. Our field has not even come to agreement about what should define mild, moderate, or severe dysphagia, much less judging the normality of certain parameters such as spillage of bolus prior to initiation of the swallow.
Utility
How useful is FEES? Several studies have described its usefulness with different types of patient populations, including spinal cord injury,37, brain injury,38, 39 stroke,40, 41, pediatrics,45, 46, 47, 48, 49 developmental disability,42 head and neck cancer,43, 44 and amyotrophic lateral sclerosis,45, 46 It has been beneficial in different settings, including the ICU,47 with postsurgical patients,48, 49 in a rehabilitation hospital,50 and in long-term care.51 It has been described not only as a diagnostic tool, but also to guide treatment, specifically to transition a patient from NPO to PO feeding status20, 21 and as a biofeedback tool to guide treatment.21
Efficacy
The final test of a new procedure is to determine its efficacy, or its ability to produce favorable outcomes. For patients with dysphagia, that means being able to eat a greater variety of foods and liquid, to maintain nutrition and hydration, and to prevent pulmonary complications. The studies above described good outcomes with patients when FEES was used to guide their treatment. Similar reports have been published using fluoroscopy or a clinical examination to guide treatment. However, there has only been one study to date that has directly compared the ability of the MBS versus the FEES (or FEESST) procedure to yield favorable outcomes in patients. Aviv52 did this in his study in which 126 outpatients with dysphagia were given either an MBS or a FEESST test. The results of the test guided their dietary and behavioral management. The patients were followed for 1 year. At this time, the incidence of pneumonia in the two groups was 18% after an MBS and 12% after the FEESST. These rates were not significantly different. The conclusion was that the two examinations were similar in their ability to guide treatment and prevent pneumonia.
Conclusion
The FEES procedure has taken advantage of a marvelous tool, the flexible endoscope, to visualize the pharyngeal and laryngeal structures intimately involved in swallowing. It has proven to be a valid, useful, cost-effective, reliable, and effective procedure for diagnosing dysphagia, for understanding the nature of the swallowing problem, and for guiding treatment. It has become a standard procedure that has enhanced the skills of many clinicians who now have a multitude of tools with which to practice. It has led to research that has uncovered some unique insights about normal and disordered swallowing.
There is much research still left to be done. Some immediate gaps that beg to be studied include standardization of the FEES protocol, reliability testing, comparison of findings to fluoroscopy when the two tools are used simultaneously, a better understanding of laryngeal function and aspiration during the swallow, a clinical trial that compares outcomes of patients who are given FEES versus another examination to guide their management, compliance of patients who are given a FEES examination to guide treatment, and ability of patients to learn and perform exercises when endoscopy is used in a biofeedback mode. The field of swallowing and swallowing disorders is an exciting one and endoscopy has opened more doors to the researcher and clinician alike.
