
Abstract
Purpose
Globally, 153 million people are visually impaired from uncorrected refractive error. The aim of this research was to verify a method whereby autorefractors could be used by non-specialist health-workers to prescribe spectacles, which used a small stock of preformed lenses that fit frames with standardised apertures. These spectacles were named S-Glasses (Smart Glasses).
Patients and methods
This prospective, single-cohort exploratory study enrolled 53 patients with 94 eligible eyes having uncorrected vision of 6/18 or worse. Eyes with best-corrected vision worse than 6/12 were excluded. An autorefractor was used to obtain refractions, which were adjusted so that eyes with astigmatism less than 2.00 dioptres (D) received spherical equivalent lenses, and eyes with more astigmatism received toric lenses with a 2.50 D cylindrical element set at one of four meridians. The primary outcome was to compare S-Glasses vision with the WHO definition of visual impairment (6/18). Where astigmatism was 2.00 D or greater, comparison with spherical equivalent was made. Mixed-model analysis with repeated effect was used to account for possible correlation between the vision of fellow eyes of the same individual.
Results
S-Glasses corrected 100% of eyes with astigmatism less than 3.00 D and 69% of eyes with astigmatism of 3.00 D or greater. Spherical equivalent lenses corrected 25% of eyes with astigmatism of 2.00−2.99 D and 11% with astigmatism of at least 3.00 D.
Discussion
S-Glasses could be beneficial to resource-poor populations without trained refractionists. This novel approach, using approximate toric lenses, results in superior vision for astigmatic patients compared with the practice of providing spherical equivalent alone.
Similar content being viewed by others

Introduction
Globally, refractive error is responsible for visual impairment in 153 million people, 8.5 million of whom are blind; the distribution of corrective spectacles would help to address this problem.1 A new method is proposed by the authors, whereby an autorefractor and a small stock of preformed lenses could be used by non-specialist healthcare workers to adequately correct vision, thereby minimising the need for trained refractionists and spectacle glazing laboratories. The required stock of lenses is kept small by using spherical lenses to correct all patients with astigmatism less than 2.00 dioptres (D), and toric lenses, incorporating a 2.50 D cylinder set at one of the four predetermined meridians, for all patients with astigmatism of 2.00 D or more. It was decided to call spectacles produced by this prescription method S-Glasses (Smart Glasses).
This study was planned as an exploratory study to test the proposed system by measuring the vision achieved by patients, while wearing S-Glasses in the consulting room of an Irish community ophthalmology clinic located in Dublin.
Materials and methods
Study design
This was a prospective, single-group exploratory intervention study, with paired pre- and post-correction comparisons of outcome measures. Because of its pilot nature, no sample size calculations were necessary a priori; however, a post-hoc assessment of the statistical power of the significant comparisons was performed, as appropriate.
Patients
The clinic’s electronic patient record database was searched for all astigmatic patients who had been dispensed spectacles with cylinders greater than 2.00 D, and an alphabetical list was generated; 2.00 D was chosen because it is known that astigmatism of this level causes visual acuity of ∼6/18.2 The first 100 patients on the list were invited to participate. Thirty patients who responded met the inclusion criteria, and were enrolled. A further 23 consecutive patients, with various refractive errors, were invited to participate as they presented to the clinic, and a total number of 53 patients were enrolled in the study.
Inclusion/exclusion criteria
The inclusion criteria were adult patients (aged >18 years) with uncorrected vision worse than 6/18 in both eyes who were capable of giving informed consent. The exclusion criterion was a best-corrected visual acuity worse than 6/12 and this was applied to individual eyes. Therefore, some patients were included in the analysis with one eye only. A total of 53 patients met the inclusion criteria and 12 individual eyes were excluded. There were 94 eyes tested with S-Glasses in total.
Intervention
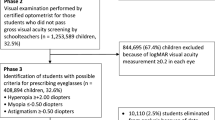
A Topcon KR8000P (Tokyo, Japan) autorefractor was used to measure the objective refraction for each patient. Refractions were recorded in minus cylinder notation and the S-Glasses algorithm was applied to these readings. Corrective lenses were presented to the patient using a Topcon phoropter, and the vision using the S-Glasses correction was recorded for each eye. The algorithm for prescribing S-Glasses is described in Figure 1.

Description of S-Glasses algorithm.
The vision in all eyes with astigmatism of 2.00 D or greater was also recorded using a spherical equivalent of the objective refraction. Then the vision achieved using the precise objective refraction measured by the autorefractor was recorded. Finally, a subjective refraction was conducted by an optometrist and the best corrected visual acuity was recorded.
Outcomes
The primary outcome was to assess and compare the vision achievable using S-Glasses against the World Health Organisation (WHO) definition of visual impairment, that is, a vision of 6/18 or worse. The secondary outcomes were to evaluate, by stratified analysis, the extent to which vision was corrected by S-Glasses and to compare this vision with: (1) uncorrected vision, (2) visual acuity achievable with just a spherical equivalent correction in the cases where astigmatism was greater than 2.00D, (3) visual acuity achievable using the autorefractor refraction and (4) best corrected visual acuity. All acuities were measured using a projected Snellen acuity chart to the nearest letter and converted to LogMAR units for analysis. For ease of reading, results are reported in this paper using the Snellen notation to the nearest letter. Where two methods of correction are compared, the difference in vision is expressed in lines, and a line is defined by 0.1 LogMAR units.
Statistical analysis
Ninety-four eyes of 53 patients were included and eyes were analysed in three groups according to the level of astigmatism; low astigmatism was defined as smaller than 2.00 D, while moderate astigmatism was between 2.00 and 2.99 D, and high astigmatism was 3.00 D or more. As some of the patients participated with only one eligible eye, while others entered the analysis with both eyes, the mean values for comparative purposes were obtained by mixed models (see below), which allowed for possible interaction among fellow eyes of the same individual. Furthermore, nine patients were members of both the high astigmatism and moderate astigmatism groups by virtue of anisometropia, and this is why the sum of the numbers of patients in each group exceeds the total number of patients in the entire study.
Descriptive statistics, with computation of the standard deviation (SD) and 95% confidence intervals (CIs) as well as the test of Shapiro-Wilk for normality of distributions were applied. Frequency distribution methods, parametric, and nonparametric tests for one-sample comparisons as well as paired, within-group comparisons were used. Paired parametric (Pearson) and nonparametric (Spearman’s rho) correlation coefficients were also computed, as appropriate. For the secondary outcomes, mixed models, with a repeated effect for the comparison between the methods, were used to obtain restricted maximum likelihood solutions with a compound symmetry of the covariance structures for all eyes as well as in the three subgroups. Least square means with 95% CIs were obtained and a post-hoc Tukey−Kramer adjustment for multiple comparisons of the P-values was done. The statistical significance of the results was assumed at P<0.05, unless stated otherwise. All analyses were performed with the statistical software PASW Statistics Ver.18 (IBM Corporation, Armonk, NY, USA) and SAS Ver.9.3 (SAS Institute Inc. Cary, NC, USA) as licensed to the Royal College of Surgeons in Ireland. All data and results are available in LogMAR units upon request.
Ethics and consent
Ethical approval was obtained by the Royal College of Surgeons in Ireland Ethics Committee, and all participants provided informed consent. We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during this research.
Results
The patients (n=53), of whom 32 were female and 21 were male, had a mean age of 60 (SD 19) years. Their spherical refractive errors ranged from −9.25 to +7.50 D and cylindrical errors ranged from 0.00 to −6.50 D (n=94 eyes).
Every eye in the low astigmatism group (<2.00 D) (n=34) achieved a vision better than 6/18 (Table 1). The mean vision in this group was less than one line worse than the mean best-corrected visual acuity and this difference was not statistically significant (P>0.05).
In the moderate astigmatism group (2.00–2.99 D) (n=24), 100% of eyes also corrected to better than 6/18 using S-Glasses, and the mean vision was 1 line worse than the best corrected acuity, which was not statistically significant (P>0.05). However, when these eyes were corrected with a spherical equivalent lens only 25% corrected better than 6/18 and the mean vision was significantly worse, by 4 lines, than the best corrected visual acuity (P<0.0001).
In the high astigmatism (>3.00 D) (n=36) group, the mean vision using S-Glasses was 2.6 lines worse than best corrected visual acuity, which was of marginal statistical significance (P=0.0633) and 69% of eyes had vision better than 6/18, with 80% of individuals having at least one eye, which could see better than 6/18. However, using the spherical equivalent correction, the mean vision was 5.5 lines worse than best corrected vision (P<0.0001) and only 11% of the eyes corrected better than 6/18, with 13% of individuals having at least one eye, which had vision better than 6/18.
The vision achievable using the autorefractor-measured correction was similar to best corrected vision. The mean vision was less than one line worse than the best corrected acuity, and this difference was not statistically significant. Across all eyes, the vision achievable using the autorefractor correction strongly correlated with the best corrected vision (n=94 eyes, Rho=0.842, Ptwo-tailed<0.01).
Discussion
Almost 90% of the blind and visually-impaired people in the world live in poor and middle-income countries without full access to eye care. This is recognised by the WHO and the International Agency for the Prevention of Blindness (IAPB) in their Vision 2020 quest for the prevention of avoidable blindness by the year 2020.3, 4
It was clearly stated that in 2006 , in order to meet Vision 2020s target, it was time to ‘act boldly’ and that ‘politicians, policy makers, primary care providers and eye specialists need to work together to develop simple, creative methods to combat vision impairment caused by uncorrected refractive error’.5 Since then, there have been very few ideas published in the literature, which aim to address some of the main causes of this problem, namely a lack of access to suitably-trained refractionists and the prohibitive cost of corrective spectacles.6, 7 To our knowledge, there have been no studies published, which aim to evaluate a method for dispensing glasses whereby there is no need for trained refractionists. This is despite the evidence that refractions measured by autorefractors can correct vision close to the subjective refractions measured by trained refractionists.8, 9 There have been some studies evaluating inexpensive ready-made glasses with spherical lenses, but the problem of astigmatism or anisometropia has been found to diminish the effectiveness of ready-made glasses, and these problems have not been addressed.10, 11, 12 It is also common for donated second hand glasses to be recycled for use by people suffering from uncorrected refractive error, however, some recently published articles criticise this approach.13, 14
The advantage of the S-Glasses algorithm (Figure 1) is that only a relatively small, finite number of individual lenses can be prescribed. Further, as the spectacle frames all have a standard-shaped aperture that is symmetrical about the horizontal axis, there would only be a relatively small stock of preformed and shaped lenses, which could be used to assemble ‘off the shelf’ glasses (Figures 2 and 3). Taken together, this means that a non-specialist health care worker could carry a small stock of S-Glasses lenses and frames, and could dispense the glasses without the need for a spectacle glazing laboratory. It is known that the cost price of good quality spectacles can be low, and the authors anticipate that the cost of the components required to assemble S-Glasses would be considerably less than $3.00 per pair, making them relatively affordable in resource-poor regions of the world.15, 16 The cost of an autorefractor is not insignificant, however, it is anticipated that using autorefractors, rather than training refractionists, is a simpler and more scalable way to refract large numbers of patients. Furthermore, there are portable, battery operated, hand-held autorefractors, which could be used in remote populations.

S-Glasses frames could be designed in various sizes, styles, and colours, but all frames would have a standard-sized lens aperture, which would be symmetrical about the horizontal axis so that the one lens shape fits all spectacles.

An illustration of how toric lenses can fit either side when the frame aperture is symmetrical about the horizontal axis. This reduces the required stock of toric lenses by half to four lenses for each spherical power.
The method for prescribing and dispensing glasses described in this study could be of great benefit to patients presenting with visual impairment due to uncorrected refractive error in regions of the world, where there is limited access to trained refractionists or spectacle glazing laboratories. Our results indicate that S-Glasses can significantly correct visual impairment, including that due to astigmatism.
All people with mild to moderate astigmatism (<3.00 D), which represents the vast majority of individuals, can be corrected to a vision of least 6/18.17 Furthermore, most of those with severe astigmatism (3.00 D or greater) can also be corrected. This novel approach, using a compromised cylindrical corrective element set at a compromised axis, results in a much improved visual acuity for patients with astigmatism than the practice of providing a spherical equivalent alone. These results demonstrate that a spherical equivalent correction is not appropriate for patients with astigmatism greater than 2.00 D.
Furthermore, a system whereby a network of non-specialist healthcare workers, who were trained to dispense S-Glasses, could act as a screening and referral mechanism for patients with low vision due to ocular pathology or extreme refractive error, which would require more specialised care. Thus, the model proposed by this paper could be included as part of an integrated eye healthcare system in each country’s National Programme and Plan of Action as envisaged by the IAPB and WHO in the Vision 2020 project.
There were some limitations to this study. The use of Snellen acuity was not ideal and it would have been better to use LogMAR ETDRS vision charts. It was also not possible to measure whether aesthenopia would be a problem with S-Glasses. The results reached were of statistical significance, however, it is acknowledged by the authors that the overall number of patients included in the study was relatively small.
It is interesting that the vision achievable using the refraction from the autorefractor was found to be nearly equivalent to the subjective refraction measured by a qualified optometrist in this study. This, potentially, has considerable implications for eye health services in regions where there are shortages of trained refractionists. The next step in the project will be to test S-Glasses in the field by comparing them to custom-made glasses in a randomised controlled clinical trial in a suitable population currently without access to glasses. Outcomes such as vision-related quality of life and spectacle intolerance due to aesthenopia will be measured.

References
Resnikoff S, Pascolini D, Mariotti SP, Pokharel GP . Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bull World Health Organ 2008; 86 (1): 63–70.
Agarwal S, Agarwal A, Apple DJ . Textbook of Ophthalmology, Vol 2 Japee Medical Publishers: New Delhi, India, 2002.
World Health Organisation (WHO). Action plan for the prevention of avoidable blindness and visual impairment, 2009-2013. 2009 ISBN 9789241500173.
Bourne RR . Uncorrected refractive error and presbyopia: accommodating the unmet need. Br J Ophthalmol 2007; 91 (7): 848–850.
McCarty CA . Uncorrected refractive error. Br J Ophthalmol 2006; 90 (5): 521–522.
Pizzarello L, Abiose A, Ffytche T, Duerksen R, Thulasiraj R, Taylor H et al. VISION 2020: The Right to Sight: a global initiative to eliminate avoidable blindness. Arch Ophthalmol 2004; 122 (4): 615–620.
Schneider J, Leeder SR, Gopinath B, Wang JJ, Mitchell P . Frequency, course, and impact of correctable visual impairment (uncorrected refractive error). Surv Ophthalmol 2010; 55 (6): 539–560.
Sun JK, Aiello LP, Cavallerano JD, Stockman M, Miller KM, Qin H et al. Diabetic Retinopathy Clinical Research Network. Visual acuity testing using autorefraction or pinhole occluder compared with a manual protocol refraction in individuals with diabetes. Ophthalmology 2011; 118 (3): 537–542.
Cleary G, Spalton DJ, Patel PM, Lin PF, Marshall J . Diagnostic accuracy and variability of autorefraction by the Tracey Visual Function Analyzer and the Shin-Nippon NVision-K 5001 in relation to subjective refraction. Ophthalmic Physiol Opt 2009; 29 (2): 173–181.
Cleary G, Spalton DJ, Patel PM, Lin PF, Marshall J . A randomized, clinical trial evaluating ready-made and custom spectacles delivered via a school-based screening program in China. Ophthalmology 2009; 116 (10): 1839–1845.
Keay L, Gandhi M, Brady C, Ali FS, Mathur U, Munoz B et al. A randomized clinical trial to evaluate ready-made spectacles in an adult population in India. Int J Epidemiol 2010; 39 (3): 877–888.
Brady CJ, Villanti AC, Gandhi M, Friedman DS, Keay L . Visual function after correction of distance refractive error with ready-made and custom spectacles: a randomized clinical trial. Ophthalmology 2012; 119 (10): 2014–2020.
Ramke J, du Toit R, Brian G . An assessment of recycled spectacles donated to a developing country. Clin Experiment Ophthalmol 2006; 34 (7): 671–676.
Wilson DA, Cronjé S, Frick K, Holden BA . Real cost of recycled spectacles. Optom Vis Sci 2012; 89 (3): 304–309.
Ramke J, Brian G, Palagyi A . Spectacle dispensing in Timor-Leste: tiered-pricing, cross-subsidization and financial viability. Ophthalmic Epidemiol 2012; 19 (4): 231–235.
Vincent JE . Simple spectacles for adult refugees on the Thailand-Burma border. Optom Vis Sci 2006; 83 (11): 803–810.
Read SA, Collins MJ, Carney LG . A review of astigmatism and its possible genesis. Clin Exp Optom 2007; 90 (1): 5–19.
Acknowledgements
We thank Tara Hurst, Sheila Purdy, and Harry Quigley for critique of the manuscript and Russell Treacy for preparation of the illustrations. No external funding was received for this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Treacy, M., Treacy, M., Dimitrov, B. et al. A method for the prescription of inexpensive spectacles by non-specialist healthcare workers: S-Glasses. Eye 27, 474–479 (2013). https://doi.org/10.1038/eye.2012.286
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2012.286
Keywords
This article is cited by
-
Vision care in areas of under-developed infrastructure
Journal of Public Health (2020)
