
Abstract
Aim
To evaluate the efficacy of conventional argon laser for the treatment of serosanguineous maculopathy secondary to polypoidal choroidal vasculopathy (PCV).
Methods
A retrospective audit of patients who had argon laser photocoagulation to angiographically determined polypoidal lesions and subsequently followed up at 1, 3, 6, and 12 months post treatment.
Results
Twenty-one eyes (75%) had stable or improved vision at 12 months. Twenty-three eyes had extrafoveal, two eyes had juxtafoveal, and three eyes had subfoveal polyps. In the extrafoveal group, 18 eyes (78%) had stable or improved vision at 12 months. Eighteen eyes (64.3%) showed clinical or angiographic resolution of maculopathy. Three eyes (10.7%) had recurrence of polyps subfoveally, three eyes (10.7%) had subsequent choroidal neovascularisation, and four eyes (14.3%) had persistent leakage with neurosensory detachment.
Conclusion
In our study, 18 of the 23 eyes which had extrafoveal polyps had stable or improved best-corrected visual acuity and showed complete resolution of maculopathy at 12 months follow-up. Argon laser photocoagulation would appear to be most beneficial for extrafoveal PCV. However, in view of the retrospective nature of this study, the true efficacy of argon laser treatment would have to be evaluated with a larger, prospective and randomised controlled trial.
Similar content being viewed by others

Introduction
Polypoidal choroidal vasculopathy (PCV) was a term first coined by Yanuzzi et al,1 where they described a haemorrhagic macular disease characterised by an inner choroidal network of vessels ending in an aneurysmal bulge or outward projection clinically visible as a reddish-orange polyp-like structure. Although the terminology was coined by Yannuzzi, this disease had been in fact described previously by Stern et al,2 as multiple recurrent serosanguineous retinal pigment epithelial detachments which seemed to preferentially affect African-American women. Subsequently, individuals of Asian descent were also found to have increased predisposition to this disorder.3, 4 This disease is associated with chronic, multiple, recurrent serosanguineous retinal pigment epithelium detachments (PEDs) and neurosensory detachments (NSDs) secondary to leakage and bleeding from these vascular lesions.
The pathogenesis for PCV remains unclear and the abnormality is believed to originate from the inner choroid where studies have shown that the dilated, tortuous aneurysmal vessels were of venular origin.5, 6 The choroidal lesions of PCV have also been described to occur in different locations; peripapillary, macula, temporal vascular arcade, or mid-periphery.7, 8, 9
There has been no consensus about the treatment for PCV. There have been reports of asymptomatic polyps which have been managed conservatively and have resolved spontaneously over time with preservation of good vision.10 However, for patients with PCV complicated by serosanguineous PEDs or NSDs affecting the macula, the prospects for visual recovery are uncertain and often poor. Many different treatment modalities have been used in the attempt to preserve vision in these patients. Direct laser photocoagulation,11 feeder vessel treatment,12 transpupillary thermotherapy,13 photodynamic therapy,14, 15, 16 and vitreoretinal surgery17, 18 are some of the modalities which have been described.
Few reports of laser photocoagulation for PCV have been described.11, 12, 19, 20 The results have been variable with one study reporting poor final vision and frequent relapses20 and another study reporting 20 of 37 eyes (54%) which had decreased visual acuity despite direct laser photocoagulation of polypoidal lesions.11 In our study, we report the 12-month outcomes of patients with symptomatic PCV treated with laser photocoagulation.
Patients and methods
This was a retrospectively analysed interventional case series aimed at evaluating the efficacy of laser photocoagulation for the treatment of serosanguineous maculopathy secondary to PCV. An audit of all case records of patients who presented to a tertiary ophthalmic centre (Singapore National Eye Centre) with symptomatic PCV was performed. Institutional review board approval was not required at the time this study was conducted.
All eligible patients had indocyanine green angiographically proven polypoidal lesions involving the macula and subsequently underwent direct argon laser photocoagulation to the polyps. Lesions were also classified angiographically according to their location into three groups ie subfoveal, juxtafoveal, and extrafoveal. Laser treatment was carried out using 200-μm spots of 0.2 s duration with sufficient intensity to cause a ‘greyish-white’ response extending just beyond the margins of the lesion on all sides. Best-corrected visual acuity (BCVA) was recorded before treatment and at each follow-up visit 1, 3, 6, and 12 months post-treatment. All BCVA measurements were in Snellen acuity and for purposes of analysis in our study, these were converted into logarithm of minimal angle of resolution21 (log MAR). Counting fingers and hand movements vision were allocated log MAR equivalents of 2.00 and 3.00 respectively. Primary outcome measure at 12 months was clinical or angiographic evidence showing resolution of serosanguineous maculopathy with or without associated improvement in visual acuity. Secondary outcome measure was the BCVA at 12 months.
Results
Patient characteristics
Twenty-eight eyes of 28 patients who had completed 12 months of follow-up were included in this study. There were 15 men (54%) and 13 women (46%). Twenty-six patients (93%) were Chinese, one was Malay, and one was Caucasian. The mean age at presentation was 67.1 years ranging from 49.7 to 83.5 years. There were 15 (54%) right eyes and 13 (46%) left eyes which underwent treatment. The mean visual acuity at presentation was 1.04 log MAR (range: 2.00–0.04).
Visual outcomes
At 12 months follow-up, 10 eyes (36%) had improved vision (log MAR improvement >0.2 units). Eleven eyes (39%) had stable vision (log MAR change⩽0.2 units). Seven eyes (25%) had decreased vision (log MAR decrease>0.2 units).
In the 21 eyes which had stable or improved vision, there was greater visual improvement in the first 3 months following treatment. Subsequent improvement was less marked and vision stabilised between 6 and 12 months after laser treatment. The changes of BCVA of each individual case before treatment and at 12 months follow-up are displayed in a scatter plot (Figure 1).

Scatter plot showing log MAR visual acuity (VA) at baseline and at 12 months follow-up.
There were 23 eyes (82%) with angiographically determined extrafoveal, two eyes (7%) with juxtafoveal, and three eyes (11%) with subfoveal polypoidal lesions. In the extrafoveal group, nine eyes (39%) showed improved vision, nine eyes (39%) had stable vision, and five eyes had decreased vision.
In the juxtafoveal group, one patient improved from a baseline log MAR of 0.60–0.32 and one patient decreased from baseline log MAR of 0.48–1.30 due to subfoveal extension of the lesion. In the subfoveal group, one patient retained stable vision, one patient decreased from baseline log MAR of 1.30–2.00 due to persistent haemorrhage and PED, and one patient decreased from a baseline log MAR of 0.42–0.60 due to recurrent subfoveal haemorrhage.
The mean number of treatments was 1.11. Three patients required repeat laser treatment; two from the extrafoveal group and one from the subfoveal group. After the second treatment, one patient from the extrafoveal group achieved stable vision at 12 months (log MAR, 2.00); the other patient had a subfoveal recurrence and went on to have photodynamic therapy. The patient from the subfoveal group retained stable vision (log MAR, 2.00) despite persistent NSD and he declined photodynamic therapy when it was offered to him.
Resolution of maculopathy
Clinically, all eyes had presented with a combination of subretinal haemorrhage and/or PED involving the macula and/or the presence of an ‘orange-coloured’ lesion adjacent to the area of haemorrhage or PED. The presence of polyps was confirmed by indocyanine green angiography.
Eighteen eyes (64.3%) had clinical and/or angiographic evidence of complete resolution of maculopathy at 12 months follow-up. Thirteen of these 18 eyes also had associated stabilisation or improvement of BCVA. Seventeen of these had extrafoveal lesions.
There were three eyes (10.7%) which had subfoveal recurrence of polyps; two of which had presented with extrafoveal lesions. Two of these eyes lost further vision and all three eyes eventually went on to have photodynamic therapy.
There were three eyes (10.7%), all from the extrafoveal group, which had subsequent choroidal neovascularisation. All three eyes were managed conservatively.
The remaining four eyes (14.3%; three subfoveal and one extrafoveal) had persistent leakage and NSD and were all managed conservatively.
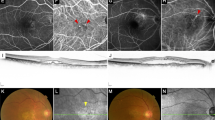
(Clinical example shown in Figure 2).

Fundus photo of a patient's left eye and the indocyanine green angiogram showing an extrafoveal polyp before (middle) and 6 months after laser treatment(right). The lesion had completely resolved with laser treatment.
Discussion
The pathogenesis of PCV is not completely understood and these polyp-like choroidal vascular abnormalities can cause significant morbidity particularly when affecting the macula. There are significant variations in the natural course of PCV and some lesions have been reported to remain quiescent or resolve spontaneously with preservation or restoration of good vision.8, 10 However, persistent leakage from these lesions can lead to chronic pigment epithelial and NSDs as well as recurrent haemorrhages and in some circumstances, a breakthrough vitreous haemorrhage.17 Ultimately, there can be permanent visual loss from atrophy and degeneration of the retinal pigment epithelium and outer retina.
The natural history of PCV has not been described extensively. However, what little that has been reported tends to point towards an unfavourable outcome with observation alone. Yuzawa et al11 reported only five of 21 eyes (24%) with PCV involving the macula had visual improvement with conservative management over a follow-up period of 3 years (IOVS 42 (supp): S800, 2001). Uyama et al10 reported that five of 14 eyes (36%) lost more than two lines of vision over a follow-up period of 2 years. Kwok et al22 also described a loss of vision of two lines or more in 7 of 9 eyes (78%), which had PCV involving the macula and were managed conservatively. Therefore, in most instances where patients have significant symptomatic visual loss, treatment is often considered.
Laser photocoagulation for PCV has been described previously11, 12, 23, 24 but results have been variable. Lafaut et al23 showed poor response in four of nine eyes which had laser treatment in macular lesions with persistent or increased exudation. In another series, four of nine eyes treated by laser had loss of vision >2 lines.22 In our series, 21 of 28 eyes (75%) remained stable or had improvement of visual acuity after laser photocoagulation. Eighteen of 28 eyes (64.3%) had complete resolution of maculopathy following treatment and 17 of these eyes had extrafoveal lesions.
The results of our study at 1-year follow-up show that laser photocoagulation of polypoidal lesions for the treatment of symptomatic serosanguineous maculopathy seems to offer the most benefit for patients with extrafoveal lesions. Eighteen of the 23 eyes with extrafoveal polyps had stable or improved vision at 12 months whereas one (of two eyes) with juxtafoveal and two (of three eyes) with subfoveal lesions had decreased vision. In the majority of cases, only one session of treatment was required. However, we are aware of the limitations of this retrospective analysis which include a small sample size, the lack of a control group for comparison, the lack of a standardised treatment protocol, and a 1-year follow-up, which is still relatively short in the context of this chronic disease.
We did also observe recurrence of PCV in three eyes. The recurrence in all three eyes were subfoveal in location and interestingly two of these three eyes had extrafoveal polyps at initial presentation. Secondary choroidal neovascularisation occurred in another three eyes, all of which presented with extrafoveal polyps. The choroidal neovascularisation in these eyes could be secondary to laser damage to Bruch's membrane or could have occurred as part of the spectrum of age-related macular degeneration as described previously.3, 5 Another four eyes (three subfoveal, one extrafoveal) had persistent maculopathy despite laser treatment. Therefore, a randomised-controlled trial would be useful to provide more evidence of the true efficacy of argon laser photocoagulation for the treatment of PCV.
In summary, PCV is a clinical entity with a chronic and relapsing course that can cause significant morbidity from recurrent or persistent leakage. Our series has demonstrated a positive outcome for this disease with laser photocoagulation mainly for extrafoveal PCV. There was clinical resolution of maculopathy in almost two-thirds of patients and three-quarters of patients had stable or improved vision at 12 months follow-up.
References
Yanuzzi LA, Sorenson J, Spaide RF, Lipson B . Idiopathic polypoidal choroidal vasculopathy. Retina 1990; 10: 1–8.
Stern RM, Zakov N, Zegarra H . Multiple recurrent serous sanguineous retinal pigment epithelial detachments in black women. Am J Ophthalmol 1985; 100: 560–569.
Iijima H, Imai M, Gohodo T . Optical coherence tomography of idiopathic choroidal vasculopathy. Am J Ophthalmol 1999; 127: 301–305.
Lip PL, Hope-Ross MW, Gibson JM . Idiopathic polypoidal choroidal vasculopathy: a disease with diverse clinical spectrum and systemic associations. Eye 2000; 5: 695–700.
Lafaut BA, Aisenbrey S, van den Broecke C . Polypoidal choroidal vasculopathy pattern in age-related macular degeneration. Retina 2000; 20: 650–654.
Okubo A, Sameshima M, Uemara A . Clinicopathological correlation of polypoidal choroidal vasculopathy revealed by ultrastructural study. Br J Ophthalmol 2002; 86: 1093–1098.
Moorthy RS, Lyon AT, Rabb MF, Spaide RF, Yanuzzi LA, Jampol LM . Idiopathic polypoidal choroidal vasculopathy of the macula. Ophthalmology 1998; 105: 1380–1385.
Yannuzzi LA, Ciardella A, Spaide RF, Rabb MF, Freund KB, Orlock . The expanding clinical spectrum of idiopathic polypoidal choroidal vasculopathy. Arch Ophthalmol 1997; 115: 478–485.
Spaide RF, Yannuzzi LA, Slakter JS, Sorenson J, Orlach DA . Indocyanine green videoangiography of idiopathic choroidal vasculopathy. Retina 1995; 15: 100–110.
Uyama M, Wada M, Nagai Y . Polypoidal choroidal vasculopathy; a natural history. Am J Ophthalmol 2002; 133: 639–648.
Yuzawa M, Mori R, Haruyama M . A study of laser photocoagulation for polypoidal choroidal vasculopathy. Jpn J Ophthalmol 2003; 47 (4): 379–384.
Nishijima K, Takahashi M, Akita J, Katsuta H, Tanemura M, Aikawa H . Laser photocoagulation of indocyanine green angiographically identified feeder vessels to idiopathic polypoidal choroidal vasculopathy. Am J Ophthalmol 2004; 137 (4): 770–773.
Vedantham V, Kolluru C, Ramasamy K . Treatment of polypoidal choroidal vasculopathy with transpupillary thermotherapy; an interventional case report. Eye 2005; 19 (8): 915–917.
Chan WM, Lam DS, Lai TY, Liu DT, Li KK, Yao Y . Photodynamic therapy with verteporfin for symptomatic polypoidal choroidal vasculopathy: one year results of a prospective case series. Ophthalmology 2004; 111 (8): 1176–1184.
Quaranta M, Mauget-Faysse M, Coscas G . Exudative idiopathic polypoidal choroidal vasculopathy and photodynamic therapy with verteporfin. Am J Ophthalmol 2002; 134: 277–280.
Spaide RF, Donsoff I, Lam DL, Yanuzzi LA, Jampol LM, Slakter J . Treatment of polypoidal choroidal vasculopathy with photodynamic therapy. Retina 2002; 22: 529–535.
Shiraga F, Matsua T, Yokoe S, Takasu I, Okanouchi T, Ohtsuki H . Surgical treatment of submacular haemorrhage associated with idiopathic polypoidal choroidal vasculopathy. Am J Ophthalmol 1999; 128: 147–154.
Terasaki H, Miyake Y, Suzuki T, Nakamura M, Nagasaka T . Polypoidal choroidal vasculopathy treated with macular translocation: clinical pathological correlation. Br J Ophthalmol 2002; 86: 321–327.
Gomez-Ulla F, Gonzalez F, Torreiro MG . Diode laser photocoagulation in idiopathic polypoidal choroidal vasculopathy. Retina 1998; 18 (5): 481–483.
Vilaplana D, Castilla M, Poposki V . Laser photocoagulation in idiopathic polypoidal choroidal vasculopathy. Over one year follow up. Arch Soc Esp Oftalmol 2005; 80 (10): 597–602.
Holladay JT . Visual acuity measurements. J Cataract Refract Surg 2004; 30: 287–290.
Kwok AK, Lai TY, Chan CW, Neoh EL, Lam DS . Polypoidal choroidal vasculopathy in Chinese patients. Br J Ophthalmol 2002; 86: 892–897.
Lafaut BA, Leys AM, Snyers B, Rasquin F, De Laey JJ . Polypoidal choroidal vasculopathy in Caucasians. Graefes Arch Clin Exp Ophthalmol 2000; 238: 752–759.
Ahuja RM, Stanga PE, Vingerling JR, Reck AC, Bird AC . Polypoidal choroidal vasculopathy in exudative and haemorrhagic pigment epithelial detachments. Br J Ophthalmol 2000; 84: 479–484.
Author information
Authors and Affiliations
Corresponding author
Additional information
Proprietary interests: the authors have no proprietary interests in any drugs or equipment described in this paper
Financial support: no financial support was received for this paper Proprietary interests: the authors have no proprietary interests in any drugs or equipment described in this paper
Meeting presentation: This paper was presented at the 2005 American Academy of Ophthalmology Annual Meeting, Chicago
Rights and permissions
About this article
Cite this article
Lee, MW., Yeo, I., Wong, D. et al. Argon laser photocoagulation for the treatment of polypoidal choroidal vasculopathy. Eye 23, 145–148 (2009). https://doi.org/10.1038/sj.eye.6702955
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702955
Keywords
This article is cited by
-
Macular neovascularization and polypoidal choroidal vasculopathy: phenotypic variations, pathogenic mechanisms and implications in management
Eye (2024)
-
Activation of quiescent polypoidal choroidal vasculopathy after membrane peeling vitrectomy for epiretinal membrane: a case report
BMC Ophthalmology (2021)
-
Polypoidal Choroidal Vasculopathy
Current Ophthalmology Reports (2019)
-
Assessment of focal laser photocoagulations’ early effect on polypoidal choroidal vasculopathy with optical coherence tomography angiography
Lasers in Medical Science (2018)
-
Photodynamic therapy: current role in the treatment of chorioretinal conditions
Eye (2016)
