
Abstract
Objective: Our objective was to assess effects of dietary supplementation with coenzyme Q10 (CoQ) on blood pressure and glycaemic control in subjects with type 2 diabetes, and to consider oxidative stress as a potential mechanism for any effects.
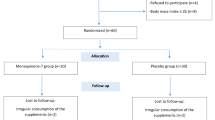
Subjects and design: Seventy-four subjects with uncomplicated type 2 diabetes and dyslipidaemia were involved in a randomised double blind placebo-controlled 2×2 factorial intervention.
Setting: The study was performed at the University of Western Australia, Department of Medicine at Royal Perth Hospital, Australia.
Interventions: Subjects were randomly assigned to receive an oral dose of 100 mg CoQ twice daily (200 mg/day), 200 mg fenofibrate each morning, both or neither for 12 weeks.
Main outcome measures: We report an analysis and discussion of the effects of CoQ on blood pressure, on long-term glycaemic control measured by glycated haemoglobin (HbA1c), and on oxidative stress assessed by measurement of plasma F2-isoprostanes.
Results: Fenofibrate did not alter blood pressure, HbA1c, or plasma F2-isoprostanes. There was a 3-fold increase in plasma CoQ concentration (3.4±0.3 µmol/l, P<0.001) as a result of CoQ supplementation. The main effect of CoQ was to significantly decrease systolic (−6.1±2.6 mmHg, P=0.021) and diastolic (−2.9±1.4 mmHg, P=0.048) blood pressure and HbA1c (−0.37±0.17%, P=0.032). Plasma F2-isoprostane concentrations were not altered by CoQ (0.14±0.15 nmol/l, P=0.345).
Conclusions: These results show that CoQ supplementation may improve blood pressure and long-term glycaemic control in subjects with type 2 diabetes, but these improvements were not associated with reduced oxidative stress, as assessed by F2-isoprostanes.
Sponsorship: This study was supported by a grant from the NH&MRC, Australia.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


References
Anderson RA, Evans ML, Ellis GR, Graham J, Morris K, Jackson SK, Lewis MJ, Rees A, Frenneaux MP . 2001 The relationships between post-prandial lipaemia, endothelial function and oxidative stress in healthy individuals and patients with type 2 diabetes Atherosclerosis 154: 475–483
Bonnefont-Rousselot D, Bastard JP, Jaudon MC, Delattre J . 2000 Consequences of the diabetic status on the oxidant/antioxidant balance Diabetes Metabol. 26: 163–176
Burke BE, Neuenschwander R, Olson RD . 2002 Randomised double-blind, placebo-controlled trial of coenzyme Q10 in isolated systolic hypertension Southern Med. J. 94: 1112–1117
Ceriello A . 2000 Oxidative stress and glycemic regulation Metab. Clin. Exp. 49: (Suppl 1): 27–29
Digiesi V, Cantini F, Brodbeck B . 1990 Effect of coenzyme Q10 on essential arterial hypertension Curr. Ther. Res. 47: 841–845
Eriksson JG, Forsen TJ, Mortensen SA, Rohde M . 1999 The effect of coenzyme Q10 administration on metabolic control in patients with type 2 diabetes mellitus Biofactors 9: 315–318
Grunfeld S, Hamilton CA, Mesaros S, McClain SW, Dominiczak AF, Bohr DF, Malinski T . 1995 Role of superoxide in the depressed nitric oxide production by the endothelium of genetically hypertensive rats Hypertension 26: 854–857
Henriksen JE, Andersen CB, Hother-Nielsen O, Vaag A, Mortensen SA, Beck-Nielsen H . 1999 Impact of ubiquinone (coenzyme Q(10)) treatment on glycaemic control, insulin requirement and well-being in patients with Type 1 diabetes mellitus Diabetic Med. 16: 312–318
Hodgson JM, Puddey IB, Croft KD, Mori TA, Rivera J, Beilin LJ . 1999 Isoflavonoids do not inhibit in vivo lipid peroxidation in subjects with high-normal blood pressure Atherosclerosis 145: 167–172
Jameson S . 1991 Coenzyme Q10, alpha-tocopherol, and free cholesterol levels in sera from diabetic patients In: ed. K Folkers, G Littarru & T Yamagami Biomedical and Clinical Aspects of Coenzyme Q pp 151–158 Amsterdam: Elsevier Science
Kitiyakara C, Wilcox CS . 1998 Antioxidants for hypertension Curr. Opin. Nephr. Hypertens. 7: 531–538
Lang JK, Gohil K, Packer L . 1986 Stimultaneous determination of tocopherols, ubiquinols and ubiquinones in blood, plasma, tissue homogenates, and sucellular fractions Anal. Biochem. 157: 106–116
Lawson JA, Rokach J, FitzGerald GA . 1999 Isoprostanes: formation, analysis and use as indices of lipid peroxidation in vivo J. Biol. Chem. 274: 24441–24444
McCarty MF . 1999 Can correction of sub-optimal coenzyme Q status improve beta-cell function in type II diabetics? Med. Hypoth. 52: 397–400
Mori TA, Croft KD, Puddey IB, Beilin LJ . 1999 An improved method for the measurement of urinary and plasma F2-isoprostanes using gas chromatography-mass spectrometry Anal. Biochem. 268: 117–125
Nishikawa T, Edelstein D, Du XL, Yamagishi S, Matsumura T, Kaneda Y, Yorek MA, Beebe D, Oates PJ, Hammes HP, Giardino I, Brownlee M . 2000 Normalizing mitochondrial superoxide production blocks three pathways of hyperglycaemic damage Nature 404: 787–790
Overvad K, Diamant B, Holm L, Holmer G, Mortensen SA, Stender S . 1999 Coenzyme Q10 in health and disease Eur. J. Clin. Nutr. 53: 764–770
Raitakari OT, McCredie RJ, Witting P, Griffiths KA, Letters J, Sullivan D, Stocker R, Celermajer DS . 2000 Coenzyme Q improves LDL resistance to ex vivo oxidation but does not enhance endothelial function in hypercholesterolaemic young adults Free Rad. Biol. Med. 28: 1100–1105
Roberts LJ, Morrow JD . 2000 Measurement of F(2)-isoprostanes as an index of oxidative stress in vivo Free Rad. Biol. Med. 28: 505–513
Singh RB, Niaz MA, Rastogi SS, Shukla PK, Thakur AS . 1999 Effect of hydrosoluble coenzyme Q10 on blood pressures and insulin resistance in hypertensive patients with coronary artery disease J. Hum. Hypertens. 13: 203–208
Thomas SR, Witting PK, Stocker R . 1999 A role for reduced coenzyme Q in atherosclerosis? Biofactors 9: 207–224
Watts GF, Playford DA, Croft KD, Ward NC, Mori TA, Burke V . 2002 Coenzyme Q10 improves endothelial dysfunction of the brachial artery in type II diabetes mellitus Diabetologia 45: 420–426
West IC . 2000 Radicals and oxidative stress in diabetes Diabetic Med. 17: 171–180
Yamagami T, Takagi M, Akagami H, Kubo H, Toyama S, Okamoto T . 1986 Effect of coenzyme Q10 on essential hypertension: a double blind controlled study In: Biomedical and Clinical Aspects of Coenzyme Q ed. K Folkers, G Littarru & T Yamagami, pp 337–343 Amsterdam: Elsevier Science
Acknowledgements
We are grateful to Ms Mary-Ann Powell for expert nursing assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hodgson, J., Watts, G., Playford, D. et al. Coenzyme Q10 improves blood pressure and glycaemic control: a controlled trial in subjects with type 2 diabetes. Eur J Clin Nutr 56, 1137–1142 (2002). https://doi.org/10.1038/sj.ejcn.1601464
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejcn.1601464
Keywords
This article is cited by
-
Effects of curcumin and/or coenzyme Q10 supplementation on metabolic control in subjects with metabolic syndrome: a randomized clinical trial
Nutrition Journal (2022)
-
Could nutrient supplements provide additional glycemic control in diabetes management? A systematic review and meta-analysis of randomized controlled trials of as an add-on nutritional supplementation therapy
Archives of Pharmacal Research (2022)
-
Potential Therapeutic Use of Coenzyme Q10 in Diabetes Mellitus and Its Complications: an Algorithm of Scoping Clinical Review
SN Comprehensive Clinical Medicine (2021)
-
Enhancement of NADPH availability for coproduction of coenzyme Q10 and farnesol from Rhodobacter sphaeroides
Journal of Industrial Microbiology and Biotechnology (2020)
-
Co-production of farnesol and coenzyme Q10 from metabolically engineered Rhodobacter sphaeroides
Microbial Cell Factories (2019)
