
Abstract
Data sources
All studies with questionnaire items on mouthwash use in the International Head and Neck Cancer Epidemiology Consortium (INHANCE).
Data extraction and synthesis
Pooled analysis data from case controlled studies using Individual Patient Data (IPD) meta-analysis methods. Logistic regression was used to assess the association of mouthwash use with cancers of the oral cavity, oropharynx, hypopharynx and larynx, adjusting for study, age, sex, pack-years of tobacco smoking, number of alcoholic drinks/day and education.
Results
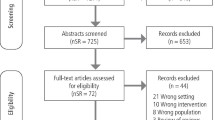
Eight thousand, nine hundred and eighty-one cases of head and neck cancer and 10,090 controls from 12 case-control studies with comparable information on mouthwash use were included in the analysis. Compared with never users of mouthwash, the odds ratio (OR) of all head and neck cancers was 1.01 [95% confidence interval (CI): 0.94-1.08] for ever users, based on 12 studies. The corresponding ORs of cancer of the oral cavity and oropharynx were 1.11 (95% CI: 1.00-1.23) and 1.28 (95% CI: 1.06-1.56), respectively.
Conclusions
Although limited by the retrospective nature of the study and the limited ability to assess risks of mouthwash use in nonusers of tobacco and alcohol, this large investigation shows potential risks for head and neck cancer subsites and in long-term and frequent users of mouthwash.
Similar content being viewed by others

Commentary
As a hospital dental practitioner and public health dentist respectively, we would not advise or advocate the regular use of mouthwash as part of routine oral hygiene treatment for our patients or the public. However, studies have shown that mouthwashes can have a role in, for example, the prevention of surgical complications (such as prophylactic use in third molar surgery reduces the risk of alveolar osteitis),1 and in the delivery of fluoride to prevent root caries.2 Nevertheless mouthwash is widely advertised and used, with market research suggesting sales have risen substantially in recent years, with an estimated 55% of the UK population using mouthwash – spending approximately £197 million in 2013.3
Recently, a large Latin American and two large European multicentre case-control studies4,5 indicated an increased risk of head and neck cancer associated with frequent (greater than twice per day) use. However, a meta-analysis observed a dose-effect relationship with increasing frequency of mouthwash use, but the corresponding risk estimates were unstable and not statistically significant.6
The International Head and Neck Cancer Epidemiology (INHANCE)7 consortium is a wide collaboration of researchers, founded in 2004, which aims to investigate risk factors for head and neck cancer by pooling data from case-control studies from across the world.8 We declare that one of the authors (DC) of this commentary is a founding member of INHANCE, however he is not an author of this INHANCE article on mouthwash.
INHANCE enables powerful analysis of head and neck cancer risk going beyond traditional alcohol and smoking risk estimates, via pooling individual study participant social, demographic and behavioural data from approximately 26,000 cases of head and neck cancer and 34,000 controls.7,9
This study involved a reasonably large sample of cases/controls (n=8981/10090), obtained from 12 case-control studies with available data on mouthwash use.10 It utilised Individual Patient Data (IPD) meta-analysis methods. Long-term use of mouthwash (>36 years) resulted in a significant increased risk of head and neck cancer (OR 1.15; 95% CI 1.01 - 1.30) and a higher risk with higher frequency (>1 x daily) of use (OR 1.31; 95% CI 1.09 - 1.58). Moreover, the combination of regular (>2 x daily), long-term (>35 years) use and head and neck cancer was higher still (OR 1.75; 95% CI 1.25 - 2.48). Specifically, in relation to oral cavity cancer the risk associated with mouthwash use of more than 35 years was also significant (OR 1.28; 95% CI 1.06-1.56). Estimates were adjusted for risk factors, smoking and alcohol, with risk increasing particularly in smokers.
This study was the largest analysis to date investigating the relationship between mouthwash and head and neck cancer risk. While the data are pooled from several studies, all included studies collected data in a conceptually similar way and there was considerable data standardisation.8 Nevertheless, case-control study design of the original studies with historical data collection does not exclude the possibility of recall bias.
Other limitations include; difficulty decoupling smoking and alcohol behaviours which are recognised risks for head and neck cancer from excessive mouthwash and residual confounding is a distinct possibility – particularly where heavy mouthwash could be used to mask smoking and alcohol behaviour, or mouthwash could be used as a form of alcohol abuse.11 Heavy mouthwash use may also be used in place of adequate oral hygiene practices, which is also emerging as a risk factor associated with head and neck cancer.5 The final issue with the study is the lack of information on alcohol content of the mouthwash, with alcohol the hypothesised aetiology process, although as the authors report 'most of the products used in these studies contained alcohol'.10
This study adds to the evidence identified by recent large studies4 that support this tendency for increased risk of head and neck cancer with excessive, high frequency or prolonged use of mouthwash.
While these are not definitive findings, they cannot be ignored and they further support our professional opinion and advice that high frequency and prolonged use of mouthwash is not a routine component of good oral hygiene.
References
Hermesch CB, Hilton TJ, Biesbrock AR, et al. Perioperative use of 0.12% chlorhexidine gluconate for the prevention of alveolar osteitis: efficacy and risk factor analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998; 85: 381–387.
Wierichs RJ, Meyer-Lueckel H . Systematic review on noninvasive treatment of root caries lesions. J Dent Res 2015; 94: 261–271.
Mintel's Oral Care – UK Report 2014. http://www.mintel.com/press-centre/household-press-centre/half-of-britains-parents-do-not-take-their-children-to-the-dentist-regularly-reports-mintel. [Accessed March 2016].
Ahrens W, Pohlabeln H, Foraita R, et al. Oral health, dental care and mouthwash associated with upper aerodigestive tract cancer risk in Europe: the ARCAGE study. Oral Oncol 2014; 50: 616–625.
Guha N, Boffetta P, Wünsch Filho V, et al. Oral health and risk of squamous cell carcinoma of the head and neck and esophagus: results of two multicentric case-control studies. Am J Epidemiol 2007; 166: 1159–1173.
Gandini S, Negri E, Boffetta P, La Vecchia C, Boyle P . Mouthwash and oral cancer risk quantitative meta-analysis of epidemiologic studies. Ann Agric Environ Med 2012; 19: 173–180.
International Head and Neck Cancer Epidemiology Consortium, The University of Utah, http://www.inhance.utah.edu [Accessed 12 March 2016]
Conway DI, Hashibe M . Boffetta P ; INHANCE consortium, et al. INHANCE consortium. Enhancing epidemiologic research on head and neck cancer: INHANCE – the international head and neck cancer epidemiology consortium. Oral Oncol 2009; 45: 743–746.
Winn D, Lee YC, Hashibe M . Boffetta P ; INHANCE consortium. The INHANCE consortium: toward a better understanding of the causes and mechanisms of head and neck cancer. Oral Dis 2015; 21: 685–693.
Boffetta, Hayes RB, Sartori S, et al. Mouthwash use and cancer of the head and neck: a pooled analysis from the International Head and Neck Cancer Epidemiology Consortium. Eur J Cancer Prev 2015; [Epub ahead of print].
Egbert AM, Reed JS, Powell BJ, Liskow BI, Liese BS . Alcoholics who drink mouthwash: the spectrum of nonbeverage alcohol use. J Stud Alcohol 1985; 46: 473–481.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Paolo Boffetta, MD, Icahn School of Medicine at Mount Sinai, New York, New York 10029, USA. E-mail: paolo.boffetta@mssm.edu
Boffetta P, Hayes RB, Sartori S, et al. Mouthwash use and cancer of the head and neck: a pooled analysis from the International Head and Neck Cancer Epidemiology Consortium. Eur J Cancer Prev 2015; [Epub ahead of print] PubMed PMID: 26275006; PubMed Central PMCID: PMC4752930.
Rights and permissions
About this article

Cite this article
Wilson, G., Conway, D. Mouthwash use and associated head and neck cancer risk. Evid Based Dent 17, 8–9 (2016). https://doi.org/10.1038/sj.ebd.6401146
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401146
