
Abstract
Data sources
Medline.
Study selection
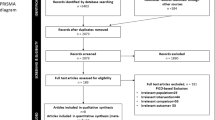
Clinical trials of orthodontic mini-screws with a minimum of 30 cases providing data on the patient, mini-screw, surgery and loading available for correlation with the mini-screws' success rates in English or German were included.
Data extraction and synthesis
Data were extracted that correlated with the miniscrews' success rate: patient sex and age, screw length and diameter, method and location of placement, time and amount of loading. The statistical analyses were performed using SPSS software (version 13 for Mac OS X, SPSS, Chicago, Ill).
Results
Fourteen clinical trials (452 patients and 1519 screws) were included, with overall success rates ranging from 59.4% to 100%. The mean success rate was 83.6% ±10.2%. Screw diameters of 1 to 1.1 mm yielded significantly lower success rates than those of 1.5 to 2.3 mm. One study reported significantly lower success rates for 6 mm vs 8 mm long mini-screws (72% vs 90%). Screw placement with or without a surgical flap showed contradictory results between studies. Three studies showed significantly higher success rates for maxillary than for mandibular screws. Loading and healing periods were not significant in the mini-screws' success rates. There was no influence of patient sex and one study found significantly greater success in patients over 30 years of age.
Conclusions
All 14 articles described success rates sufficient for orthodontic treatment. Placement protocols varied markedly. Screws under 8 mm in length and 1.2 mm in diameter should be avoided. Immediate or early loading up to 200 cN was adequate and showed no significant influence on screw stability.
Similar content being viewed by others


Commentary
The term “mini-screw” is one of a number used to describe small screws, surgically placed through alveolar cortical bone to be used as temporary anchorage devices in orthodontic treatment. They have become increasingly prevalent in the past decade as they confer a number of advantages when compared to traditional intra-oral and extra-oral anchorage reinforcement.
There is marked heterogeneity in mini-screw design and placement techniques. This review was constructed with the aim of analysing the success rates of mini-screws with a view to defining a set of guidelines for their selection and application. The validity of this review is compromised somewhat by the use of only one database in collating any relevant articles; the paucity of search terms is also discouraging. However, upon comparison with other relevant papers,1,2 it does appear that the studies included are representative of the available literature. A detailed analysis of each article would also have been desirable; however, information such as the design of each study was unreported. Given one of the main aims was to discern the success rates of mini-screws, a discussion of what is deemed a success would seem to be appropriate. Although not forthcoming, it is pertinent to realise that ‘success’ differs in the discussed articles. It is most frequently seen as gaining ‘anchorage for required treatment time’ and so mobile/displaced mini-screws can still be seen as a success provided they can still be used to reinforce anchorage.
Accepting these issues, the quoted success rate of over 80% is comparable with that derived in other reviews on the subject. Of worthy mention is one such paper containing more contemporary data on an additional five studies yielding an increase of over 800 mini-screws in its analysis.3 However, the overall success rate changes little.
When comparing the time allowed for the mini-screw to heal before loading, along with the magnitude of the subsequently applied force, there was considerable variation between the studies and within study groups. Along with the poorer performance observed with mini-screws of less than 1.2mm diameter and 8mm in length, these areas generate further avenues for investigation.
Given that this area of orthodontic research is still in its infancy, the data shown here can be seen as a starting point for the design of suitable prospective studies to help elucidate the most efficacious method for mini-screw placement.
Practice points
-
Mini-screws can be used successfully to reinforce anchorage in orthodontic treatment with current data suggesting a failure rate of less than one in five.
-
A standardised protocol yielding the highest chance of success remains elusive
References
Chen Y, Kyung HM, Zhao WT, et al. Critical factors for the success of orthodontic mini-implants: a systematic review. Am J Orthod Dentofacial Orthop. 2009; 135: 284–291.
Reynders R, Ronchi L, Bipat S . Mini-implants in orthodontics: a systematic review of the literature. Am J Orthod Dentofacial Orthop. 2009; 135: 564 e1–19; discussion -5.
Schatzle M, Mannchen R, Zwahlen M, et al. Survival and failure rates of orthodontic temporary anchorage devices: a systematic review. Clin Oral Implants Res 2009; 20: 1351–1359.
Author information
Authors and Affiliations
Additional information
Address for correspondence; Adriano G. Crismani, University Clinic of Orthodontics, Department of Dentistry and Maxillofacial Surgery, Medical University of Innsbruck, Innsbruck, Austria. E-mail: adriano.crismani@i-med.ac.at
Crismani AG, Bertl MH, Celar AG, Bantleon HP, Burstone CJ. Miniscrews in orthodontic treatment: review and analysis of published clinical trials. Am J Orthod Dentofacial Orthop 2010; 137: 108-113.
Rights and permissions
About this article
Cite this article
Stanford, N. Mini-screws success rates sufficient for orthodontic treatment. Evid Based Dent 12, 19 (2011). https://doi.org/10.1038/sj.ebd.6400777
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400777
This article is cited by
-
The Effects of Diameter, Length and Insertion Method on the Stability of Orthodontic Miniscrew
Journal of Medical and Biological Engineering (2022)
-
RFA measurements of survival midpalatal orthodontic mini-implants in comparison to initial healing period
Progress in Orthodontics (2020)
-
Accuracy of torque-limiting devices for mini-implant removal: an in vitro study
Journal of Orofacial Orthopedics / Fortschritte der Kieferorthopädie (2013)
-
Accuracy of torque-limiting devices used for mini-implant placement—an in vitro study
Journal of Orofacial Orthopedics / Fortschritte der Kieferorthopädie (2013)
-
Multipurpose use of orthodontic mini-implants to achieve different treatment goals
Journal of Orofacial Orthopedics / Fortschritte der Kieferorthopädie (2012)
