
Abstract
Data sources
PubMed, EMBASE, Web of Science, Cochrane library, China Biology Medicine Disc (CBM), China National Knowledge infrastructure (CNKI).
Study Selection
This study included only human randomised controlled trials (RCTs) and clinical controlled trials (CCTs). To be included studies had to include patients prescribed oral anticoagulant therapy (OAT) requiring dental extraction(s). Comparison was made between patients discontinuing OAT for the dental extraction(s) and those continuing with their OAT. The outcome measured was post-operative bleeding identified by clinician or patient.
Data extraction and synthesis
The methods of data extraction were based on the Cochrane Handbook for Systematic Reviews of Interventions. The search was carried out by two reviewers from the data sources listed above. There was no indication of hand searching references of relevant studies or reputable publications, nor any mention of contacting clinical experts or researchers in this field. Language restrictions were unclear. The included studies were assessed for bias using a seven point classification, and a clear traffic light diagram was included to demonstrate the risk of bias of the included studies.
Results
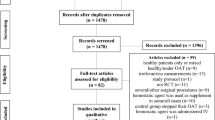
Nine hundred and sixty-eight studies were identified with six meeting the inclusion and exclusion criteria. Of the six studies, four were RCTs and two were CCTs encompassing 314 subjects who continued their OAT during tooth extraction(s) and 277 who discontinued their OAT to allow for tooth extraction(s). Five of the six studies were found to have high risk of bias.
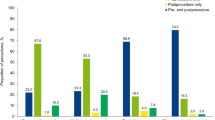
A meta-analysis of the six studies was conducted. The incidence of post-operative bleeding was 10.8% where OAT was continued and 8.3% where it was discontinued, showing no statistically significant difference. The relative risk ratio to continuing OAT during tooth extraction was 1.31 and 95% confidence interval, albeit with a wide range of 0.79-2.14.
Conclusions
According to the current literature available on this subject, the results of this meta-analysis suggest that patients continuing OAT during tooth extraction do not have an increased incidence of post-operative bleeding following tooth extraction compared to patients who discontinue their OAT.
Similar content being viewed by others

Commentary
Oral anticoagulant therapy (OAT) is used to prophylactically prevent or reduce thrombosis in patients who suffer from a variety of conditions. These include cardiovascular diseases such as atrial fibrillation, venous thromboembolism such as deep vein thrombosis (DVT) and patients who have mechanical heart valves in certain cases.1 Therefore this makes the use of OAT a common finding in the general patient population.
Oral anticoagulant medications are found in many forms including Warfarin, Heparin and newer oral anticoagulants. Warfarin, a vitamin K agonist, is widely used for many conditions. Heparin is less widely used and administered intravenously, interfering with thrombin-antithrombin pathways. Common new anticoagulants include Rivaroxiban, Apixaban and Edoxaban; all factor Xa inhibitors. Dabigatran, a factor IIa inhibitor, is another form of new oral anticoagulant.2
The risk to a patient taking OAT who requires a dental extraction is the increased chance of haemorrhage both at the time of and post-surgery. This has resulted in some practitioners wishing to discontinue the use of OAT around the time of tooth extraction to prevent this risk.3
However, the risks to discontinuing OAT could be more grave, namely thromboembolism which could result in embolic stroke or even potentially fatality. Indeed, thromboembolic events following discontinuing of OAT for tooth extraction have been reported in the literature,4,5 although generally the risk is low.6
This review is clear in the databases searched, how inclusion and exclusion criteria were applied and the assessment of the quality and validity of the available evidence. Only RCTs and CCTs were included assessing human subjects, which would be suitable studies to be used in a meta-analysis of this intervention. Regardless, there was a high degree of heterogeneity between studies in the form of the type of drug used, the amount of teeth for extraction, the follow-up period post-operatively and the bleeding outcome measured. Moreover five of the six studies were identified to have high levels of bias.
The subjects were prescribed Warfarin in four of the included studies; in the remaining two studies one analysed patients taking a Vitamin K inhibitor and the final study failed to identify the drug used for OAT. This means commonly used anticoagulants such as Heparin as well as new oral anticoagulant drugs such as Rivaroxiban, Apixaban, Edoxaban and Dabigatran were not knowingly included in this analysis. One of the reasons for this omission may be the search terms used in the initial literature search which did not include any generic or trade drug names that may have identified further studies.
Antiplatelet drugs were also excluded from this study, in keeping with the title; however, these may have been a welcome addition given their increasing use in the general population.7 In addition follow-up was of short duration ranging from one to seven days across the studies and the method of measurement of outcomes differed between studies.
The validity of the meta-analysis is questionable given the differing medications and high risk of bias in the majority of the studies. The authors identify many limitations of their study in the discussion including those mentioned above, in addition to the small sample size of some of the studies, the differences in INR levels between studies, the types of surgery provided, the clinical skill of the clinician and the type of intervention provided when bleeding occurred.
Nonetheless the results of the study are in agreement with the majority of the current literature, including systematic reviews and clinical studies, which suggest there is limited evidence available to advocate discontinuing OAT for minor dental surgery.8,9,10
Standardisation of reporting of bleeding outcomes post surgeries across the literature, and more robust RCTs and CCTs in the future with larger sample sizes may aid in further discussion on this topic.
References
Marcy TR, Truong T, Rai A . Comparing Direct Oral Anticoagulants and Warfarin for Atrial Fibrillation, Venous Thromboembolism, and Mechanical Heart Valves. Consult Pharm 2015; 30: 644–656.
Sardar P, Chatterjee S, Chaudhari S, Lip GY . New oral anticoagulants in elderly adults: evidence from a meta-analysis of randomized trials. J Am Geriatr Soc 2014; 62: 857–864.
Mulligan R, Weitzel KG . Pretreatment management of the patient receiving anticoagulant drugs. J Am Dent Assoc 1988; 117: 479–483.
Wahl MJ . Dental surgery in anticoagulated patients. Arch Intern Med 1998; 158: 1610–1616.
Dunn AS, Turpie AG . Perioperative management of patients receiving oral anticoagulants: a systematic review. Arch Intern Med 2003; 163: 901–908.
Garcia DA, Regan S, Henault LE, et al. Risk of thromboembolism with short term interruption of warfarin therapy. Arch Intern Med 2008; 168: 63–69.
Schreuder WH, Peacock ZS . Antiplatelet therapy and exodontia. J Am Dent Assoc 2015; 146: 851–856.
Bajkin BV, Vujkov SB, Milekic BR, Vuckovic BA . Risk factors for bleeding after oral surgery in patients who continued using oral anticoagulant therapy. J Am Dent Assoc 2015; 146: 375–381.
Weltman NJ, Al-Attar Y, Cheung J, et al. Management of dental extractions in patients taking warfain as anticoagulant treatment: a systematic review. J Can Dent Assoc 2015; 81: f20
Broekema FI, van Minnen B, Jansma J, Bos RR . Risk of bleeding after dentoalveolar surgery in patients taking anticoagulants. Br J Oral Maxillofac Surg 2014; 52: e15-9
Author information
Authors and Affiliations
Additional information
Address for correspondence: Juan Xu, Department of Stomatology, Chinese People's Liberation Army General Hospital, 28 Fuxing Road, Beijing 100853, China. E-mail: newxj@hotmail.com
Yang S, Shi Q, Liu J, Xu J. Should oral anticoagulant therapy be continued during dental extraction? A meta-analysis. BMC Oral Health 2016; 16: 81.
Rights and permissions
About this article

Cite this article
Madeley, E., Duane, B. Oral anticoagulant therapy and tooth extraction, does the evidence support drug holidays?. Evid Based Dent 19, 53–54 (2018). https://doi.org/10.1038/sj.ebd.6401308
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401308
