
Abstract
Data sources
Medline, the Science Citation Index (SCI) via Web of Science, Scopus, CINAHL, Global Index Medicus, Google Scholar and SLT-related reports of the International Agency for Research on Cancer and the National Cancer Institute of the United States.
Study selection
Observational studies on the use of SLT and the risk of developing OPMDs in South Asian Populations.
Data extraction and synthesis
Duplicate selection of studies was undertaken with two reviewers undertaking data abstraction and quality assessment independently. Risk and odds ratios were extracted or calculated for studies where possible. Meta odds ratios (mOR) were calculated using a random effects analysis.
Results
Fifteen papers reporting 18 studies were included. The majority (12) were from India. All the studies were case-control designs. MOR for any OPMD with the use of any SLT product was 15.5 (95% CI; 9.9–24.2). Risk was higher in women; mOR = 22.2 (95% CI, 9.1–54.1) than men; mOR = 8.7 (95% CI, 2.1–34.8). Betel quid with tobacco carried the highest risk for OPMD, mOR = 16.1 (95% CI, 7.8–33.5).
Conclusions
The findings of our study point towards a strong association between some forms of OPMDs and SLT use in South Asia. The risk estimates are high, irrespective of controlling for confounders such as smoking and alcohol or stratification by sex, country or source of controls. There is also an exposure-response relationship between OPMDs and SLT use.
Similar content being viewed by others

Commentary
Oral cancer is ranked as the sixth most common malignancy in South Asia – with nearly 300,000 new cases diagnosed each year, accounting for one third of the total cancer burden in India.1 Tobacco and alcohol consumption are the most significant risk factors for oral cancer world-wide, however, in South Asia smokeless tobacco (SLT) accounts for a greater attributable risk.2 Smokeless tobacco is any form of tobacco consumed through the mouth or nose that does not involve burning the product – this includes betel quid, paan, gutkha, chewing tobacco and other such products. While only 1.6% of men and 0.5% of women in the United Kingdom use SLT,3 90% of SLT use is concentrated in South Asia3 with the practice viewed as being socially and culturally acceptable.4
Oral potentially malignant disorders (OPMDs) are clearly defined in this study as any chronic lesions/conditions found in the mouth that have the potential to transform into oral cancer;5 this includes: leukoplakia, erythroplakia, oral sub-mucous fibrosis (OSMF), lichen planus, actinic keratosis, discoid lupus erythematosus and palatal lesions among reverse smokers.6 The prevalence of OPMDs worldwide ranges from 1 to 5%;7 and their potential for them to undergo malignant transformation ranges from 1 to 36%, depending on the subtype of OPMD.8 This study seeks to quantify the risk associated with SLT use and the development of OPMDs in South Asia.6
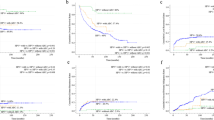
Fifteen articles corresponding to eighteen studies, pertaining to three of the seven countries in South Asia, were included in the meta-analysis. A substantial risk association between SLT use and OPMDs was estimated from the pooled data (meta odds ratio, mOR = 15.5; 95% CI, 9.9–24.2). The challenge in meta-analysis of published studies is taking into account confounders – analysis of the subgroup of studies here that had adjusted for smoking and alcohol found limited attenuation with a high-risk association remaining (mOR 13.1; 95% CI 8.3–20.7). OSMF was found to have the highest risk association with SLT use (mOR = 20.0; 95% CI, 12.3–32.5), and leukoplakia the lowest (mOR 4.33; 95% CI 1.4–13.2). Of the range of SLT products included, betel quid with tobacco carried the highest risk association for developing OPMDs (mOR = 16.1; 95% CI, 7.8–33.5); and women were found to have a higher risk association (mOR = 22.2; 95% CI, 9.1–54.1) than men (mOR = 8.7; 95% CI, 2.1–34.8).
Overall, this was a well conducted systematic review and meta-analysis conforming to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) reporting guidelines.9 The search strategy was thorough, but perhaps could also have included seeking unpublished data or contacting authors. The reviewers assessed the quality of the included studies using the National Collaborating Centre for Methods and Tools, McMaster University's ‘Effective Public Health Practice Project Quality Assessment Tool for Quantitative Studies’,6 and this identified one of the major limitations of this meta-analysis – ie the quality of included studies were either of moderate (n = 12) or weak (n = 6) quality;6 no studies were found to have strong qualities when assessed. Moreover, the quantification of SLT exposure in these studies was also identified by the authors as a problem and limitation – particularly the lack of a clear definition for ‘ever’ exposure may cause overestimation of the true risk, as an individual who has used SLT once was categorised in the same group as someone who used SLT for 20 years.7
This review is a good baseline description of the extent of epidemiological research into SLT and OPMD risk in South Asia. It points to the need for further research into this risk association, and indeed for the risk associations between SLT, OPMD and oral cancer. However, more importantly, it highlights the importance for research into SLT cessation in Asian populations and communities as a means to prevent oral cancer worldwide.
Change history
05 July 2017
Updated: This article was amended online on 5 July 2017 to correct a typo in the title. The original title incorrectly stated 'sobacco' instead of 'tobacco'.
References
Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 Cancer incidence and mortality worldwide: IARC CancerBase No. 11. Lyon, France: International Agency for Research on Cancer, 2013.
Siddiqi K, Shah S, Abbas SM, et al. Global burden of disease due to smokeless tobacco consumption in adults: analysis of data from 113 countries. BMC Med 2015; 13:194.
Sinha DN, Gupta PC, Ray C, Singh PK . Prevalence of smokeless tobacco use among adults in WHO South-East Asia. Indian J Cancer 2012; 49:342–346.
Bile KM, Shaikh JA, Afridi HU, Khan Y . Smokeless tobacco use in Pakistan and its association with oropharyngeal cancer. East Mediterr Health J 2010; 16:S24–S30.
Manne RK . Oral potentially malignant disorders/individuals. Oral Oncol 2014; 50:e7–e8.
Khan Z, Khan S, Christianson L, Rehman S, Ekwunife O, Samkange-Zeeb F . Smokeless Tobacco and Oral Potentially Malignant Disorder in South Asia: A Systematic Review and Meta-analysis. Nicotine Tob Res 2016; pii: ntw310. doi: 10.1093/ntr/ntw310. [Epub ahead of print]
Mortazavi H, Baharvand M, Mehdipour M . Oral potentially malignant disorders: an overview of more than 20 entities. J Dent Res Dent Clin Dent Prospects 2014; 8:6–14.
Warnakulasuriya S . Oral Submucous fibrosis: pathogenesis and presentation. Oral Oncol 2011; 47:S5
Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000; 283:2008–2012.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Zohaib Khan, MPH, Leibniz Institute for Prevention Research and Epidemiology-BIPS, Achterstrasse 30, 28359, Bremen, Germany. E-mail: khan@leibniz-bips.de
Khan Z, Khan S, Christianson L, Rehman S, Ekwunife O, Samkange-Zeeb F. Smokeless Tobacco and Oral Potentially Malignant Disorders in South Asia: A Systematic Review and Meta-analysis. Nicotine Tob Res 2016; pii: ntw310. doi: 10.1093/ntr/ntw310. [Epub ahead of print] Review. PubMed PMID: 27928050.
Rights and permissions
About this article

Cite this article
Seenan, P., Conway, D. Smokeless tobacco – a substantial risk for oral potentially malignant disorders in South Asia. Evid Based Dent 18, 54–55 (2017). https://doi.org/10.1038/sj.ebd.6401242
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401242
