
Abstract
The aim of this study was to assess whether adjuvant treatment of breast cancer (BC) affects the risk of stroke, and to explore radiation targets and fraction doses regarding risk and location of stroke. In a Swedish BC cohort diagnosed during 1970–2003, we carried out a nested case–control study of stroke after BC, with relevant details extracted from medical records. The odds ratio (OR) for radiotherapy (RT) vs that of no RT did not differ between cases and controls (OR=0.85; confidence interval, CI=0.6–1.3). Radiotherapy to internal mammary chain (IMC) and supraclavicular (SCL) lymph nodes vs that of no RT was associated with a higher, although not statistically significant, risk of stroke (OR=1.3; CI=0.8–2.2). In a pooled analysis, RT to IMC and SCL vs the pooled group of no RT and RT to breast/chest wall/axilla (but not IMC and SCL), showed a significant increase of stroke (OR=1.8; CI=1.1–2.8). There were no associations between cancer laterality, targets of RT, and location of stroke. The radiation targets, IMC and SCL, showed a statistically significant trend for an increased risk of stroke with daily fraction dose. Our finding of a target-specific increased risk of stroke and a dose-response relationship for daily fraction dose, indicate that there may be a causal link between RT to the IMC and SCL and risk of stroke.
Similar content being viewed by others

Main
Randomised clinical trials (Overgaard et al, 1997, 1999; Ragaz et al, 1997) and meta-analyses by the Early Breast Cancer Trialists' Collaborative Group (Clarke et al, 2005) have shown a benefit of post-operative radiotherapy (RT) in breast cancer (BC), by reducing local recurrences and BC deaths. On the other hand, there seems to be an excess of vascular deaths in women who were given RT (Clarke et al, 2005). Radiotherapy to the supraclavicular (SCL) lymph nodes includes the proximal part of the carotid artery in the photon field. Studies of head and neck cancer have shown an increased risk of carotid stenosis, followed by ischaemic stroke after RT (Cheng et al, 2000; Dorresteijn et al, 2002; Haynes et al, 2002).
Our earlier study (Nilsson et al, 2005) showed a statistically significant increase of 12% of stroke in a large BC cohort. Another study (Jagsi et al, 2006) found similar results, whereas two others did not (Hooning et al, 2006; Woodward et al, 2006). None of the last three studies showed a statistically significant increase of stroke among women given RT to the SCL.
In our case–control study, we aimed to assess whether any adjuvant treatment of BC, such as RT, tamoxifen, and chemotherapy, affects the risk of stroke, and to explore radiation targets and radiation fraction doses regarding risk and location of stroke.
Patients and methods
We conducted a case–control study of the first stroke after BC nested in a cohort of women with BC. The cohort comprises 4689 women with a first invasive BC diagnosed during 1970–2003 residing in Uppsala County, Sweden, at diagnosis and registered in the Swedish Cancer Register, which has 98% coverage (Mattsson and Wallgren, 1984). To identify stroke after BC, the cohort was linked, by Personal Registration Numbers, to the Swedish Hospital Discharge Register, containing all in-patient health care events. The definition of stroke was based on the International Classification of Disease (ICD) codes (Table 1). The ICD codes were grouped into the following subtypes: ischaemic stroke, cerebral haemorrhage, and ill-defined cerebrovascular lesion (Lawlor et al, 2002).
We found 316 eligible women with an invasive BC followed by hospitalisation for a stroke during the period 1970–2003, of whom 34 were excluded after record review, leaving 282 cases for analysis. The exclusion criteria were that a stroke could not be verified in the medical records, or that the medical records revealed a history of stroke also before the BC diagnosis. A total of 12 women were excluded, as they did not have an invasive BC, or as their BC was diagnosed before 1970.
For each case, one control was chosen by incidence density sampling (Rothman, 1998) ensuring that the probability of being chosen is proportional to the time at risk in the cohort. The control was sampled at random, among those who were alive and without a history of hospitalisation for a stroke at the date of the stroke, for the case. We refer to this date as index date for the controls. Cases were eligible as control subjects before their stroke event. We found a stroke diagnosis in two primarily selected controls before the index date. These patients were not in the risk set and, consequently, were not eligible as controls. In addition, 11 controls had no BC, or had BC diagnosed before 1970. For the 13 women, new controls were selected for each respective case by the same statistical method, leaving a total of 282 controls.
From the medical records we obtained information on BC, according to the International Union Against Cancer (UICC) TNM classification (6th edn) (tumour size, node status, presence of distant metastases, and laterality), and details of treatments.
With regard to RT, we collected information from the chart about target areas: remaining breast tissues after breast conserving surgery (BCS), chest wall after mastectomy, lymph nodes in the axilla, internal mammary chain (IMC), and SCL area. Data regarding daily fraction radiation doses and total doses were also collected. In respect of exposure to radiation, the subjects were separated into three groups: (1) no RT; (2) RT to breast/chest wall/axilla, but not to IMC/SCL; and (3) RT to IMC/SCL, irrespective of RT to other targets. In the following, we refer to these groups as: (1) ‘No RT’; (2) ‘RT except IMC/SCL’; and (3) ‘RT to IMC/SCL’.
During the study period 1970–2003, several different RT regimens have been used. The thoracic wall has been treated with low energy electrons during the whole period. The fraction schemes were: 3 Gy × 15=45 Gy (1970–1985), 2.3 Gy × 20=46 Gy (1986–1996), and thereafter 2 Gy × 25=50 Gy. Breast conserving surgery was started in the year of 1982 in our health care region. The remaining breast tissues were then treated with two opposed tangential photon fields 2 Gy × 27=54 Gy. From 1997 and further, the fractionation scheme was 2 Gy × 25=50 Gy.
The lymph nodes have been treated with different techniques and fractionation during this period. In the period 1970–1972, small–sized frontal Cobolt-60 photon fields to cover the SCL and IMC were given. One such small field of 7 Gy was given each day, and in consecutive days a chain of fields were given to cover the targets. The axilla was treated with photons (Cobolt-60), 4 Gy × 7 in a frontal field and 4 Gy × 6 in a dorsal field. In the period 1973–1976, IMC, SCL, and axilla were treated with a frontal Cobolt-60 photon field of 4 Gy × 10=40 Gy. The IMCs were treated simultaneously using a frontal field of electrons 3 Gy × 5=15 Gy, whereas the axilla was given 4 Gy × 4–5=20–24 Gy in a dorsal photon field.
In the period 1977–1985, IMC, SCL, and axilla were treated using a frontal Cobolt-60 photon field of 3.5 Gy × 9=31.5 Gy. The IMC and SCL were treated simultaneously using a frontal field of electrons 3 Gy × 5=15 Gy, whereas the axilla was given 4 Gy × 6=24 Gy in a dorsal photon field. In the 1986–1994 period, IMC, SCL, and axilla were treated using a frontal photon field of 2.5 Gy × 12=30 Gy. The IMC and SCL were treated simultaneously using a frontal field of electrons 2.5 Gy × 8=20 Gy, whereas the axilla was given 3.2 Gy × 8=25.6 Gy in a dorsal photon field.
In 1995 and after, treatment of the lymph nodes was dose planned, and all the included nodes were given 2 Gy × 27=54 Gy. In 1997 and later, the nodes were given 2 Gy × 25=50 Gy.
Information regarding adjuvant endocrine treatment (specified as tamoxifen or aromatase inhibitor), chemotherapy data (type of regimens and number of courses), and recurrences (local or distant) were abstracted from the medical records. For our stroke classification, we used all available information in the medical records, namely, medical history including clinical presentation, results of computed tomography (CT) scan and MRI, angiography, surgery reports, and autopsy records. We reviewed the records to decide whether the stroke was in the vertebrobasilar or carotid territories (Bamford et al, 1991). For carotid strokes, we also registered left or right hemisphere location. In the 32 cases, in which the classification and location was not obvious, two independent reviewers carried out a consensus evaluation, but this was still not possible in five of the cases. We registered the presence of atrial fibrillation, documented by electrocardiography, at the time of stroke among the cases.
Odds ratios (ORs) with 95% confidence intervals (CIs), in the 1 : 1 matched case–control study, were calculated using conditional logistic regression (Breslow and Day, 1980), adjusting for age in four categories (<60, 60–69, 70–79, and 80+ years) at BC diagnosis; this is done using Cox's regression (Cox, 1972). Tests of independence between laterality of BC and stroke for various RT regimens were carried out using Fisher's exact test. All statistical analyses were carried out using the statistical program package R (Ihaka, 1996).
Results
The characteristics of cases and controls are described in Table 2. Cases were significantly older. The mean age at BC diagnosis was 71.5 years (s.d., 11.0 years) for cases and 58.7 years (s.d., 13.2 years) for controls. The median follow-up period was 6.2 years (25th percentile 2.8 years; 75th percentile 11.0 years) for cases and 5.5 years (25th percentile 1.9 years; 75th percentile 9.3 years) for controls.
The cases had slightly more advanced cancers than the controls. Stage I cancer was more common among the controls. Only 1% of all subjects had distant metastasis at BC diagnosis with no difference between cases and controls. Less than 10% of the cases and controls had distant metastasis at the time of stroke or at the index date (controls). Furthermore, <5% of subjects had local recurrences at the time of stroke or at the index date. Cases and controls did not differ regarding incidence of local or distant recurrences.
Only four cases developed other cancers before their stroke, whereas controls did not. The cancers were non-Hodgkin lymphoma, ovarian cancer, small intestinal carcinoid tumour, and gastric cancer, respectively.
Almost 80% of the strokes originated in the carotid arteries and 20% in the vertebrobasilar system (Table 3). Computed tomography of the brain was carried out in 73% of the cases. Of these cases, 62% had ischaemic stroke, of which 48% had cerebral infarction and 14% had transient cerebral ischaemia. Ten percent of the cases had haemorrhagic stroke (2%, subarachnoidal haemorrhage and 8%, intracerebral haemorrhage). Of these cases, 28% had ill-defined stroke, mostly diagnosed in ‘the pre computer tomography era’, and 22% of the cases had atrial fibrillation at the time of their stroke.
We evaluated the relationship between stroke after BC and adjuvant treatments (Table 4). In the first analysis, not adjusted for age, we found no association between any BC treatment and stroke (data not shown). As the cases were significantly older than the controls, we adjusted the ORs for age. The overall OR for RT did not differ significantly from unity. However, as the analyses were stratified on RT type, differences emerged. Radiotherapy, except IMC/SCL compared with that of no RT was associated with a lower risk of stroke. Moreover, RT to IMC/SCL vs that of no RT was associated with a higher, although not significant, risk of stroke (OR=1.3; CI=0.8–2.2). When pooling the groups, no RT and RT, except IMC/SCL, a post hoc comparison of RT to IMC/SCL vs the pooled group showed a significant increase of stroke with an age-adjusted OR=1.8 and CI=1.1–2.8.
We also repeated the analyses stratifying on cerebral haemorrhage in one group (n=29) and ischaemic stroke plus ill-defined cerebrovascular lesion in another group (n=253); the latter showing a same pattern as for all types of stroke, and significantly increased risk of stroke among the subjects receiving RT to IMC/SCL vs that of no RT and RT, except IMC and SCL (OR=1.9; CI=1.2–3.2). No significant association between RT and haemorrhagic stroke was seen, although the CIs were wide.
Adjuvant tamoxifen was used by few women during the study period, that is ∼15% of the subjects, and the associated OR for stroke was as for chemotherapy below unity, but not in a statistically significant way.
Tamoxifen was used for either 2 or 5 years. Among the cases, 13/46 had tamoxifen for 2 years, whereas 33/46 had tamoxifen for 5 years. For the controls, the numbers were 10/43 and 33/43, respectively. Only one woman received an adjuvant aromatase inhibitor.
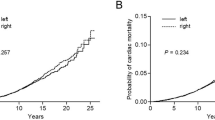
When investigating laterality, the analysis was restricted to cases with right or left carotid strokes, but no significant association was found between the BC laterality, targets of RT, and the location of the stroke (Table 5).
We further investigated dosage effects of RT, measured by the daily fraction dose, to different targets and risk of stroke (Table 6). The RT dosage administered to the remaining breast, after breast conservation, was standardised with very similar doses for all who were treated, thus a dose-response relation could not be evaluated (data not shown). However, for IMC and SCL, there was a significant trend for higher risk of stroke with increasing daily fraction dose, especially marked for high doses (⩾4 Gy).
Discussion
The main finding in our study is a statistically significant (OR=1.9) increase of stroke among women with BC, who had received RT to IMC and SCL. The risk was dose dependent and pertained to ischaemic and ill-defined stroke, but not to haemorrhagic stroke (although, we caution that the statistical precision for haemorrhagic stroke is low). There was no increased risk seen for the RT group as a whole or after exposure to hormonal treatment or chemotherapy. However, in the studied time period, few women were recommended for systematic adjuvant treatments.
This study is based on population-based registries with high coverage (Mattsson and Wallgren, 1984). This study covers a long period of follow-up. The medical records could be retrieved for virtually all cases and controls. We have no reason to believe that cases and controls were followed differently with respect to cerebral vascular disease.
The selection of controls followed standard incidence density-based sampling nested within a well-defined cohort (Rothman, 1998). We deliberately avoided matching for age, stage of disease, and time period of diagnosis, as indications and methods for RT are associated with these factors. Indeed, our findings indicate that such a matching would have entailed over-matching, and the risk of stroke may have been underestimated. Thus, we aimed to fulfil one of the basic methodological rules in a case–control study: the controls will be selected against criteria, which are not associated with a likelihood of or type of exposure.
Of all the strokes, ∼90% are ischaemic and 10% are haemorrhagic (Rothwell et al, 2005). This should also be true regarding ill-defined stroke. Thus, we deemed it appropriate to analyse ischaemic and ill-defined stroke together.
Of the cases, 22% had atrial fibrillation at the time of their stroke, corresponding well to epidemiological studies (Sandercock et al, 1992). We have no information on cardiovascular risk factors, such as hypertension, smoking, and hyperlipidaemia at the time of RT. However, if anything, it is likely that these factors are associated with more severe co-morbidity and, thus, may be associated with a contraindication for RT, thereby driving our estimates to the conservative side. For example, RT, which was not delivered to IMC and SCL, was associated with a lower risk of stroke that probably reflects a selection bias. There is no plausible biological explanation for RT to decrease the risk of stroke. Most women in this group underwent RT to the remaining breast after breast conservation; the reasons for avoiding RT after breast conservation, during this period, include a low-performance status and serious cardiovascular disease.
Given the possibility of selection bias mentioned above, we deem it likely that RT not delivered to IMC and SCL is associated with either low or no risk of stroke. Furthermore, we found no association between BC laterality and the corresponding hemisphere location of the carotid stroke. Thus, if there is a direct causal link between RT and stroke, we speculate that it is the dose to the superior part of the heart and the aortic arch (corresponding to the IMC radiation field) that is detrimental rather than the dose to the proximal part of the carotid artery (SCL radiation field). In that way, IMC radiation would increase the risk of atherosclerosis (Schultz-Hector and Trott, 2007) and, furthermore, thrombo-embolic stroke and embolus may follow the blood stream to either the right or left carotid artery, irrespective of BC laterality and SCL irradiation. However, we could not analyse the targets, IMC or SCL, as separate risk factors, as most subjects received RT to both targets combined. The distribution of stroke location is similar to that in epidemiological studies (Bamford et al, 1991), neither supporting, nor making a case against a causal explanation for RT as a risk factor for stroke.
In contrast to our findings, another study found a significant association between tamoxifen and stroke, but not between RT to SCL and stroke (Hooning et al, 2006). However, the subjects were ∼20 years younger, and the study group was restricted to 10-year BC survivors. In two studies (Jagsi et al, 2006; Woodward et al, 2006), there was no association between RT to SCL and stroke, but no information regarding RT to IMC was given. A recent study (Woodward et al, 2008) found no increase of carotid stenosis after radiation, measured by ultrasound.
Our result agrees with another study (Bowers et al, 2005), which showed a large increase of stroke, Relative Risk=4.3, among childhood Hodgkin survivors who had received mantle irradiation, involving IMC and SCL bilaterally. In keeping with our speculation that IMC radiation is detrimental, 50% of the Hodgkin survivors with stroke had concomitant heart or valve problems, predisposing to cardio-embolic stroke.
High daily fraction radiation doses increase the risk of late toxicity, such as myocardial infarction (Cuzick et al, 1994), lymph oedema, and brachial plexopathy (Johansson et al, 2002). Similarly, we found a dose-dependent relationship between radiation dose to IMC and SCL and stroke (Table 6). It is difficult to compare old RT techniques with modern techniques, as generally hypo fraction was used in the former. When using the older techniques no dose planning was used, implicating an increased risk of radiation exposure to other organs in the mediastinum, namely, the heart and the aortic arch and its branches. Furthermore, the radiation volumes were larger and the dose homogeneity was poorer.
Taken together, our earlier finding of a 12% increased risk of stroke in relative terms after BC diagnosis (Nilsson et al, 2005), the present target-specific increased risk of a stroke, a dose-response relationship for daily fraction dose, and a suggestion of an increased risk of ischaemic stroke, indicate that there may be a causal relationship between RT to the IMC and SCL and risk of stroke. Together with other studies, our findings indicate that an increased risk of stroke has to be taken into consideration in view of giving RT to IMC or SCL. The ongoing randomised European Organisation for Research and Treatment of Cancer (EORTC) study regarding RT to IMC will provide important data regarding that risk; however, these effects will take a long time to appear.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Bamford J, Sandercock P, Dennis M, Burn J, Warlow C (1991) Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet 337: 1521–1526
Bowers DC, McNeil DE, Liu Y, Yasui Y, Stovall M, Gurney JG, Hudson MM, Donaldson SS, Packer RJ, Mitby PA, Kasper CE, Robison LL, Oeffinger KC (2005) Stroke as a late treatment effect of Hodgkin's disease: a report from the Childhood Cancer Survivor Study. J Clin Oncol 23: 6508–6515
Breslow NE, Day NE (1980) Statistical methods in cancer research. Volume I – The analysis of case-control studies. IARC Sci Publ 248–278
Cheng SW, Ting AC, Lam LK, Wei WI (2000) Carotid stenosis after radiotherapy for nasopharyngeal carcinoma. Arch Otolaryngol Head Neck Surg 126: 517–521
Clarke M, Collins R, Darby S, Davies C, Elphinstone P, Evans E, Godwin J, Gray R, Hicks C, James S, MacKinnon E, McGale P, McHugh T, Peto R, Taylor C, Wang Y (2005) Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet 366: 2087–2106
Cox DR (1972) Regression models and life-tables. J R Stat Soc B 34: 187–202
Cuzick J, Stewart H, Rutqvist L, Houghton J, Edwards R, Redmond C, Peto R, Baum M, Fisher B, Host H, Lythgoe J, Ribeiro G, Scheurlen H (1994) Cause-specific mortality in long-term survivors of breast cancer who participated in trials of radiotherapy. J Clin Oncol 12: 447–453
Dorresteijn LD, Kappelle AC, Boogerd W, Klokman WJ, Balm AJ, Keus RB, van Leeuwen FE, Bartelink H (2002) Increased risk of ischemic stroke after radiotherapy on the neck in patients younger than 60 years. J Clin Oncol 20: 282–288
Haynes JC, Machtay M, Weber RS, Weinstein GS, Chalian AA, Rosenthal DI (2002) Relative risk of stroke in head and neck carcinoma patients treated with external cervical irradiation. Laryngoscope 112: 1883–1887
Hooning MJ, Dorresteijn LD, Aleman BM, Kappelle AC, Klijn JG, Boogerd W, van Leeuwen FE (2006) Decreased risk of stroke among 10-year survivors of breast cancer. J Clin Oncol 24: 5388–5394
Ihaka R, Gentleman R (1996) R: a language for data analysis and graphics. J Comput Graph Stat 5: 299–314
Jagsi R, Griffith KA, Koelling T, Roberts R, Pierce LJ (2006) Stroke rates and risk factors in patients treated with radiation therapy for early-stage breast cancer. J Clin Oncol 24: 2779–2785
Johansson S, Svensson H, Denekamp J (2002) Dose response and latency for radiation-induced fibrosis, edema, and neuropathy in breast cancer patients. Int J Radiat Oncol Biol Phys 52: 1207–1219
Lawlor DA, Smith GD, Leon DA, Sterne JA, Ebrahim S (2002) Secular trends in mortality by stroke subtype in the 20th century: a retrospective analysis. Lancet 360: 1818–1823
Mattsson B, Wallgren A (1984) Completeness of the Swedish Cancer Register. non-notified cancer cases recorded on death certificates in 1978. Acta Radiol Oncol 23: 305–313
Nilsson G, Holmberg L, Garmo H, Terent A, Blomqvist C (2005) Increased incidence of stroke in women with breast cancer. Eur J Cancer 41: 423–429
Overgaard M, Hansen PS, Overgaard J, Rose C, Andersson M, Bach F, Kjaer M, Gadeberg CC, Mouridsen HT, Jensen MB, Zedeler K (1997) Postoperative radiotherapy in high-risk premenopausal women with breast cancer who receive adjuvant chemotherapy. Danish Breast Cancer Cooperative Group 82b Trial. N Engl J Med 337: 949–955
Overgaard M, Jensen MB, Overgaard J, Hansen PS, Rose C, Andersson M, Kamby C, Kjaer M, Gadeberg CC, Rasmussen BB, Blichert-Toft M, Mouridsen HT (1999) Postoperative radiotherapy in high-risk postmenopausal breast-cancer patients given adjuvant tamoxifen: Danish Breast Cancer Cooperative Group DBCG 82c randomised trial. Lancet 353: 1641–1648
Ragaz J, Jackson SM, Le N, Plenderleith IH, Spinelli JJ, Basco VE, Wilson KS, Knowling MA, Coppin CM, Paradis M, Coldman AJ, Olivotto IA (1997) Adjuvant radiotherapy and chemotherapy in node-positive premenopausal women with breast cancer. N Engl J Med 337: 956–962
Rothman KJ (1998) Case-Control Studies. Modern Epidemiology. Lippincott-Raven: Philadelphia
Rothwell PM, Coull AJ, Silver LE, Fairhead JF, Giles MF, Lovelock CE, Redgrave JN, Bull LM, Welch SJ, Cuthbertson FC, Binney LE, Gutnikov SA, Anslow P, Banning AP, Mant D, Mehta Z (2005) Population-based study of event-rate, incidence, case fatality, and mortality for all acute vascular events in all arterial territories (Oxford Vascular Study). Lancet 366: 1773–1783
Sandercock P, Bamford J, Dennis M, Burn J, Slattery J, Jones L, Boonyakarnkul S, Warlow C (1992) Atrial fibrillation and stroke: prevalence in different types of stroke and influence on early and long term prognosis (Oxfordshire community stroke project). BMJ 305: 1460–1465
Schultz-Hector S, Trott KR (2007) Radiation-induced cardiovascular diseases: is the epidemiologic evidence compatible with the radiobiologic data? Int J Radiat Oncol Biol Phys 67: 10–18
Woodward WA, Durand JB, Tucker SL, Strom EA, Perkins GH, Oh J, Arriaga L, Domain D, Buchholz TA (2008) Prospective analysis of carotid artery flow in breast cancer patients treated with supraclavicular irradiation 8 or more years previously: no increase in ipsilateral carotid stenosis after radiation noted. Cancer 112: 268–273
Woodward WA, Giordano SH, Duan Z, Hortobagyi GN, Buchholz TA (2006) Supraclavicular radiation for breast cancer does not increase the 10-year risk of stroke. Cancer 106: 2556–2562
Acknowledgements
This study was supported by grants from the Research Fund of the Department of Oncology, Uppsala University Hospital, the Lions Cancer Foundation, and the Erik, Karin and Gösta Selander Foundation.
Author information
Authors and Affiliations
Corresponding author
Additional information
Conflict of interest
The authors declare no conflicts of interest.
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Nilsson, G., Holmberg, L., Garmo, H. et al. Radiation to supraclavicular and internal mammary lymph nodes in breast cancer increases the risk of stroke. Br J Cancer 100, 811–816 (2009). https://doi.org/10.1038/sj.bjc.6604902
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6604902
Keywords
This article is cited by
-
Adapting and implementing breast cancer follow-up in primary care: protocol for a mixed methods hybrid type 1 effectiveness-implementation cluster randomized study
BMC Primary Care (2023)
-
Breast cancer survivorship: state of the science
Breast Cancer Research and Treatment (2018)
-
Unplanned irradiation of internal mammary lymph nodes in breast cancer
La radiologia medica (2017)
-
The Marmot report: accepting the poisoned chalice
British Journal of Cancer (2013)
-
Lokalisation von Koronarstenosen nach Strahlentherapie wegen Mammakarzinom
Strahlentherapie und Onkologie (2012)
