
Abstract
Stress plays an important role in psychiatric disorders, and preclinical evidence indicates that the central endocannabinoid system modulates endocrine and neuronal responses to stress. This study aimed to investigate the effect of acute stress on circulating concentrations of endocannabinoids (eCBs) in healthy humans. A total of 71 adults participated in two sessions in which they were exposed to either a standardized psychosocial stress procedure (Trier Social Stress Test) or a control task. Blood samples for eCB and cortisol assays and cardiovascular and subjective measures were obtained before and at regular intervals after the tasks. Serum concentrations of the eCBs, N-arachidonylethanolamine (anandamide, AEA) and 2-arachidonoylglycerol (2-AG), as well as of the N-acylethanolamides (NAEs), N-palmitoylethanolamine (PEA) and N-oleoylethanolamine (OEA), and of the O-acylglycerol, 2-oleoylglycerol (2-OG), were determined. Compared with the control condition, stress increased serum concentrations of AEA and the other NAEs immediately after the stress period. Increases in PEA were positively correlated with increases in serum cortisol after stress. Furthermore, anxiety ratings at baseline were negatively correlated with baseline concentrations of AEA. The sex and menstrual cycle status of the subject affected the NAE responses to stress. Interestingly, subjects of Asian and African-American races exhibited different patterns of stress responses compared with the Caucasian subjects. These results indicate that stress increases circulating NAEs in healthy human volunteers. This finding supports a protective role for eCBs in anxiety. Further research is needed to elucidate the function of these lipid mediators, and to determine the mechanisms that regulate their appearance in the circulation.
Similar content being viewed by others
INTRODUCTION
Stress contributes to somatic and psychiatric disorders such as depression, anxiety, and substance abuse (Esler et al, 2008; Krishnan and Nestler, 2008; Parker et al, 2003; Sinha, 2008). Acute stress activates the hypothalamic–pituitary–adrenal (HPA) axis, leading to release of glucocorticoids such as cortisol (Lopez et al, 1999; Chrousos et al, 2009), and the sympathetic-adrenomedullary system (SAM), leading to secretion of catecholamines (Lopez et al, 1999; Chrousos et al, 2009). Recent preclinical evidence indicates that stress also mobilizes the endocannabinoid (eCB) system in both the brain and the periphery, and that the eCB system can modulate behavioral and endocrine responses to both acute and chronic stress (Hill et al, 2010; Patel and Hillard, 2008). In the current study, we examined the effects of acute stress on serum concentrations of eCBs and their structural analogs in healthy human volunteers.
The eCB system consists of two functionally identified endogenous ligands, N-arachidonylethanolamine (anandamide, AEA) and 2-arachidonoylglycerol (2-AG) (Di Marzo et al, 2005). AEA as well as the structurally analogous lipids N-palmitoylethanolamine (PEA) and N-oleoylethanolamine (OEA) belong to the family of N-acylethanolamines (NAEs) (Ueda et al, 2010), whereas 2-AG and its structural analog 2-oleoylglycerol (2-OG) belong to the family of O-acylglycerols (Sugiura et al, 2006). PEA, OEA, and 2-OG do not target the CB1 or CB2 receptors, although they share some metabolic processes with their eCB family members (Di Marzo et al, 2005; Ho and Hillard, 2005).
In the central nervous system (CNS), eCBs are thought to be synthesized ‘on demand’ in response to increased neuronal excitation (Kano et al, 2009). After being released into the synapse, eCBs act in a retrograde manner to activate presynaptic CB1 receptors to inhibit neurotransmitter release (Patel and Hillard, 2009). Both of the eCBs and their congeners are also present in the serum and plasma (Wood et al, 2008). Immune cells, endothelial cells, adipocytes, and visceral organs have the ability to synthesize and release eCBs to the blood and have been proposed to serve as sources of circulating eCBs (Cote et al, 2007; Di Marzo et al, 1999; McCarron et al, 2006); it is also possible that the eCBs in the circulation reflect overflow from the brain (Hillard et al, 2012). The function of circulating eCBs is not fully understood. Correlational studies suggest that circulating eCBs exert hemodynamic (Randall et al, 2007; Wagner et al, 1997), immunomodulatory (O’Sullivan and Kendall, 2010), metabolic (Di Marzo et al, 2009), and reproductive (Taylor et al, 2010) effects in humans. Recent studies in women with depression showed that circulating concentrations of AEA correlate with emotional variables (Hill et al, 2008), suggesting that circulating eCBs reflect and could contribute to emotional responses. Peripheral eCB concentrations are increased during labor (Habayeb et al, 2004), and circulating peripheral eCBs are increased immediately after parabolic flights in subjects without motion sickness, but not in subjects with motion sickness (Chouker et al, 2010).
The current study was designed to investigate the effects of an acute psychosocial stressor (Trier Social Stress Task (TSST); Kirschbaum et al, 1993a) on serum concentrations of eCBs and structural analogs in healthy volunteers compared with a control condition. The study used a within-subject design with both stress and no stress conditions to lessen interindividual differences. We hypothesized that serum concentrations of eCBs and their structural analogs would increase after stress and would be correlated with other indicators of stress, including serum cortisol, cardiovascular measures, and feelings of anxiety.
In addition, we examined the effects of sex and menstrual cycle phase in stress-induced serum concentrations of eCBs and their structural analogs. These analyses were based upon earlier findings that these factors contribute to individual differences in responses to stress. For example, Kirschbaum et al (1999) reported that, during the TSST, men exhibited significantly higher ACTH responses than women in either cycle phase, and men showed significantly higher salivary free cortisol concentrations than women in the follicular phase. Men also exhibit larger blood pressure responses after psychosocial stress than women (Lepore et al, 1993; Matthews et al, 2001). In line with these findings, our group previously reported that men exhibited greater increases in serum cortisol after undergoing the TSST than women (Childs et al, 2010). In addition, luteal-phase women showed greater stress-induced increases in heart rate and anxiety than follicular-phase women (Childs et al, 2010).
Our sample was heterogeneous with respect to race, and published work led us to carry out a secondary analysis of race as a factor in response to the TSST. Chong et al (2008) showed that HPA axis activation (ie, cortisol concentrations) during the TSST was greater in Caucasians than in people of African descent. Social anxiety disorder, generalized anxiety, and panic disorder are more common in Caucasians than African Americans (Asnaani et al, 2010). Thus, in this study we conducted exploratory analyses with sex, menstrual cycle, and race as possible factors in eCB response to acute stress.
PATIENTS AND METHODS
Subjects
Healthy volunteers (N=71; 48 women, 23 men), aged 18–32 years, were recruited via posters and advertisements. They underwent a semistructured psychiatric screening interview, completed a psychiatric symptom checklist (SCL-90) (Derogatis, 1983), the Michigan Alcoholism Screening Test (Selzer, 1971), a health questionnaire with a detailed section on current and lifetime drug use, and they received a physical examination including an electrocardiogram. Volunteers were excluded if they consumed more than three cups of coffee per day, had a body mass index (BMI) outside the range of 18–26 kg/m2, took any regular medication (including hormonal contraceptives or exogenous hormones), and had any serious medical condition (defined by the US Centers for Disease Control and Prevention) such as cardiovascular diseases including hypertension, gastroenterological diseases including liver or kidney dysfunction, or any neurological conditions. Subjects with a lifetime diagnosis of an Axis I disorder including panic disorder, generalized anxiety disorder, bipolar disorder, major depressive disorder, psychotic symptoms, or lifetime substance dependence or current abuse (American Psychiatric Association, 1994) were excluded from the study. However, specific phobias, lifetime alcohol abuse, dysthymia, or personality disorders were not exclusionary. Subjects were excluded if they were not fluent in English; had less than a high school education; or worked the night shift. Women with irregular cycle lengths or severe premenstrual affective symptoms within 3 months preceding the study were excluded. Cigarette smokers were excluded as smoking is known to alter response to the TSST (Childs and de Wit, 2010; Kirschbaum et al, 1993b).
Design
The study used a randomized, two-session crossover design with a stress session (TSST) and a no stress session (control). Each subject participated in both experimental sessions, which occurred at least 48 h apart. This study was approved by the institutional review board of The University of Chicago for the use of human subjects and by the institutional review board of the Medical College of Wisconsin for the serum lipid analyses. The study was conducted in accordance with the Helsinki Declaration of 1975.
Procedure
Participants attended an orientation in which they provided consent and practiced answering the questionnaires. Subjects were specifically instructed not to take any drugs including alcohol and nicotine and not to use any medication, including over-the-counter medications, for 24 h before each session. Women were randomly assigned to participate during either the follicular or luteal phase of the menstrual cycle. Follicular sessions were scheduled between days 3 and 10 of the menstrual cycle, using the first day of menstruation as day 1. Luteal sessions were scheduled 2 to 10 days after a positive urine ovulation test. The stress and no stress sessions were scheduled within 7 days so that women could participate in both experimental sessions within a single cycle phase.
Subjects were tested individually in a comfortable patient room at the University of Chicago Hospital's General Clinical Research Center (GCRC). To standardize sleeping and eating, subjects were admitted to the GCRC at 2100 h the night before each session. Subjects were awakened at 0730 h and had a standard breakfast at 0800 h including their usual amount of caffeine. After breakfast, they provided breath and urine samples to exclude recent use of drugs including alcohol and nicotine. At 0830 h, an intravenous catheter with a clave connector was placed in the nondominant arm of the participants for collection of blood samples. Heparin flushes were used to keep the catheter open. Heart rate was monitored continuously beginning at 0900 h, using a chest band (Mini-Logger). At 0940 h, baseline blood samples were obtained to determine concentrations of eCBs, eCB-like compounds, and serum cortisol. At the same time, blood pressure and mood measures were obtained.
At 0950 h, the experimenter read the standardized TSST instructions (Kirschbaum et al, 1993a) or the control instructions to the participant. After the 10 min preparation period, participants were escorted to an adjacent room for the tasks at 1000 h. During the TSST, participants gave their 5 min mock job interview and 5 min oral arithmetic in front of two unsmiling ‘examiners,’ with a clear view of their own image on a television monitor. During the control task, subjects spoke with a friendly research assistant about neutral topics including interests and hobbies. After the procedures (10 min), subjects were escorted back to the patient room. Blood samples were obtained and blood pressure was measured immediately (0.5 min) and at 5, 10, 20, 30, 60, 90, and 120 min after the tasks. Participants also completed mood questionnaires immediately and at 10, 20, 30, 60, 90, and 120 min after completing the tasks. At the end of the second session, participants were debriefed about the study and received payment.
Dependent Measures
The primary outcome measures in this study were serum concentrations of two eCBs (AEA and 2-AG) and three structural analogs (PEA, OEA, and 2-OG). These compounds will be referred to in aggregate as ‘lipids.’ Lipids were obtained before and immediately after the tasks (baseline, 0.5 min). Unfortunately, because of technical problems, we were not able to accurately measure and therefore not able to include lipid concentrations at later time points (5, 10, 20, 30, 60, 90, and 120 min). Secondary measures were serum cortisol concentrations, and cardiovascular and subjective measures obtained before and at repeated times after the tasks (baseline, 0.5, 5, 10, 20, 30, 60, 90, and 120 min). The direct effects of the TSST on these secondary measures have been reported previously (Childs et al, 2010). We also examined serum cortisol, heart rate, systolic blood pressure, and feelings of anxiety in relation to concentration of the lipids, as these secondary measures are known to interact with the eCB system (Hill et al, 2009a; Kunos et al, 2000; Gorzalka et al, 2008).
Lipid Measurement
Following collection, blood samples were immediately refrigerated and then centrifuged. Serum was stored at −80 °C until analyses. Lipid extraction from serum was performed by solid-phase extraction as previously described (Hill et al, 2008). Briefly, serum (0.5 ml) was loaded onto conditioned solid-phase extraction columns (Bond Elut C18; Varian) and washed with 5 ml of deionized water. Columns were eluted with 1 ml ethyl acetate, dried under N2 gas, and lipids were resuspended in 20 μl methanol. Lipids of interest were analyzed by liquid chromatography-electrospray ionization-mass spectrometry (LC-ES-MS; Agilent LC-MSD 1100 series) and quantified by isotope dilution as described previously (Patel et al, 2005b). Samples (5 μl) were separated on a reverse-phase C18 column (Kromasil, 250 × 2 mm, 5 μm diameter; Phenomenex) using stationary phase A (deionized water with 0.005% acetic acid, 1 mM ammonium acetate) and mobile phase B (methanol with 0.005% acetic acid, 1 mM ammonium acetate). Samples were eluted at 300 μl/min flow rate by linear gradient (Solvent B increasing from 85 to 90% over 15 min, then 90–100% over 5 min, then held at 100% for 10 min). Selective ion monitoring was used to detect positive ions [2H8] AEA (m/z 356; retention time=12.4 min), AEA (m/z 348; retention time=12.6 min), PEA (m/z 300; retention time=16.1 min), OEA (m/z 326; retention time=17.0 min), 2-OG and 1,3-OG (m/z 357; retention time=18.4 and 19.4 min, respectively), [2H8] 2-AG and [2H8] 1,3-AG (m/z 387; retention times=13.1 and 14.1 min, respectively), and 2-AG and 1,3-AG (m/z 379; retention times=13.3 and 14.3 min, respectively). Because 2-AG isomerizes to 1,3-AG during storage and extraction (Stella et al, 1997), the area of both peaks was combined to yield total 2-AG. There was a contaminant peak that intervened between the 1,3-AG and 2-AG peaks in the serum samples. Therefore, the peaks for the two arachidonoyl glycerol esters were always identified using the migration times obtained from chromatographs of standards and in comparison with migration times for deuterated 2-AG within the same sample.
Cortisol
Blood samples for cortisol analyses were immediately refrigerated, and then centrifuged and stored at −80 °C. The GCRC Core Laboratory at the University of Chicago determined the levels of cortisol using a chemiluminescent technology (Immulite 1000 Cortisol; Siemens Healthcare Diagnostics, Deerfield, IL, USA; sensitivity=0.20 μg/dl). The immune cortisol assay kits were processed by an automatic clinical platform. The test units contained an assay-specific coated bead for specific binding and used chemiluminescent quantifications for precise hormone measurements. Sample and reagent were pipetted into a test unit. Following incubation, test units were spun at high speed to expel fluid into the integral sump chamber. Then, chemiluminescent substrate was added to the test unit after many washes, removing unbound material from the bead and inner tube. Finally, light emission was read with a high-sensitivity photon counter to perform precise measurement.
Cardiovascular Measures
Heart rate was recorded continuously using polar chest band monitors (Mini-Logger, Mini Mitter/Respironics, Bend, OR, USA). Blood pressure was measured at repeated intervals using a Critikon Dinamap Plus Vital Signs Monitor (GE Healthcare Technologies, Waukesha, WI, USA). In this investigation we focused on continuous heart rate and systolic blood pressure, given that both are valid measures of the effects of acute stress on the cardiovascular system and, in particular, on the circulation. Peripheral endocannabinoids are known to modulate cardiovascular processes such as blood pressure and vasoconstriction (Kunos et al, 2000).
Subjective Measures
To assess subjective effects of stress, subjects completed the standardized questionnaire Profile of Mood States (POMS) (Johanson and Uhlenhuth, 1980) at regular intervals. The POMS measures momentary mood states on eight primary scales (eg, Anger, Anxiety, and Confusion). Because the eCB system is implicated in anxiety (Hill et al, 2009a; Gorzalka et al, 2008), we utilized the POMS Anxiety scale as our main measure of subjective responses to stress.
Statistical Analyses
First, baseline differences between stress and no stress conditions were evaluated for all outcome measures using one-way analysis of variance (ANOVA). There were no significant differences between the two sessions on any measure. The influences of demographic measures such as gender and cycle phase, race, age, BMI, cannabis use frequency, and session order on the outcome measures at baseline were assessed using ANOVA or Pearson's bivariate correlation analyses.
Second, the main effects of stress on primary and secondary outcome measures were investigated using one-way repeated measures ANOVAs (stress vs no stress). Analogous to the analyses of the lipids, we used the values of heart rate, blood pressure, serum cortisol, and Anxiety obtained at baseline and immediately after (0.5 min) the tasks. For continuous heart rate data, mean heart rates during 10-min periods at baseline and during the tasks were used. Comparing concentrations at baseline and immediately after the tasks provided a good index of the peak stress effect for the secondary outcome measures (Figure 1). Change from baseline values (see graphs) were calculated by subtracting values obtained immediately after the tasks from respective values at baseline. Possible confounding variables on the main effects of stress (age, BMI, cannabis use frequency, and session order) were assessed by performing separate analyses of covariance (ANCOVAs) and considered in further statistical analyses. Influences of race, gender, and cycle phase were separately considered in further analyses, and subanalyses were carried out in subgroups of Caucasian, African-American, and Asian subjects, as well as in male participants and follicular and luteal female participants.

Time course of the secondary outcome measures anxiety (a), serum cortisol (b), systolic blood pressure (c), and heart rate (d: bpm refers to beats per minute). To assess the main effect of stress on secondary outcome measures, repeated-measures ANOVAs were performed comparing changes from baseline (−20-min time point) in the no stress and stress sessions (ANOVA; ***p<0.001).
Third, we used Pearson's bivariate correlations and partial correlations to assess relationships between concentrations of lipids and levels of cortisol, heart rate, blood pressure, and Anxiety. First, to estimate stable individual differences in these measures in the absence of stress, we used baseline concentrations from the second session to minimize variability related to the novelty of the first session. To examine correlations between the measures in response to stress, we performed bivariate correlations between stress-induced changes in lipid concentrations and stress-induced changes of cortisol, heart rate, blood pressure, and Anxiety. In this analysis, a single value of stress response was calculated for each variable as follows: first, the change from baseline to 0.5 min values (Cfbl) was determined for both the stress and no stress conditions; second, the effect of stress was calculated as the difference between these values for each individual (Cfbl Stress−Cfbl No Stress).
Repeated measures ANOVAs were performed with Greenhouse–Geisser correction when violations of sphericity were detected. We did not correct our primary measures for multiple comparisons because serum concentrations of the lipids are highly correlated among each other, and hence do not represent independent multiple tests. Subjective, cardiovascular, and hormonal responses to stress are expected to reflect separate and independent underlying processes. Thus, α was set at p<0.05 (two tailed) for the analyses of main stress effects on the outcome measures.
Subanalyses were corrected for multiple testing with Bonferroni–Holm corrections using the α threshold p=0.0166 for statistical significance. Correlational analyses were corrected for multiple testing using Bonferroni–Holm corrections according to the number of outcome measures examined using a p-value of 0.0125 for statistical significance.
RESULTS
Demographic Characteristics
Table 1 shows the demographic characteristics of the overall sample (N=71). Participants were 18–32 years old (mean: 21.51, SEM±0.43), 62% were of European American descent. Most of the subjects were college students (66.2%). None of the subjects were daily cigarette smokers, although 11.3% smoked at less frequent intervals. The subjects were light social drinkers (mean drinks per week: 2.56±0.38) and they consumed on average 5 cups of coffee per week (mean cups per week: 5.38±0.668). Approximately one-quarter (25.4%) of the subjects consumed marijuana recreationally (mean cigarettes per month for users only: 2.32±0.47), and none of the subjects were daily marijuana users. Approximately half of the subjects (56.3%) had tried marijuana at least once in their lifetime. These levels of use are typical for this age group (http://monitoringthefuture.org/). There were no significant correlations between cannabis use frequency and lipid concentrations at baseline (bivariate Pearson's correlation) or after stress (Supplementary Tables S1 and S2). There were no significant associations between age, BMI or session order and lipid concentrations at baseline or lipid concentrations after stress (one-way ANOVA, bivariate Pearson's correlation). There were no baseline differences between stress and no stress sessions (one-way ANOVA) for any of the outcome measures and no effects of session order.
Main Effect of Stress on Subjective, Cardiovascular, and Cortisol Response
As described previously (Childs et al, 2010), the TSST significantly increased serum cortisol concentrations (one-way ANOVA; p=0.003, F(1, 69)=9.326), systolic blood pressure (one-way ANOVA; p=0.00005, F(1, 70)=18.36), heart rate (one-way ANOVA; p=0.00003, F(1, 45)=21.35), and self-reports of Anxiety (one-way ANOVA; F(1, 70)=49.93; p=10−9). Figure 1 shows the time course of the secondary outcome measures for the first 30 min after the stress and no stress task as changes from baseline. Supplementary Table S3 shows baseline levels of the outcome measures for stress and no stress sessions for all subjects and different race groups. Supplementary Figure S1 shows the raw cortisol data for the first 30 min after the stress and no stress tasks.
Main Effect of Stress on Circulating Lipids
To assess the main effect of stress on circulating lipids, repeated measures ANOVAs were performed comparing changes from baseline to 0.5 min between the no stress and stress sessions (Figure 2). Stress significantly increased serum concentrations of AEA (one-way ANOVA; p=0.003, F(1, 67)=9.27), PEA (one-way ANOVA; p=0.0004, F(1, 68)=13.63), and OEA (one-way ANOVA; p=0.003, F(1, 68)=9.8). Serum concentrations of 2-AG and 2-OG were increased over baseline during both sessions; however, neither change reached statistical significance. There was no difference in the change from baseline values for 2-AG and 2-OG between the stress and no stress session. Overall, the concentrations of 2-AG (Supplementary Figure S2) and 2-OG were highly variable among individuals.

Serum concentrations as changes from baseline after the no stress (NS) and stress (S) procedures are presented for AEA (a), PEA (b), OEA (c), 2-AG (d), and 2-OG (e). To assess the main effects of stress on circulating lipids, repeated-measures ANOVAs were performed comparing changes from baseline in the no stress and stress sessions (*p<0.05; **p<0.01; ***p<0.001).
Exploratory Subanalyses of Caucasian, African-American, and Asian Participants
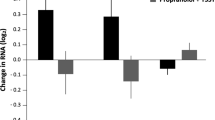
As our sample was racially mixed, we performed exploratory subanalyses of the effects of stress on lipids in Caucasian (N=44; male: N=14, female: N=30), African-American (N=15; male: N=4, female: N=11), and Asian participants (N=12; male: N=5, female: N=7). Interestingly, the findings of the overall sample could be accounted for by responses among Caucasians only (Figure 3). Caucasians showed significant differences between the no stress and stress session in changes from baseline of AEA (two-way ANOVA; p=0.002, F(1, 41)=10.42), PEA (two-way ANOVA; p=0.0003, F(1, 42)=15.58), and OEA (two-way ANOVA; p=0.0003, F(1, 42)=15.53). There was no significant increase over baseline in any of the lipids in either the no stress or stress condition in African-American or Asian subjects.

Serum concentrations as changes from baseline after the no stress and stress procedures presented among subgroups of Caucasian, African-American, and Asian subjects; the lipids measured are AEA (a), PEA (b), OEA (c), 2-AG (d), and 2-OG (e). Repeated-measures ANOVAs were performed comparing changes from baseline in the no stress and stress sessions (**p<0.01; ***p<0.001).
Stress significantly increased Anxiety in Caucasians (one-way ANCOVA; p=0.002, F(1, 42)=11.52) and African Americans (one-way ANCOVA; p=0.00009, F(1, 15)=13.00) but not in Asians. Stress significantly increased systolic blood pressure in Caucasians (one-way ANOVA; p=0.013; F(1, 43)=6.66) and African Americans (one-way ANOVA; p=0.005; F(1, 14)=10.86), heart rate in Caucasians only (one-way ANOVA; p=0.013; F(1, 30)=17.92), and serum cortisol in Caucasians (one-way ANOVA; p=0.008; F(1, 42)=7.68) and Asians (one-way ANOVA; p=0.038; F(1, 11)=5.53) (Supplementary Figure S3). Although Caucasians displayed the most robust responses to stress among the groups, stress significantly affected African Americans and Asians on some of the secondary outcome measures. Except for the increase of serum cortisol in Asians, all findings remained significant after adjustment for multiple testing.
Baseline raw data of lipids and secondary outcome measures for different race groups are shown in Supplementary Table S3. There were modest differences in baseline self-reported anxiety in the no stress session between race groups (Asians>Caucasians>African Americans, one-way ANOVA: p=0.002, F(2, 70)=6.30). Thus, anxiety levels at baseline were included as covariates in relevant analyses. The three different racial groups did not differ significantly at baseline on other outcome measures or on demographic measures except age (African Americans mean age 23.67 years (SEM±1.06), Caucasians 21.30 years (SEM±0.55), and Asians 19.58 years (SEM±0.43 Age did not influence the lipid response to stress in the sample.
Exploratory Subanalyses of Males, and of Females Tested During Follicular and Luteal Phases
Sex and menstrual cycle phase are known to influence responses to stress (Childs et al, 2010). Therefore, we performed subanalyses comparing men (N=23), and women in the luteal phase (N=26) and in the follicular phase (N=22). These subanalyses indicated that stress increased PEA in follicular women (one-way ANOVA; p=0.05, F(1, 21)=4.32) and luteal women (one-way ANOVA; p=0.047, F(1, 24)=4.37) and in men (one-way ANOVA: p=0.028, F(1, 21)=5.54), and increased AEA concentrations in men (one-way ANOVA; p=0.047, F(1, 21)=4.44; Figure 4). However, none of these findings remained significant after adjustment for multiple testing.

Serum concentrations as changes from baseline after the no stress and stress procedures presented among subgroups of men, luteal, and follicular women; the lipids measured are AEA (a), PEA (b), OEA (c), 2-AG (d), and 2-OG (e). Repeated-measures ANOVAs were performed comparing changes from baseline in the no stress and stress sessions (*p<0.05).
As reported previously (Childs et al, 2010), stress significantly increased Anxiety in all subgroups of subjects (follicular: one-way ANOVA; p=0.0002, F(1, 21)=19.56; luteal: one-way ANOVA; p=0.0002, F(1, 25)=19.82; male: one-way ANOVA; p=0.002, F(1, 22)=12.52). In men, stress increased serum cortisol (one-way ANOVA; p=0.010, F(1, 22)=7.96) and stress increased heart rate and systolic blood pressure in luteal women and in men (heart rate: luteal: one-way ANOVA; p=0.002, F(1, 17)=13.15; men: one-way ANOVA; p=0.006, F(1, 12)=10.70; systolic blood pressure: luteal: one-way ANOVA; p=0.045, F(1, 25)=4.46; men: one-way ANOVA; p=0.001, F(1, 22)=14.30; Supplementary Figure S4). Except for the stress-mediated increase in systolic blood pressure among luteal women, the findings remained significant after adjustment for multiple testing. The subgroups of men, follicular women, and luteal women did not differ at baseline or on any of the investigated demographic measures.
Correlation Analyses
We performed correlation analyses using pretask data from the second session to investigate the relationship between pretask baseline concentrations of PEA, AEA, 2-AG, and 2-OG, and baseline cortisol, heart rate, blood pressure, and Anxiety. The baseline concentrations of AEA were negatively correlated with feelings of Anxiety (r=−0.294, p=0.014), which remained significant after adjustment for multiple testing (Figure 5). There were no other significant correlations between baseline concentrations of the lipids and other outcome measures.

Scatterplots showing correlations between pretask baseline (BL: second session) concentrations of the N-acylethanolamines and anxiety. The three panels show correlations between pretask baseline concentrations of Anxiety and pretask baseline concentrations of (a) AEA, (b) PEA, and (c) OEA (*p<0.05).
Correlation analyses were performed using bivariate Pearson's correlation to assess associations of stress-induced changes in circulating concentrations of the lipids with stress-induced changes in cortisol, heart rate, blood pressure, and Anxiety. The increase in circulating PEA following the stress session was positively correlated with serum cortisol concentrations after the stress task (r=0.37, p=0.002; Figure 6). This correlation remained significant after adjustment for multiple testing. The 2-OG, but not 2-AG, concentrations were positively correlated with feelings of Anxiety after stress (r=0.28, p=0.027; Supplementary Figure S5), which was not significant after adjustment for multiple testing. Blood pressure and heart rate after stress were not correlated with any of the investigated lipids (Supplementary Figure S6).

Scatterplots showing correlations between stress-induced concentrations of the N-acylethanolamines and stress-induced cortisol concentrations. The three panels show correlations between stress-induced cortisol concentrations and stress-induced concentrations of (a) AEA, (b) PEA, and (c) OEA. Values are derived by subtracting no-stress session values from stress session values (**p<0.01, Cfbl: change from baseline).
To further investigate a possible impact of low vs high AEA basal concentrations on stress response, we conducted a median split in the baseline AEA concentration to divide the sample into high and low prestress groups. There was a trend for subjects with lower AEA concentrations at baseline to show higher cortisol release after stress compared with subjects with higher AEA concentrations at baseline (two-way ANOVA, group × condition interaction, p=0.051, F(1, 66)=3.94). The high and low baseline AEA groups did not significantly differ on any other measures of stress response.
DISCUSSION
The major finding of the study is that acute psychosocial stress significantly increased serum concentrations of all three NAEs examined. This finding is consistent with other preclinical evidence that the eCB system is involved in the response to acute stress (Gorzalka et al, 2008). There was a significant, positive correlation between stress-induced increase in PEA concentration and the amount of circulating cortisol at 30 s following the end of stress. Preclinical studies indicate that peripheral glucocorticoid concentrations after stress are correlated with reduced AEA concentrations in stress-responsive regions of the brain (Patel et al, 2004, 2005a; Rademacher et al, 2008; Hill et al, 2009b). eCBs and their structural analogs are able to cross the blood brain barrier (Willoughby et al, 1997; Glaser et al, 2006). Although it is possible that Circulating NAEs represent overflow of the lipids from the brain following stress, these preclinical studies indicate that stress causes a reduction in brain NAEs. The source of circulating NAEs, particularly during stress, is an important question that remains to be answered.
There was a trend for subjects with lower AEA concentrations at baseline to show greater increases in cortisol after stress, compared with participants with higher AEA concentrations at baseline. These data are interesting and suggest that baseline eCB tone regulates HPA axis reactivity to stress. A similar relationship was observed in two earlier studies: in the first, baseline circulating concentrations of AEA were inversely correlated with motion sickness in response to parabolic flights (Chouker et al, 2010) and, in the second, baseline concentrations of AEA affected reflex responses to orthostatic stress (Schroeder et al, 2009). Thus, these studies indicate that, in addition to being stress reactive, circulating eCBs also contribute to the magnitude of the stress response.
Circulating concentrations of AEA were negatively associated with Anxiety at baseline. Although these data are correlational and do not demonstrate causality, the finding is robust and suggests the hypothesis that high concentrations of AEA in the circulation are protective against anxiety. This is in agreement with a clinical study (Hill et al, 2008) as well as with findings in nonhuman models, in which inhibition of AEA metabolism has anxiolytic and antidepressant effects (Bambico et al, 2007; Naidu et al, 2007). Furthermore, the anxiolytic agent, diazepam, increases AEA in the amygdala, and bromazepam and buspirone have diminished anxiolytic effects in CB1-knockout mice (Micale et al, 2009; Uriguen et al, 2004). In humans, the synthetic cannabinoid nabilone significantly reduces nightmares and flashbacks in patients with posttraumatic stress disorder (Fraser, 2009). Thus, the serum content of AEA might be a potential biomarker for both anxiety and depression. These data provide further support for the notion that inhibition of AEA catabolism could be a potential target for treating anxiety and anxiety-related psychiatric disorders.
The relative concentrations of AEA, PEA, and OEA in the circulation (PEA>OEA>AEA) parallel the relative concentrations of these lipids in the brain (Patel et al, 2005b) and likely reflect the proportion of palmitic, oleic, and arachidonic acids in the N-acyl position of the precursor of the NAEs, N-acyl-phosphatidylethanolamine (NAPE; Ueda et al, 2010). AEA, PEA, and OEA have overlapping but not identical biosynthetic and catabolic mechanisms (Ueda et al, 2010; Tsuboi et al, 2007). All three NAEs are substrates of fatty acid amide hydrolase (FAAH), with AEA being the best substrate of the three (Ueda et al, 1995). A second NAE hydrolysis enzyme, N-acylethanolamine-hydrolyzing acid amidase (NAAA), has been identified that is found in lysosomes and has an acidic pH and preferentially acts on PEA as a substrate (Tsuboi et al, 2007). The current study does not provide insights into the enzymatic processes responsible for the changes in circulating NAEs in response to stress. However, FAAH-knockout mice as well as mice treated with a FAAH inhibitor accumulate AEA but not 2-AG in response to stress (Gaetani et al, 2009). Thus, decreased FAAH activity might be responsible for mediating the observed parallel increase of all three NAEs but not of O-acylglycerols in response to stress.
Although the increase in AEA concentration coincided with the peak increase in heart rate and blood pressure, AEA concentration was not correlated with measures of sympathetic nervous system (SNS) activation. However, it is possible that the relationship between SNS activity and AEA in the circulation is very dynamic or outside the sensitivity of our measurements. Our measurement of SNS activity and AEA concentrations were made 30 s after the stress session, and hence it is possible that this is too late to determine the relationships between these responses. There was also no significant correlation between AEA and cortisol concentrations.
Unexpectedly, stress did not increase circulating concentrations of 2-AG. This is in contrast to the findings of Hill et al (2009a), who found that circulating 2-AG was higher immediately following social stress exposure than before exposure in 15 women. However, the study of Hill et al (2009a) did not include a no stress control condition, but instead reported an increase compared with prestress baseline. In our study, circulating concentrations of 2-AG and 2-OG tended to increase immediately after both the control and stress task, although they did not reach significance in either case. For unknown reasons, there was a high individual variability in 2-AG and 2-OG concentrations in the present study, which could have masked a significant stress effect on these compounds. Alternatively, peripheral 2-AG and 2-OG might not be specifically involved in response to stressful or threatening situations, but instead could be responsive to interactions or external change without regard to the salience of the situation.
We observed some individual differences in biochemical measures before and after the stress. Men exhibited greater changes from baseline in each of the NAEs compared with women, and women in the luteal phase tended to respond more strongly than women in the follicular phase. Interestingly, the increase in AEA after stress only reached statistical significance in men in subanalyses. The lack of a significant change in women is in accord with the study of Hill et al (2009a); they observed that all three NAEs increased slightly, but did not reach statistical significance following exposure of women to stress. We found interesting differences among the three racial groups represented in our sample; specifically, stress increased the NAEs but not the secondary outcome measures in Caucasians only. The finding of a possible racial difference in response to stress is consistent with several other reports of race differences (Ahwal et al, 1997; Chong et al, 2008; Sherwood et al, 1995).
There are several important limitations of this study. First, we did not obtain information about current stress levels, temperament or trait anxiety, or about the participants’ exposure to early life stress, trauma, or early-life adversity. It is known that early-life mistreatment can affect responses to stress later in life, and thus early-life stress may have been an important source of individual variability in the present study (Dannlowski et al, 2012). In particular, early-life trauma could interact with either race or sex, and thus contribute to some of the individual differences reported here. It will be of interest to determine in future studies whether exposure to early childhood stressors influences the eCB responses to acute stress in adulthood. Second, our 2-AG spectra were contaminated by a peak that migrated between 2-AG and 1,3-AG. We did not include this peak in the integrations; however, its presence could have contributed to the variability in 2-AG measurements. Third, our analysis of lipids in sera obtained at various time points during the stress recovery period were confounded by the time between blood draws. We suspect that the use of heparin to flush the catheters between draws was the problem. Studies are on-going to establish this mechanism.
In conclusion, our data provide evidence that the eCB system is involved in response to acute psychosocial stress in healthy humans. Our findings are consistent with other findings suggesting that eCBs and related lipids may be useful as diagnostic agents of stress-related psychiatric disorders (Hill et al, 2009c). Future studies are needed to characterize the nature of the lipid response, including its time course and reactivity to other forms of stress. It will also be important to use other outcome measures like functional imaging or genetic analyses to understand the physiological role of the lipids, and develop their potential in psychiatric treatment.
References
Ahwal WN, Mills PJ, Kalshan DA, Nelesen RA (1997). Effects of race and sex on blood pressure and hemodynamic stress response as a function of the menstrual cycle. Blood Press Monit 2: 161–167.
American Psychiatric Association (1994). Diagnostic and Statistical Manual of Mental Disorders, 4th edn. American Psychiatric Press: Washington, DC.
Asnaani A, Richey JA, Dimaite R, Hinton DE, Hofmann SG (2010). A cross-ethnic comparison of lifetime prevalence rates of anxiety disorders. J Nerv Ment Dis 198: 551–555.
Bambico FR, Katz N, Debonnel G, Gobbi G (2007). Cannabinoids elicit antidepressant-like behavior and activate serotonergic neurons through the medial prefrontal cortex. J Neurosci 27: 11700–11711.
Childs E, de Wit H (2010). Effects of acute psychosocial stress on cigarette craving and smoking. Nicotine Tob Res 12: 449–453.
Childs E, Dlugos A, De Wit H (2010). Cardiovascular, hormonal, and emotional responses to the TSST in relation to sex and menstrual cycle phase. Psychophysiology 47: 550–559.
Chong RY, Uhart M, McCaul ME, Johnson E, Wand GS (2008). Whites have a more robust hypothalamic-pituitary-adrenal axis response to a psychological stressor than blacks. Psychoneuroendocrinology 33: 246–254.
Chouker A, Kaufmann I, Kreth S, Hauer D, Feuerecker M, Thieme D et al (2010). Motion sickness, stress and the endocannabinoid system. PLoS One 5: e10752.
Chrousos GP, Kino T, Charmandari E (2009). Evaluation of the hypothalamic-pituitary-adrenal axis function in childhood and adolescence. Neuroimmunomodulation 16: 272–283.
Cote M, Matias I, Lemieux I, Petrosino S, Almeras N, Despres JP et al (2007). Circulating endocannabinoid levels, abdominal adiposity and related cardiometabolic risk factors in obese men. Int J Obes (Lond) 31: 692–699.
Dannlowski U, Stuhrmann A, Beutelmann V, Zwanzger P, Lenzen T, Grotegerd G et al (2012). Limbic scars: long-term consequences of childhood maltreatment revealed by functional and structural magnetic resonance imaging. Biol Psychiatry 71: 286–293.
Derogatis L (1983). SCL-90-R Manual II. Clinical Psychometric Research: Towson, MD.
Di Marzo V, Bisogno T, De Petrocellis L, Melck D, Orlando P, Wagner JA et al (1999). Biosynthesis and inactivation of the endocannabinoid 2-arachidonoylglycerol in circulating and tumoral macrophages. Eur J Biochem 264: 258–267.
Di Marzo V, De Petrocellis L, Bisogno T (2005). The biosynthesis, fate and pharmacological properties of endocannabinoids. Handb Exp Pharmacol 168: 147–185.
Di Marzo V, Ligresti A, Cristino L (2009). The endocannabinoid system as a link between homoeostatic and hedonic pathways involved in energy balance regulation. Int J Obes (Lond) 33 (Suppl 2): S18–S24.
Esler M, Eikelis N, Schlaich M, Lambert G, Alvarenga M, Kaye D et al (2008). Human sympathetic nerve biology: parallel influences of stress and epigenetics in essential hypertension and panic disorder. Ann NY Acad Sci 1148: 338–348.
Fraser GA (2009). The use of a synthetic cannabinoid in the management of treatment-resistant nightmares in posttraumatic stress disorder (PTSD). CNS Neurosci Ther 15: 84–88.
Gaetani S, Sipasquale P, Romano A, Righetti L, Cassano T, Piomelli D et al (2009). The endocannabinoid system as a target for novel anxiolytic and antidepressant drugs. Int Rev Neurolbiol 85: 57–72.
Glaser ST, Gatley SJ, Gifford AN (2006). Ex vivo imaging of fatty acid amide hydrolase activity and its inhibition in the mouse brain. J Pharmacol Exp Ther 316: 1088–1097.
Gorzalka BB, Hill MN, Hillard CJ (2008). Regulation of endocannabinoid signaling by stress: implications for stress-related affective disorders. Neurosci Biobehav Rev 32: 1152–1160.
Habayeb OM, Taylor AH, Evans MD, Cooke MS, Taylor DJ, Bell SC et al (2004). Plasma levels of the endocannabinoid anandamide in women--a potential role in pregnancy maintenance and labor? J Clin Endocrinol Metab 89: 5482–5487.
Hill MN, Hillard CJ, Bambico FR, Patel S, Gorzalka BB, Gobbi G (2009c). The therapeutic potential of the endocannabinoid system for the development of a novel class of antidepressants. Trends Pharmacol Sci 30: 484–493.
Hill MN, McLaughlin RJ, Morrish AC, Viau V, Floresco SB, Hillard CJ et al (2009b). Suppression of amygdalar endocannabinoid signaling by stress contributes to activation of the hypothalamic–pituitary–adrenal axis. Neuropsychopharmacology 34: 2733–2745.
Hill MN, Miller GE, Carrier EJ, Gorzalka BB, Hillard CJ (2009a). Circulating endocannabinoids and N-acyl ethanolamines are differentially regulated in major depression and following exposure to social stress. Psychoneuroendocrinology 34: 1257–1262.
Hill MN, Miller GE, Ho WS, Gorzalka BB, Hillard CJ (2008). Serum endocannabinoid content is altered in females with depressive disorders: a preliminary report. Pharmacopsychiatry 41: 48–53.
Hill MN, Patel S, Campolongo P, Tasker JG, Wotjak CT, Bains JS (2010). Functional interactions between stress and the endocannabinoid system: from synaptic signaling to behavioral output. J Neurosci 30: 14980–14986.
Hillard CJ, Weinlander KM, Stuhr KL (2012). Contributions of endocannabinoid signaling to psychiatric disorders in humans: genetic and biochemical evidence. Neuroscience 204: 207–299.
Ho WS, Hillard CJ (2005). Modulators of endocannabinoid enzymic hydrolysis and membrane transport. Handb Exp Pharmacol 168: 187–207.
Johanson CE, Uhlenhuth EH (1980). Drug preference and mood in humans: diazepam. Psychopharmacology (Berl) 71: 269–273.
Kano M, Ohno-Shosaku T, Hashimotodani Y, Uchigashima M, Watanabe M (2009). Endocannabinoid-mediated control of synaptic transmission. Physiol Rev 89: 309–380.
Kirschbaum C, Kudielka BM, Gaab J, Schommer NC, Hellhammer DH (1999). Impact of gender, menstrual cycle phase, and oral contraceptives on the activity of the hypothalamus-pituitary-adrenal axis. Psychosom Med 61: 154–162.
Kirschbaum C, Pirke KM, Hellhammer DH (1993a). The ‘Trier Social Stress Test’--a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology 28: 76–81.
Kirschbaum C, Strasburger CJ, Langkrar J (1993b). Attenuated cortisol response to psychological stress but not to CRH or ergometry in young habitual smokers. Pharmacol Biochem Behav 44: 527–531.
Krishnan V, Nestler EJ (2008). The molecular neurobiology of depression. Nature 455: 894–902.
Kunos G, Jarai Z, Batkai S, Goparaju SK, Ishac EJ, Liu J et al (2000). Endocannabinoids as cardiovascular modulators. Chem Phys Lipids 108: 159–168.
Lepore SJ, Allen KA, Evans GW (1993). Social support lowers cardiovascular reactivity to an acute stressor. Psychosom Med 55: 518–524.
Lopez JF, Akil H, Watson SJ (1999). Neural circuits mediating stress. Biol Psychiatry 46: 1461–1471.
Matthews KA, Gump BB, Owens JF (2001). Chronic stress influences cardiovascular and neuroendocrine responses during acute stress and recovery, especially in men. Health Psychol 20: 403–410.
McCarron RM, Chen Y, Tomori T, Strasser A, Mechoulam R, Shohami E et al (2006). Endothelial-mediated regulation of cerebral microcirculation. J Physiol Pharmacol 57 (Suppl 11): 133–144.
Micale V, Cristino L, Tamburella A, Petrosino S, Leggio GM, Drago F et al (2009). Anxiolytic effects in mice of a dual blocker of fatty acid amide hydrolase and transient receptor potential vanilloid type-1 channels. Neuropsychopharmacology 34: 593–606.
Naidu PS, Varvel SA, Ahn K, Cravatt BF, Martin BR, Lichtman AH (2007). Evaluation of fatty acid amide hydrolase inhibition in murine models of emotionality. Psychopharmacology (Berl) 192: 61–70.
O’Sullivan SE, Kendall DA (2010). Cannabinoid activation of peroxisome proliferator-activated receptors: potential for modulation of inflammatory disease. Immunobiology 215: 611–616.
Parker KJ, Schatzberg AF, Lyons DM (2003). Neuroendocrine aspects of hypercortisolism in major depression. Horm Behav 43: 60–66.
Patel S, Carrier EJ, Ho WS, Rademacher DJ, Cunningham S, Reddy DS et al (2005b). The postmortal accumulation of brain N-arachidonylethanolamine (anandamide) is dependent upon fatty acid amide hydrolase activity. J Lipid Res 46: 342–349.
Patel S, Cravatt BF, Hillard CJ (2005a). Synergistic interactions between cannabinoids and environmental stress in the activation of the central amygdala. Neuropsychopharmacology 30: 497–507.
Patel S, Hillard CJ (2008). Adaptations in endocannabinoid signaling in response to repeated homotypic stress: a novel mechanism for stress habituation. Eur J Neurosci 27: 2821–2829.
Patel S, Hillard CJ (2009). Endocannabinoids as modulators of synaptic signaling. In: Reggio PH (ed). The Cannabinoid Receptors. Humana Press: New York, pp 281–308.
Patel S, Roelke CT, Rademacher DJ, Cullinan WE, Hillard CJ (2004). Endocannabinoid signaling negatively modulates stress-induced activation of the hypothalamic-pituitary-adrenal axis. Endocrinology 145: 5431–5438.
Rademacher DJ, Meier SE, Shi L, Ho WS, Jarrahian A, Hillard CJ (2008). Effects of acute and repeated restraint stress on endocannabinoid content in the amygdala, ventral striatum, and medial prefrontal cortex in mice. Neuropharmacology 54: 108–116.
Randall MD, Kendall DA, Bennett AJ, O’Sullivan SE (2007). Rimonabant in obese patients with type 2 diabetes. Lancet 369: 555.
Schroeder C, Batkai S, Engeli S, Tank J, Diedrich A, Luft FC et al (2009). Circulating endocannabinoid concentrations during orthostatic stress. Clin Auton Res 19: 343–346.
Selzer ML (1971). The Michigan alcoholism screening test: the quest for a new diagnostic instrument. Am J Psychiatry 127: 1653–1658.
Sherwood A, May CW, Siegel WC, Blumenthal JA (1995). Ethnic differences in hemodynamic responses to stress in hypertensive men and women. Am J Hypertens 8: 552–557.
Sinha R (2008). Chronic stress, drug use, and vulnerability to addiction. Ann NY Acad Sci 1141: 105–130.
Stella N, Schweitzer P, Piomelli D (1997). A second endogenous cannabinoid that modulates long-term potentiation. Nature 388: 773–778.
Sugiura T, Kishimoto S, Oka S, Gokoh M (2006). Biochemistry, pharmacology and physiology of 2-arachidonoylglycerol, an endogenous cannabinoid receptor ligand. Prog Lipid Res 45: 405–446.
Taylor AH, Amoako AA, Bambang K, Karasu T, Gebeh A, Lam PM et al (2010). Endocannabinoids and pregnancy. Clin Chim Acta 411: 921–930.
Tsuboi K, Takezaki N, Ueda N (2007). The N-acylethanolamine-hydrolyzing acid amidase (NAAA). Chem Biodivers 4: 1914–1925.
Ueda N, Kurahashi Y, Yamamoto S, Tokunaga T (1995). Partial purification and characterization of the porcine brain enzyme hydrolyzing and synthesizing anandamide. J Biol Chem 270: 23823–23827.
Ueda N, Tsuboi K, Uyama T (2010). Enzymological studies on the biosynthesis of N-acylethanolamines. Biochim Biophys Acta 1801: 1274–1285.
Uriguen L, Perez-Rial S, Ledent C, Palomo T, Manzanares J (2004). Impaired action of anxiolytic drugs in mice deficient in cannabinoid CB1 receptors. Neuropharmacology 46: 966–973.
Wagner JA, Varga K, Ellis EF, Rzigalinski BA, Martin BR, Kunos G (1997). Activation of peripheral CB1 cannabinoid receptors in haemorrhagic shock. Nature 390: 518–521.
Willoughby KA, Moore SF, Martin BR, Ellis EF (1997). The biodisposition and metabolism of anandamide in mice. J Pharmacol Exp Ther 282: 243–247.
Wood JT, Williams JS, Pandarinathan L, Courville A, Keplinger MR, Janero DR et al (2008). Comprehensive profiling of the human circulating endocannabinoid metabolome: clinical sampling and sample storage parameters. Clin Chem Lab Med 46: 1289–1295.
Acknowledgements
This research was supported by grants from the National Institute on Drug Abuse (DA022439, DA02812, and MO1RR00055). We thank Patricia Kriegel and Ana Asiama for technical assistance and Drs Royce Lee and Karran Phillips for medical support. We offer many thanks to the participants.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest. Dr de Wit has received support from Unilever for an unrelated research project.
Additional information
Supplementary Information accompanies the paper on the Neuropsychopharmacology website
Supplementary information
Rights and permissions
About this article
Cite this article
Dlugos, A., Childs, E., Stuhr, K. et al. Acute Stress Increases Circulating Anandamide and Other N-Acylethanolamines in Healthy Humans. Neuropsychopharmacol 37, 2416–2427 (2012). https://doi.org/10.1038/npp.2012.100
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/npp.2012.100
Keywords
This article is cited by
-
Endocannabinoids, endocannabinoid-like compounds and cortisone in head hair of health care workers as markers of stress and resilience during the early COVID-19 pandemic
Translational Psychiatry (2024)
-
Sex differences in neuroendocrine, sympathetic nervous system, and affect responses to acute stress in cannabis users
Psychopharmacology (2023)
-
Acquisition of threat responses are associated with elevated plasma concentration of endocannabinoids in male humans
Neuropsychopharmacology (2022)
-
Effects of cycling workstation to get tertiary employee moving on their overall health: study protocol for a REMOVE trial
Trials (2021)
-
The endocannabinoid system in humans: significant associations between anandamide, brain function during reward feedback and a personality measure of reward dependence
Neuropsychopharmacology (2021)
