
Abstract
The pharmaceutical industry has targeted various types of molecules to subdue inflammatory diseases. Drugs that disrupt cell migration appear particularly promising in clinical trials and in many animal models of inflammatory disease. Cell migration inhibitors not only interfere with migration of cells to a tissue, but also can affect other necessary processes such as mediator release and angiogenesis. However, the question is whether drugs that target adhesion molecules or chemoattractant receptors will prove superior to drugs that target other molecular types. This review proclaims the virtues of targeting cell migration–related molecules for development of new anti-inflammatory and anti-tumor based drugs. It is likely that cell migration inhibitors will transform the way in which many human inflammatory diseases and cancers are treated.
Similar content being viewed by others


Main
Despite the many billions of dollars that have been spent on immunological research, few effective anti-inflammatory drugs have emerged. An urgent need for new drugs exists, as many inflammatory diseases are inadequately responsive to current medications. Moreover, in developed countries, the incidence of some inflammatory diseases, such as asthma, has increased markedly over recent decades. The incidence of some autoimmune diseases, including type 1 diabetes, is also on the rise, further suggestive of links between inflammatory diseases and aspects of modern lifestyles1. The challenge for the development of new anti-inflammatory drugs has been to find appropriate targets that are essential in the inflammatory process but are mostly dispensable for host defense against pathogens.
The development of several new drugs is poised to revolutionize the treatment of inflammatory diseases. Therapeutics that selectively alter cell migration represent a particularly promising class of the new anti-inflammatory drugs. The basis for this optimism rests on several recent developments. The first is the proven efficacy of the first migration-inhibitory drug to be approved, the anti–α4 integrin monoclonal antibody (mAb) natalizumab (Tysabri). This agent represents a breakthrough for the treatment of multiple sclerosis and Crohn's disease, by limiting T cell migration to an inflamed tissue, such as the central nervous system in multiple sclerosis. A second development has been the discovery of the many cell migration molecules required for development of different inflammatory responses and the demonstration in animal models that targeting these is a highly effective way to ameliorate inflammation. Finally, after a slow start, the pharmaceutical industry has developed potent and selective small molecule as well as mAb inhibitors for most of the important cell migration molecules, particularly the chemoattractant receptors. While adhesion molecules, such as the integrins, have generally been targeted by protein based drugs such as mAbs, chemoattractant receptors are G protein–coupled receptors (GPCRs) that are generally amenable to inhibition by organic small molecule drugs. The ability to take them orally makes small molecule inhibitors the drug of choice, yet mAbs also offer some distinct advantages.
Intervention points for cell migration inhibitors
Leukocyte extravasation usually occurs through a multistep process, involving first the selectins, then chemoattractant receptor signaling, followed by firm adhesion to vessel walls through the actions of integrins (Fig. 1). Thereafter, leukocytes migrate along chemotactic gradients, by means of chemoattractant receptor signaling and the actions of adhesion molecules, particularly integrins. Each of the molecular participants in this process—selectins, chemoattractants and integrins—has a fundamental and sequential role, such that inhibition of any given selectin, chemoattractant receptor or integrin could effectively inhibit leukocyte extravasation entirely. Selectin or integrin adhesion molecules are few, whereas the number of chemokines and other chemoattractants suggest that these latter molecules must be prominent in dictating the precise placement of leukocyte subsets. For instance, many of the functional subsets of T cells express the α4 integrin uniformly, but they differentially express a range of chemoattractant receptors such as CCR5, CCR6 and CXCR5. This provides opportunities, as well as pitfalls. If a drug targets a cell migration molecule too selectively, it might be ineffective.If it inhibits too broadly, it might be too immunocompromising.

Points 1–3 involve the multistep adhesion cascade of leukocyte binding to endothelium. Chemoattractants (green dots) signal chemoattractant GPCRs such as chemokine receptors or C5aR, leading to integrin activation and firm adhesion. Chemoattractants also attract leukocytes through tissues (point 4) and stimulate leukocytes to release inflammatory mediators such as histamine and proteases (point 5). An associated feature of many inflammatory responses is angiogenesis, in which chemokines are important (point 6). Finally, leukocyte egress from tissues, particularly lymphoid tissues, is regulated by S1P receptors (point 7), and stimulation of S1P receptors can limit the migration through blood and tissues by pathogenic T cells. At present, there are many drugs in preclinical and clinical development that target one or more of these points (Table 1). Selectin inhibitors operate at point 1; integrin inhibitors may operate at points 1, 3 and 4; chemoattractant receptor inhibitors operate at points 2, 4, 5 and 6; and S1P receptor–based drugs such as FTY-720 operate at point 7.
Chemoattractant signaling is usually an essential event during the multistep process of leukocyte rolling and transendothelial migration. Consequently, inhibitors of many chemoattractants or their receptors have proven to be highly effective anti-inflammatory agents in a range of animal models of inflammation (see reviews by refs. 2, 3, 4, 5). However, inhibitors of the integrins and selectins have also proven to be highly effective in animal models of inflammation and in human disease. A second point at which a cell migration inhibitor may limit the inflammatory response is disruption of normal cell placement within a tissue. For instance, in human asthma, epithelial cell elaboration of eotaxins attracts eosinophils, which can subsequently damage airway epithelium6. CCR3 deficiency in mice does not prevent the binding of eosinophils to endothelium, but does result in their arrest in the subendothelial space and failure to traverse airway tissue7. Chemoattractants do much more than simply facilitate cell movement. The proinflammatory effects of chemokines or anaphylatoxins such as C5a derive from the release of inflammatory mediators by mast cells, macrophages and neutrophils, including substances such as histamine, myeloperoxidase and proteases (Fig. 1). Inflammatory responses often result in new blood vessel growth, and certain chemokines are important in stimulating vessel growth. Finally, chemoattractant receptors also regulate leukocyte retention within a tissue (Fig. 1). Manipulation of leukocyte retention by drugs such as FTY-720 is proving to be a successful approach for retaining T cells in lymphoid tissues, thereby limiting their migration to inflammatory lesions.
Some examples of the most advanced cell migration–based drugs in development (or approved) for inflammatory diseases are listed in Table 1. Drug developers now have a diverse range of candidate molecular targets to alter cell migration for the treatment of inflammation or cancer. Cell migration inhibitors can generally be divided into four classes. Three of these represent the three types of molecules involved in cell migration and adhesion: the selectins and their receptors, the chemoattractants and their receptors, and the integrins and their receptors (Fig. 1). A fourth class includes the signaling molecules downstream from adhesion or chemoattractant receptors, such as phosphoinositide-3-OH kinase-γ (PI(3)K-γ). The diversity of adhesion molecules and chemoattractant receptors, and their restriction to particular subsets of leukocytes, offers the possibility for selective inhibition of leukocytes—for instance, a leukocyte type implicated in the pathogenesis of disease. Various effector T cell subsets have been implicated in the pathogenesis of different autoimmune or allergic diseases. Likewise, mast cells, neutrophils and eosinophils, which tend to be considered in the context of innate immunity, can act as potent effector cells during inflammatory responses associated with adaptive immunity. The following sections outline many of the promising cell migration targets for subsets of T cells and other effector leukocytes.
Selectin inhibitors
Leukocyte tethering and rolling, mediated usually by three selectins (L-selectin, P-selectin and E-selectin), are the first steps in the process of leukocyte binding to vascular endothelium (Fig. 1). L-selectin is involved in the homing of T cells to lymphoid tissues but is also expressed on other leukocyte types, where it participates in inflammation. E-selectin is expressed selectively on skin endothelium, whereas P-selectin is expressed on inflamed endothelium and by certain leukocytes. Expression of both E- and P-selectins is regulated by inflammatory stimuli. P-selectin glycoprotein ligand-1 (PSGL-1) is a mucin-like glycoprotein that binds P-selectin, as well as L- and E-selectin. It is expressed on certain leukocytes, as well as inflamed endothelial cells. Cutaneous lymphocyte-associated antigen (CLA) represents a modified form of PSGL-1 that interacts with E-selectin for skin homing by T cells.
Blockade of selectins or PSGL-1 inhibits several inflammatory conditions, at least in animal models. These will not be reviewed in detail here, as a recent review is available8. The most impressive experimental data are in models of ischemia-reperfusion, particularly in transplantation and myocardial reperfusion injury, and in atherosclerosis. One widely used selctin inhibitor is recombinant human PSGL-1-Ig fusion protein (rPSGL-1-Ig), whose mechanism of action is prevention of neutrophil entry to inflamed or reperfused tissues. However, results of human trials with selectin inhibitors have been mixed. The most promising selectin inhibitor in human trials appears to be Bimosiamose, which is a pan-selectin inhibitor developed by Revotar Biopharmaceuticals. It was effective in models of allograft and xenograft rejection and in mouse models of asthma. Revotar has reported positive results for human phase IIa clinical trials for chronic obstructive pulmonary disease (COPD), psoriasis and asthma (http://www.revotar.com).
Integrin inhibitors
Natalizumab, the mAb to α4 integrin developed by Biogen-Idec and Elan for the treatment of multiple sclerosis and Crohn's disease, together with another integrin inhibitor, efaluzimab (Raptiva), validates the effectiveness of migration inhibitors for human inflammatory diseases. Natalizumab binds to both α4β1 (VLA-4) and α4β7. Several studies in rodents indicated that an α4-integrin inhibitor should be highly effective for human multiple sclerosis and inflammatory bowel disease. The results of two phase 3 clinical trials showed that natalizumab markedly reduces the number of relapses in individuals with multiple sclerosis9. The notable adverse effect of these trials was the development in two subjects of progressive multifocal leukoencephalopathy, a condition caused by a polyoma virus, JC virus. This complication has resulted in restrictions on the type of patient that can receive the drug.
CD11a-CD18 (LFA-1) is one of the important integrins for leukocyte binding to endothelium and subsequent migration through tissue. Efaluzimab is a humanized mAb that was approved in 2003 for the treatment of moderate to severe plaque psoriasis. A recently published long-term study demonstrated sustained improvement in psoriasis symptoms in subjects throughout three years of continuous treatment10. Thus, efaluzimab is one of the most effective treatments for psoriasis at present.
In addition, other promising approaches in pharmacological targeting of integrins are being developed. The successful molecular modeling of integrins has allowed development of small molecule allosteric antagonists and ligand mimetics (reviewed in ref. 11). In addition, statin compounds, commonly used for the treatment of hypercholesterolemia, also selectively block LFA-1-mediated adhesion and costimulation of lymphocytes and suppress inflammation in a mouse model of peritonitis12. Nevertheless, use of statins as anti-inflammatory drugs in humans has not yet been reported.
Chemoattractant receptor inhibitors
Neutrophils, eosinophils and mast cells express many chemoattractant receptors that serve both innate-immunity and inflammatory functions. Excessive neutrophil influx has been implicated also in immune-mediated inflammatory disorders such as psoriasis, rheumatoid arthritis and inflammatory bowel disease, and, as previously mentioned, excessive eosinophil recruitment has been implicated in the pathogenesis of asthma. Discussed below are some of the most promising chemoattractant receptor targets for inflammatory reactions. Those receptors involved in T cell–mediated inflammatory diseases are discussed separately, although there can be considerable overlap in expression of receptors by macrophages, neutrophils and eosinophils, and by particular T cell subsets.
C5a receptors
The complement component C5a is one of the most potent chemoattractants for neutrophils and eosinophils. It also activates other leukocytes including mast cells and basophils. The detrimental effects of uncontrolled C5a production have been verified in many inflammatory conditions, particularly those involving the pathogenic effects of neutrophils. For instance, overproduced C5a or upregulated C5aR expression has been implicated in the pathogenesis of rheumatoid arthritis, respiratory distress syndrome, inflammatory bowel disease, systemic lupus erythematosus (SLE), ischemia-reperfusion injury, COPD and sepsis (reviewed by ref. 13). Mice genetically deficient in one of the receptors for C5a (C5aR) and antagonists that block binding of C5a to its receptor have established the validity of this receptor as a therapeutic target for many autoimmune diseases and acute inflammatory conditions13,14. Genetic anomalies in regulators of the alternative pathway of complement, such as complement factor H, are associated with particular autoimmune diseases of the kidney and also of the eye, notably age-related macular degeneration15; such diseases represent attractive indications for C5aR antagonists. A second receptor exists for C5a, termed C5L2 (also called GPR77), but its precise function is uncertain. Although this receptor does not signal in the classical fashion like C5aR, it may serve a role in inflammation. Some studies have suggested that C5L2 acts as an anti-inflammatory molecule16, whereas other studies have suggested a proinflammatory role17. Recently, C5L2 deficiency and C5L2-specific antibodies have been shown to protect against sepsis induced in mice by cecal ligation and puncture18, although it still appears that C5aR, rather than C5L2, is overwhelmingly the important target.
Over the past decades, even before the discovery of C5aR, many research groups have tried to develop highly potent and specific small molecule antagonists to block C5a function. This approach has turned out to be surprisingly difficult, probably because C5a has a relatively high molecular weight (>10,000) and binds to C5aR through two or more sites. Novo Nordisk and G2 Therapies have developed a high-affinity mAb to human C5aR (ref. 19), which is now in early clinical trials.
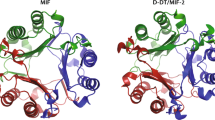
The increasing ease of producing transgenic mice with humanized receptors or ligands will likely establish the ready use of 'human' knock-in mice for new drug development. Four humanized chemoattractant receptor knock-in mice have been reported so far, including C5aR (ref. 19) and also CXCR2 (ref. 20), CCR2 (ref. 21) and CCR5 (ref. 22). Human molecule knock-in mice are particularly useful for preclinical development of drugs that show selectivity for the human target. Many of the best antagonists that have come from initial screens are deprioritized because of their species selectivity. In studies with C5aR mAbs, we have successfully used human C5aR knock-in mice in an inflammatory model. Passively transferred inflammatory arthritis in K/BxN h.C5aR knock-in mice could be prevented or reversed with an mAb specific to human C5aR19 (Fig. 2). One problem with using human molecule knock-in mice is whether the mouse ligand (or receptor) binds with similar affinity and functionality as does the natural human ligand (or receptor); this is the case for the human C5aR and CXCR2 knock-in mice, and, fortunately, many mouse chemokines bind with similar fidelity to human receptor counterparts, although in some cases—for example, CCR2—they show decreased efficacy and potency.

The mouse C5aR coding region was replaced with the human C5aR sequence, to create human C5aR knock-in mice. Mouse neutrophils display high expression of human C5aR, assessed using a human C5aR-specific mAb (left). Human C5aR knock-in mice develop inflammatory arthritis in the K/BxN model (middle). Human C5aR knock-in mice treated with mAb to human C5aR are completely protected (right). These human C5aR knock-in mice have been instrumental for the development of Novo Nordisk's C5aR mAb inhibitor. From Lee et al.19.
CXCR2 and CXCR1
CXCR2 (and its close relative CXCR1) are attractive targets for a range of inflammatory diseases as well as cancers. CXCR2 is the principal chemokine receptor expressed on neutrophils, and its expression extends to eosinophils, mast cells and a small subset of T cells. CXCR2 serves as a receptor for the CXC chemokines that contain the sequence Glu-Leu-Arg near the N terminus, so-called 'ELR' chemokines, namely CXCL8 (IL-8) and CXCL1 (Gro-α). CXCR2 inhibitors are highly effective in animal models of inflammation including lipopolysaccharide-induced lung neutrophilia and arthritis23. A negative sentiment developed about CXCL8 and its receptors after the failure of trials of a mAb to CXCL8 (Abgenix ABX-IL8) in human COPD24 and psoriasis. However ABX-IL-8 may not recognize the immobilized, in vivo active form of CXCL8, which may be one reason for the lack of clinical efficacy. In addition, CXCL8 is not the only CXCR2 or CXCR1 ligand expressed by activated epithelium and endothelium in inflammatory conditions. Hence, inhibitors that target CXCR2, or both CXCR2 and CXCR1, should be much more effective, as these should block six or more ligands. Most drug development activity has focused on CXCR2 because it binds many more ligands than does CXCR1. Patients with COPD, acute respiratory distress syndrome, rheumatoid arthritis and psoriasis would likely benefit from treatment with a CXCR2–CXCR1 inhibitor. In each of these conditions, neutrophils seem to play a pathogenic role and CXCR2 (and/or CXCR1) and their ligands likely play an essential role in neutrophil recruitment. In human rheumatoid arthritis, angiogenesis is likely to contribute to disease pathogenesis and so the anti-angiogenic effects of a CXCR2 inhibitor, as discussed below, may contribute to therapeutic effectiveness. One issue to resolve is the relative importance of CXCR2 versus CXCR1 and versus C5aR. A number of CXCR2–CXCR1 antagonists are in human clinical trials, the most advanced being Schering-Plough's CXCR2 small molecule inhibitor SCH 527123, already in phase 2 trials for COPD and 'neutrophilic' asthma.
Other inflammatory chemoattractant receptors
A number of companies have programs centering on CCR2 antagonism. Incyte has a CCR2 antagonist, INCB3284, which is now in phase 2a clinical trials in patients with rheumatoid arthritis and type 2 diabetes. Merck has a drug, MK0812, in phase 2 trials in subjects with multiple sclerosis. Millennium Pharmaceuticals has a humanized mAb, MLN1202, that targets CCR2. This drug failed in a phase 2 trial for rheumatoid arthritis but is now in trials for multiple sclerosis and atherosclerosis. A mAb to CCL2, possibly the most important CCR2 chemokine ligand, also failed in clinical trials. ABN912 had no effect in rheumatoid arthritis because it dramatically increased the serum concentrations of CCL2 by serving as a blood depot of this chemokine rather than eliminating it25. This result indicates that careful selection of the most appropriate antibody isotypes, their half-lives with and without their target molecules and the mechanisms of elimination must be carefully considered when developing therapeutic antibodies targeting chemokines. A particular problem with CCR2 antagonism might be promotion of Alzheimer's disease. In the brain, microglia may be neuroprotective by phagocytosing amyloid-β protein. In a mouse model of Alzheimer's disease, CCR2 deficiency accelerates early disease progression and results in premature death26. Also, mice deficient in CCR2 (or CCL2) develop cardinal features of age-related macular degeneration, possibly because of defective clearance of C5a and immunoglobulin G (ref. 27). Whether CCR2 antagonists will produce a similar effect will be an important issue. At present, animal data suggest that CCR2 antagonists should be most useful in atherosclerosis and multiple sclerosis28.
Other promising chemoattractant receptors that have been targeted with small molecule inhibitors include CCR1 and the leukotriene B4 (LTB4) receptor, BLT1. Studies with BLT1-deficient mice have validated this receptor, at least in mouse inflammation. Substantial protection from disease was observed in the K/BxN mouse model of inflammatory arthritis29 and, to a lesser degree, in allergic airway models. Nevertheless, the issue exists of how close the biology of the human system matches that of the mouse, since human clinical trials of a LTB4 receptor antagonist found that LTB4 was not a major contributor to the inflammatory process in human rheumatoid arthritis30. CCR1 is an inflammatory chemokine receptor expressed on monocytes, T cells and dendritic cells and interacts with several of the inflammatory chemokines. CCR1 was one of the first chemokine receptors to be identified and so attracted considerable attention from the pharmaceutical industry. Several studies have demonstrated the importance of CCR1 in mouse models of inflammation, particularly in models of rheumatoid arthritis and in experimental autoimmune encephalomyelitis (reviewed in ref. 31). In one human clinical trial, an orally administered CCR1 antagonist developed by Schering AG and Berlex Biosciences showed no effect over placebo in a 16-week randomized, double-blind trial in relapsing-remitting multiple sclerosis. CCR1 is an example of an important target looking for the right therapeutic indication, and several other CCR1 antagonists (by Pfizer, Millennium Pharmaceuticals and ChemoCentryx/GlaxoSmithKline) are in human clinical trials, for indications such as rheumatoid arthritis and transplant rejection.
Chemoattractant receptors for T cell subsets
A straightforward concept that has emerged over the years is that T cell subsets express cell migration molecules appropriate to their functional program. For instance, naive T cells require the special microenvironment of organized lymphoid tissues for their priming and express L-selectin and CCR7, which facilitate migration across high endothelial venules. Expression of various chemoattractant receptors is carefully regulated during T differentiation from naive T cells to functional subsets. As such, the chemoattractant receptors are proving to be reliable markers for functional subsets of effector and memory T cells. CXCR5 marks T follicular helper (TFH) cells that provide T cell help to B cells. CRTh2 and CCR3 mark TH2 T cells, and CCR6 preferentially marks TH-17 cells (Fig. 3). The reason for the association of different receptors with the various T cell subsets and functional programs is because certain subsets need to be in specific places and interact with different leukocyte subsets. This faithful association of receptor expression with functional programs offers opportunities to either block or subdue select arms of the T cell response, for instance, pathogenic TH-17 cells that might be driving an autoimmune disease. Despite the widespread use of chemokine receptors as either markers, or targets, for different types of immune responses, a few considerations must be remembered. None of the individual T cell chemoattractant receptors shown in Figure 3 is absolutely specific for any of the T cell subsets, as they are expressed by innate immune cells and also by many other cells types. One topic not discussed here is receptor expression by CD4+CD25+ regulatory T cells. Chemoattractant receptors place regulatory T cells in the correct locations to facilitate their function, and the main receptors they express are those that have also been implicated in inflammatory diseases: CCR2, CCR4, CCR5, CCR6 and CCR7 (ref. 32). The question of course is whether inhibitors of these receptors will disrupt normal endogenous immune regulatory mechanisms.

(a) TH1 cells produce the cytokine IFN-γ, which stimulates cells to produce chemokines such as CXCL10, a CXCR3 ligand. TH1 cells preferentially express CXCR3 and CCR5, and associate with leukocyte types such as macrophages. GVHD, graft-versus-host disease. (b) TH2 responses typically involve the cytokines IL-4 and IL-13, which stimulate chemokines such as the eotaxins, which recruit CCR3-expressing leukocytes, particularly eosinophils. Another TH2 expressed chemoattractant receptor is CRTh2, which is also expressed by eosinophils. (c) TH-17 cells produce IL-17 isoforms, and these stimulate ELR chemokines such as CXCL8, which attracts neutrophils. The main TH-17 chemoattractant receptor is CCR6, which binds the chemokine CCL20; CCR4 also serves as a chemoattractant receptor. (d) T cell–B cell interactions occur mostly in B cell follicles and germinal centers, and CXCR5—binding the chemokine CXCL13—orchestrates germinal center interactions. The TFH cells that provide help to B cells express CXCR5 and the cytokine IL-21.
T H 1 receptors: CXCR3, CCR5
TH1 cells are important effector cells for antiviral responses and are the main cell type that produces interferon-γ (IFN-γ). Knowledge of the relative importance of TH1 cells versus TH-17 cells as effectors for human autoimmune diseases is still evolving, but virtually all T cells in the synovial fluid of humans with rheumatoid arthritis express CCR5 (ref. 33). Individuals homozygous for the CCR5Δ32 mutation do not express functional CCR5 and are generally protected from developing rheumatoid arthritis, suggesting that CCR5 is a promising target for treatment of rheumatoid arthritis34. CCR5 is the most important co-receptor for HIV entry, and several pharmaceutical companies have produced small molecule CCR5 inhibitors. Pfizer's maraviroc (Selzentry) holds considerable promise for certain inflammatory conditions, as well as for inhibiting HIV entry into CCR5+ cells. Why does HIV target CCR5? CCR5 facilitates effector T cell and dendritic cell migration to mucosal surfaces, where exposure to HIV mostly occurs. CCR5 marks TH1 T cells, which have an antiviral role, and so infection of CCR5+ TH1 cells may also subvert immune defenses. Regardless, the association of CCR5 with HIV infection has resulted in CCR5 antagonists being one of the first chemokine-based drugs to be approved, although not as yet for inflammatory conditions. Study of CCR5Δ32 homozygous individuals suggests that CCR5 antagonists may also be useful therapy for graft-versus-host disease and transplant rejection35,36. One potential downside of a CCR5 inhibitor could be compromised antiviral immune defenses, because, in a study of human West Nile virus infection, CCR5Δ32 homozygosity was significantly associated with death37, and intact CCR5 is also critical for survival of mice infected with West Nile virus38. However, the approximately 1–2% of people of European ancestry lacking CCR5 seems to survive perfectly well, although other mechanisms may compensate for its absence.
The other main chemokine receptor that marks TH1 cells is CXCR3, although its expression is somewhat different in being expressed on a wider variety of T cells, including some TH-17 cells. However its connection to antiviral defense is strong, as its ligands CXCL10 (IP-10), CXCR9 (MIG) and CXCL11 (ITAC) are strongly induced by IFN-γ. Like CCR5, CXCR3 shows a notable expression on T cells associated with particular inflammatory conditions, including rheumatoid arthritis33. Animal model data using CXCR3-deficient mice or CXCR3 inhibitors point to the utility of CXCR3 inhibitors for treating organ transplant rejection and rheumatoid arthritis39. An interesting feature of CXCR3 is that it also serves as an endothelially expressed receptor that promotes angiostasis. Therefore, inhibition of CXCR3 may remove inhibitory signals for new blood vessel growth. One utility of a CXCR3 inhibitor could be promotion of allograft or xenograft acceptance, because inhibition of CXCR3 on T cells would limit T cell recruitment to an inflamed graft, and inhibition of the angiostatic function of CXCR3 would promote angiogenesis and new blood vessel formation in the organ graft. A CXCR3 small molecule inhibitor from Amgen/Tularik failed in a human clinical trial for psoriasis, and since then no companies have reported other clinical trials. A mAb to CXCL10 (MDX-1100, Medarex) is now in clinical trials for ulcerative colitis. CXCL10 (IP-10) is perhaps the most important of the three ligands of CXCR3, and the results of this trial should provide guidance for other drug development programs. Another approach is inhibition of the two TH1 receptors, CXCR3 and CCR5, using one drug. A small molecule antagonist termed TAK-779 blocks both CCR5 and CXCR3 in humans and rodents and inhibits the development of adjuvant-induced arthritis in rats.
T H 2 receptors: CCR3, CRTh2
TH2 responses involve a different set of cytokines, such as interleukin (IL)-4 and IL-13, and these induce chemokines such as the eotaxins (CCL11, CCL24 and CCL26), which attract eosinophils by binding the chemokine receptor CCR3 (see Fig. 3). CCR3 is one of the promising targets for allergic diseases and notably asthma, in part because it functions not only for eosinophil responses, but also for basophils, mast cells and some TH2 T cells. CCR3 is the dominant functional chemokine receptor expressed by eosinophils40, which are strongly implicated in the pathogenesis of human asthma. CCL11 (eotaxin) is secreted by bronchial epithelial and endothelial cells and presumably attracts eosinophils to the lungs of allergic asthmatic patients. Eosinophils release toxic substances, such as major basic protein, designed for defense against large extracellular parasites. Indeed, asthmatic airways resemble a tissue that is mounting an antiparasite response, namely mucous production, smooth muscle contraction (for expulsion of parasites) and eosinophil recruitment.
CCR3 inhibitors, as well as CCR3-deficient mice, have provided validation of this target, particularly in mouse models of allergic airway inflammation7,41,42,43. One would think that the substantial in vivo data on interactions between CCR3 and eotaxins and their overexpression in human asthma would have given rise to many more drug development programs. However the eosinophil fell out of favor with drug companies, partly because of an unsuccessful clinical trial of an IL-5 mAb. It now appears that anti–IL-5 therapy does not totally suppress eosinophil numbers in tissues because other cytokines such as GM-CSF can also contribute to eosinophilia, and neutrophils can also contribute to asthma pathogenesis. A central issue in allergic diseases, particularly human asthma, is defining what cell type is the most 'pathogenic'. If eosinophils are important, then CCR3 represents an ideal target. If allergic diseases are driven more by IL-13–expressing TH2 cells, then other targets may be preferable, because CCR3 is expressed only by a subset of TH2 cells and is dispensable for T cell–mediated allergic responses41. An alternative application for a CCR3 antagonist is eosinophilic esophagitis, a prevalent form of food allergy that causes distressing symptoms—heartburn, nausea and vomiting. A single-nucleotide polymorphism in the human CCL26 gene is associated with susceptibility to eosinophilic esophagitis, and CCR3-deficient mice are protected in an experimental model of eosinophilic esophagitis44. A number of potent CCR3 antagonists have been described, and some have entered human clinical trials45.
CRTh2 (chemoattractant receptor–homologous molecule expressed on TH2 cells) is a receptor for the prostaglandin PGD2. CRTh2 is restricted to allergic-type inflammatory cells, including TH2 cells, eosinophils and basophils, and seems to be a much more reliable TH2-expressed receptor than CCR3. Several biological and genetic studies point to CRTh2 as a highly attractive target for allergic diseases. For instance, potent and selective CRTh2 receptor antagonists significantly reduce airway inflammation in animal models of allergic asthma46,47. A small molecule compound from the biotech company Oxagen, termed ODC9101, is now in phase 2a clinical trials, and intense interest is growing around this target.
T H -17 cells and CCR6 and CCR4
IL-17-producing CD4+ T cells (TH-17 cells) represent a distinct T helper cell lineage48 involved in the pathogenesis of various autoimmune diseases (Fig. 3). TH-17 cells express CCR6 and CCR4, and this combination of receptors distinguishes this subset49, although TH-17 cells probably also express CCR2 and CXCR3 but not CCR5 (ref. 50). Certain IL-17 isoforms act to recruit neutrophils to inflammatory sites. For instance, administration of IL-17A into the airways of mice induces a substantial increase in neutrophils associated with production of CXCL1 and CXCL2 (ref. 51). Several studies suggest CCR6 inhibition holds promise for treatment of TH-17–related inflammatory conditions, such as rheumatoid arthritis52, and multiple sclerosis (F. Sallusto, personal communication). Synoviocytes from arthritic joints of mice and humans produce large amounts of CCL20, a ligand for CCR6, and administering a blocking CCR6 mAb substantially inhibits arthritis in a mouse model52. However, T cells in human rheumatoid arthritis uniformly express CCR5 and CXCR3 (ref. 33), typical TH1 receptors, and so the precise pathogenic role of TH-17 cells versus TH1 cells and their chemokine receptor expression need to be clarified. Inhibition of CCR6 may be more feasible and effective, from a drug development perspective, than inhibiting the many IL-17 isoforms. CCR6 is potentially 'druggable' using organic small molecules, although this target has proven difficult in small molecule screens, and, as such, CCR6 may be a prime target for other inhibitory approaches, such as a blocking mAb.
T FH cells and CXCR5
T cells provide help to B cells within germinal centers. The principal molecules responsible for T and B cell colocalization within germinal centers include CXCR5 and its chemokine ligand CXCL13 (ref. 53). Mice that lack CXCR5 have severely disrupted lymphoid follicles and mount poor T-dependent antibody responses.
The relevance of TFH cells for human disease is that overactive TFH cells drive B cells to make autoantibodies53. A good example of this effect is the San Roque mouse, which develops an antibody-mediated autoimmune disease because of an induced mutation that impairs repression of ICOS expression54. TFH cells also produce CXCL13, which is involved in lymphoid tissue neogenesis and hence may be relevant to the pathogenesis of various chronic inflammatory autoimmune diseases. CXCR5 as a target has not attracted much attention from the pharmaceutical industry because of the limited data available so far on the suitability of CXCR5 inhibitors for antibody-mediated autoimmune diseases, such as SLE.
The promise of tissue-specific cell migration inhibitors
The division of much of the T cell immune system into gut-associated or skin-associated homing subsets represents one of the fundamental subdivisions of the immune system (see the review by Sigmundsdottir and Butcher55 in this issue). It also presents an opportunity for the design of tissue-selective inhibitors for inflammatory diseases. It is now widely accepted that naive T cells migrate randomly between blood and lymphoid tissues, whereas effector and memory T cells polarize to phenotypes associated either with gut or skin tropism56. This polarization relates to the site where a naive T cell was originally primed, whether gut-associated lymphoid tissues or skin-associated lymphoid tissues. These tropisms probably represent a means for rationalization of immunological resources in that antigen-specific effector T cells are directed back to sites where they are most likely to encounter the provocative pathogen. However, the very same tissue-selective effector T cells that mediate host defense, in the gut for instance, can also be associated with pathogenic inflammatory responses, such as celiac disease, Crohn's disease or ulcerative colitis.
One of the promising tissue-specific migration inhibitors in late-stage clinical trials in Crohn's disease is the CCR9 inhibitor CCX282 (Traficet-EN) from ChemoCentryx. CCR9+ T cells contribute to pathogenesis of inflammatory bowel disease in mouse models. The fundamental role of integrin α4β7 for gut homing by T cells and the success of an α4β1 mAb suggest that blockade of α4β7 should be effective for human inflammatory bowel disease. Studies in primates have shown that blockade of α4β7 with a mAb is highly effective for the treatment of colitis57. A recent clinical trial with a humanized mAb to α4β7 (MLN002) in patients with active ulcerative colitis demonstrated a superiority over placebo58. Drugs such as CCX282 or mAb to α4β7 may have fewer side effects, as they could avoid the broad immunosuppressive effects of current anti-inflammatory drugs and selectively target the pathogenic T cells associated with gut homing.
One of the chief defining molecules for T cell migration through the skin is CLA; this binds to E-selectin, which is preferentially expressed on inflamed endothelium in the skin. The chemokine CCL27 (CTACK) and its receptor CCR10 are key chemoattractant molecules for T cell migration to the skin, and neutralization of CCL27 suppresses skin inflammatory responses in animal models59. Inhibitors of CCR10 or CLA could be suitable for immune-mediated skin diseases, particularly psoriasis, although development of drugs has yet to be reported.
Blockade of lymphocyte egress: FTY-720
FTY-720 (Fingolimod) holds promise as a new blockbuster anti-inflammatory drug and, after natalizumab and efaluzimab, is the most advanced in human clinical trials. FTY-720 causes lymphocyte retention in lymph nodes, with a consequent lymphopenia in blood60. This drug is phosphorylated in vivo to yield a molecule that mimics sphingosine-1-phosphate (S1P) and acts as an agonist for four of the five members of the S1P family of GPCRs. The physiological role of S1P receptors on lymphocytes is to control their exit from lymphoid tissues61. This exit is very much an active and regulated process, and certain stimuli, particularly antigen challenge, can reduce lymphocyte exit from lymph nodes to almost zero, an effect described by sheep immunologists as 'lymphocyte shutdown'. FTY-720 sequesters lymphocytes in secondary lymphoid organs, thereby preventing their migration to sites of inflammation. This drug also limits T cell access to organ grafts and autoimmune lesions, reduces inflammation in many animal models and inhibits leukocyte recruitment in a mouse model of airway inflammation62. In an initial proof-of-concept study, FTY-720 reduced the number of MRI-measurable lesions and clinical disease activity in subjects with multiple sclerosis63. Sustained benefits after three years of treatment with the drug in subjects with multiple sclerosis were reported recently in an ongoing phase 2 study64. One potential side-effect of FTY-720 treatment is bradycardia due to expression of certain S1P receptors, particularly S1P3, in the heart. Hence, development of agonists that are selective for one particular receptor subtype, S1P1, are being pursued vigorously by several pharmaceutical companies.
Cell migration inhibitors, angiogenesis and cancer
The association of chemokines and chemokine receptors with angiogenesis, or with tumor cell metastasis, offers an opportunity for the development of new anticancer therapies. Chemokine signaling may act at many levels to promote tumorigenesis65. Certain chemokines mediate angiogenesis, thereby ensuring an adequate blood supply for tumor growth. Chemokines can also facilitate homing of endothelial progenitor cells to tumors, which promotes their growth66,67, and deliver survival signals directly to cancer cells. Finally, expression of certain chemokine receptors, such as CXCR4 and CCR7, may promote tumor metastasis to lymph nodes or other tissues.
Molecules that regulate tumor-associated angiogenesis provide promising targets for treatment of cancers, as evidenced by the antiangiogenic drug bevacizumab (Avastin), an inhibitor of vascular endothelial growth factor. The ELR chemokines, such as CXCL8 and CXCL1, serve an angiogenic role through their binding to CXCR2 expressed by endothelial cells. ELR chemokines released by tumor cells induce microvascular endothelial cell migration and tube formation68. The other main chemokine receptors expressed by endothelium, particularly hypoxic endothelium, include CXCR4 and CXCR7. Expression of CXCR2 and CXCR4 and possibly CXCR7 is regulated by the transcription factor hypoxia inducible factor (HIF)69. This finding presumably relates to the connection between hypoxia and inflammation and the need to promote new blood vessel formation during an active inflammatory response. Several studies have shown substantial inhibition of tumor growth in animal models using chemokine or chemokine receptor inhibitors, particularly for CXCR2, CXCR4 and CXCR7 (refs. 70, 71, 72).
Tumor cells express various chemokines and chemokine receptors, some of which promote tumor growth and metastasis. For instance, CXCR3 is expressed on mouse and human mammary tumor cell lines. Antagonism of CXCR3 on breast tumor cells using a small molecule antagonist inhibits experimental lung metastasis73. CXCR7 is also selectively expressed by certain tumors71 and facilitates prostate cancer metastasis and progression74. Because expression of CXCR7 is restricted to many tumor types and to hypoxic endothelium, a mAb that effectively blocks CXCR7 function and kills CXCR7-expressing cells might be an ideal antitumor agent. Conceivably, CXCR7 may function by heterodimerizing with CXCR4 (ref. 75) and/or CXCR2. Although CXCR7 is a promising target for tumor therapy, the current availability of CXCR2 or CXCR4 small molecule antagonists makes a compelling case for a trial of these in selected human cancers. So far, few companies have revealed clinical programs for chemokine-based angiogenesis inhibitors. Chemokine Therapeutics Corp. has developed a peptide analog of the chemokine CXCL12, which antagonizes CXCR4, and it is in a phase 1/2 trial for cancer indications. A CXCR4 antagonist, AMD3100, has been shown to mobilize CD34+ stem cells from the bone marrow into the blood and augment migration of bone marrow–derived endothelial progenitor cells into sites of neovascularization after myocardial infarction. AMD3100 is being developed as a drug for mobilizing stem cells for transplantation in patients with multiple myeloma and non-Hodgkin's lymphoma. AMD3100 also decreases growth of both primary and metastatic breast cancer in mouse models76.
Targeting hints from viruses and human genetics
A growing number of virally encoded proteins subvert immune responses by binding to many different chemokines (reviewed in ref. 76). Indeed, the chemokine system is frequently targeted by pathogens to subvert immune responses, which suggests that pharmaceutical inhibition for human inflammatory diseases is also a worthwhile approach. Some viruses produce chemokine homologs, typified by vMIP-II, which shows broad antagonistic activity. Another strategy is the use of membrane-expressed chemokine receptor homologs, such as US28 of human cytomegalovirus, which sequesters chemokines to dampen host responses. Finally, some viruses simply use secreted chemokine-binding proteins, such as M-T7 of myxoma virus, that bind chemokines with high affinity. vMIP-II, encoded by Kaposi's sarcoma herpesvirus HHV8, antagonizes many of the TH1-associated receptors, such as CCR1, CCR2 and CCR5, but stimulates TH2-associated receptors such as CCR3. A noteworthy feature of most viral chemokines or chemokine-binding proteins is their broad chemokine or receptor-binding capabilities, which suggests that viruses need to circumvent chemokine redundancy for effective immune subversion (76).
Many polymorphisms have been identified in genes encoding cell migration molecules, particularly chemokines and their receptors. A number of these are associated with human inflammatory diseases or protection from disease. Several have been mentioned above and others are listed in Table 2. In general, the strong association of a gene polymorphism with human disease, such as CCR5 for rheumatoid arthritis, makes a compelling case for targeting a particular molecule. One pending opportunity is the incorporation of pharmacogenomic strategies into the clinical use of migration inhibitors. For example, it would make little sense to give a CCR5Δ32 individual a CCR5 inhibitor, whereas an individual with an allergic disease and a polymorphism in CCL26 might be an ideal patient for a CCR3 antagonist.
Lessons learned and future directions
Pharmaceutically, the preferred method of drug delivery is a pill taken orally. The chemoattractant receptors are GPCRs, which traditionally have been 'druggable' by organic small molecules, a reason why the pharmaceutical industry has embraced chemoattractant receptors so enthusiastically. However, drugs targeting chemoattractant receptors have had a slow genesis. The complement receptor C5aR was discovered 15 years ago, yet few small molecule inhibitors have been described. Likewise, chemokines and their receptors have also been known for some time, yet there is not a single chemokine receptor antagonist on the market for any indication other than HIV infection. The pitfalls in 'drugging' chemoattractant receptors should be fully appreciated, so that lessons can be learned and the full therapeutic potential of this system realized. First, there is still much to learn about the role of chemoattractants in human disease and how best to target cell migration molecules. We need to understand mechanistically how the activities of chemokines are regulated in vivo, the role of the non-signaling receptors such as CXCR7 and D6, and how important heteromerization of chemokines and their receptors is. An inhibitor of one receptor may cooperatively inhibit another receptor to which it heterodimerizes. CCR2 and CCR5 form heterodimers, as do CCR2 and CXCR4 (ref. 78). Thus, chemokine receptor antagonists may regulate allosterically the functional properties of receptors that they do not bind directly78. One of the other big problems is the difficulty in translating findings in the mouse to humans. Information gained from disease models—for example, knockout mice—does not necessarily reflect the human situation. Ultimately, the many human clinical trials of cell migration inhibitors (Table 1) will reveal the roles of the different selectins, integrins and chemoattractant receptors in human inflammatory diseases.
Original discovery efforts for organic small molecule inhibitors of chemoattractant receptors relied on competition ligand binding assays, because these were amenable to high-throughput assays. Experience now indicates that chemoattractant receptor inhibitors are best identified through functional assays such as calcium flux or chemotaxis. Many of these receptor inhibitors now in development are allosteric inhibitors and work by binding to a site other than the natural ligand binding site. A good example is the CCR5 inhibitor TAK779, which inhibits all of the ligands of CCR5 by binding to a site in the transmembrane spanning helices, remote from the ligand contact sites79. The deficiency of many of the early inhibitors, derived from competition binding assays, were that they often cross-reacted with one or more of the hundreds of different GPCRs or ion channels, which was usually discovered relatively late during development. The difficulties inherent in modeling GPCRs, because of their seven-transmembrane structure, resulted in little if any rational antagonist design. Finally, many of the chemoattractant receptor small molecule antagonists developed against human targets lacked adequate affinity or functionality against the homologous target in mice. In some cases, years of synthetic work were spent making human antagonists that would work on rodent receptors.
Because some chemoattractant receptors have proven intractable to inhibition by small molecules, inhibition by mAbs has been an alternative approach. A distinct advantage of mAbs is that they can be used to both inhibit functional activity and kill receptor positive cells through mechanisms such as antibody-dependent cell-mediated cytotoxicity. This latter feature may be advantageous for removing a pathogenic cell type expressing a particular target. For instance, plasmacytoid dendritic cells selectively express the chemoattractant receptor ChemR23 (ref. 80). Some of the best chemoattractant receptor candidates for blocking or killing using mAbs include CCR6 or CCR4 on TH-17 cells and CXCR5 on TFH cells and B cells. Kyowa Hakko and Amgen have developed a depleting mAb to CCR4 that is now in a phase 2 trial for psoriasis.
Truncated or otherwise modified chemokines such as Met-RANTES have been used extensively in animal models and demonstrate a substantial inhibition of inflammation (reviewed in ref. 5). There is one notable clinical program employing a modified chemokine, by Chemokine Therapeutics Corp, whose drug CTCE-9908 is a peptide analog of the chemokine CXCL12 (SDF-1) and an antagonist of its receptor CXCR4; it seems promising in a phase 1/2 trial for cancer. A cyclic peptide derived from the C terminus of C5a serves as a potent antagonist for C5aR (ref. 81), and a drug based on this approach, developed by Arana Therapeutics, is in human trials. Finally, chemokines themselves could serve as drugs, either to stimulate certain effects or to serve as natural antagonists. Ligands of the TH1 related receptor CXCR3 naturally antagonize CCR3, a receptor implicated in TH2 responses.
This review has concentrated on adhesion and chemoattractant receptors. An attractive alternative is inhibition of chemoattractant receptor signaling. This topic is covered in detail by Thelen and Stein82 in this issue. The most promising class of such signaling molecules is PI(3)Ks83. Mice lacking one of the four isoforms, PI(3)Kγ, possess neutrophils and macrophages that show impaired activation through chemoattractant receptors and poor chemotactic responses84. These mice are also protected in various models of inflammation85, including inflammatory arthritis86 and glomerulonephritis87. Several drug companies have produced effective small molecule inhibitors of PI3Kγ (reviewed in ref. 88). These agents inhibit the function of several different chemoattractant receptors simultaneously, thus circumventing the redundancy issue. PI3Kγ signaling also operates for receptors other than chemoattractant receptors, which may offer advantages and drawbacks.
Conclusions
The many clinical trials with cell migration inhibitors that are ongoing or planned should provide considerable new insight into the pathogenesis of human diseases. The already extensive studies of cell migration inhibitors in rodent models of inflammation provide grounds for optimism for the many ongoing and upcoming human trials (Table 1). It will be important for pharmaceutical companies to report the failures, as well as the successes, so that a better understanding is gained of human disease pathogenesis. There will almost certainly be a need to reassess the current animal models of inflammation as the true nature of human inflammatory diseases unfolds.
The promise of cell migration inhibitors for the treatment of inflammatory diseases, and possibly cancers and infectious diseases, is immense. The results of many ongoing clinical trials should further validate the impact this new class of drugs will have on human health and herald a new era for anti-inflammatory therapies.
References
Bach, J.F. The effect of infections on susceptibility to autoimmune and allergic diseases. N. Engl. J. Med. 347, 911–920 (2002).
Viola, A. & Luster, A.D. Chemokines and their receptors: drug targets in immunity and inflammation. Annu. Rev. Pharmacol. Toxicol. 48, 171–197 (2008).
Luster, A.D., Alon, R. & von Andrian, U.H. Immune cell migration in inflammation: present and future therapeutic targets. Nat. Immunol. 6, 1182–1190 (2005).
Mackay, C.R. Chemokines: immunology's high impact factors. Nat. Immunol. 2, 95–101 (2001).
Proudfoot, A.E. Chemokine receptors: multifaceted therapeutic targets. Nat. Rev. Immunol. 2, 106–115 (2002).
Ponath, P.D. et al. Cloning of the human eosinophil chemoattractant, eotaxin. Expression, receptor binding, and functional properties suggest a mechanism for the selective recruitment of eosinophils. J. Clin. Invest. 97, 604–612 (1996).
Humbles, A.A. et al. The murine CCR3 receptor regulates both the role of eosinophils and mast cells in allergen-induced airway inflammation and hyperresponsiveness. Proc. Natl. Acad. Sci. USA 99, 1479–1484 (2002).
Ley, K., Laudanna, C., Cybulsky, M.I. & Nourshargh, S. Getting to the site of inflammation: the leukocyte adhesion cascade updated. Nat. Rev. Immunol. 7, 678–689 (2007).
Polman, C.H. et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N. Engl. J. Med. 354, 899–910 (2006).
Leonardi, C. et al. Efalizumab: results of a 3-year continuous dosing study for the long-term control of psoriasis. Br. J. Dermatol. 158, 1107–1116 (2008).
Shimaoka, M. & Springer, T.A. Therapeutic antagonists and conformational regulation of integrin function. Nat. Rev. Drug Discov. 2, 703–716 (2003).
Weitz-Schmidt, G. et al. Statins selectively inhibit leukocyte function antigen-1 by binding to a novel regulatory integrin site. Nat. Med. 7, 687–692 (2001).
Guo, R.F. & Ward, P.A. Role of C5a in inflammatory responses. Annu. Rev. Immunol. 23, 821–852 (2005).
Lee, H., Whitfeld, P.L. & Mackay, C.R. Receptors for complement C5a. The importance of C5aR and the enigmatic role of C5L2. Immunol. Cell Biol. 86, 153–160 (2008).
Zipfel, P.F., Heinen, S., Jozsi, M. & Skerka, C. Complement and diseases: defective alternative pathway control results in kidney and eye diseases. Mol. Immunol. 43, 97–106 (2006).
Gerard, N.P. et al. An anti-inflammatory function for the complement anaphylatoxin C5a-binding protein, C5L2. J. Biol. Chem. 280, 39677–39680 (2005).
Chen, N.J. et al. C5L2 is critical for the biological activities of the anaphylatoxins C5a and C3a. Nature 446, 203–207 (2007).
Rittirsch, D. et al. Functional roles for C5a receptors in sepsis. Nat. Med. 14, 551–557 (2008).
Lee, H. et al. Human C5aR knock-in mice facilitate the production and assessment of anti-inflammatory monoclonal antibodies. Nat. Biotechnol. 24, 1279–1284 (2006).
Mihara, K. et al. Human CXCR2 (hCXCR2) takes over functionalities of its murine homolog in hCXCR2 knockin mice. Eur. J. Immunol. 35, 2573–2582 (2005).
Prosser, H. et al. Targeted replacement of rodent CCR2 with the human orthologue CCR2B: a mouse model for in vivo analysis of human target-selective small molecule MCP-1 receptor antagonists. Drug Dev. Res. 55, 197–209 (2002).
Saita, Y., Kondo, M., Miyazaki, T., Yamaji, N. & Shimizu, Y. Transgenic mouse expressing human CCR5 as a model for in vivo assessments of human selective CCR5 antagonists. Eur. J. Pharmacol. 518, 227–233 (2005).
Podolin, P.L. et al. A potent and selective nonpeptide antagonist of CXCR2 inhibits acute and chronic models of arthritis in the rabbit. J. Immunol. 169, 6435–6444 (2002).
Mahler, D.A., Huang, S., Tabrizi, M. & Bell, G.M. Efficacy and safety of a monoclonal antibody recognizing interleukin-8 in COPD: a pilot study. Chest 126, 926–934 (2004).
Haringman, J.J. et al. A randomized controlled trial with an anti-CCL2 (anti-monocyte chemotactic protein 1) monoclonal antibody in patients with rheumatoid arthritis. Arthritis Rheum. 54, 2387–2392 (2006).
El Khoury, J. et al. Ccr2 deficiency impairs microglial accumulation and accelerates progression of Alzheimer-like disease. Nat. Med. 13, 432–438 (2007).
Ambati, J. et al. An animal model of age-related macular degeneration in senescent Ccl-2- or Ccr-2-deficient mice. Nat. Med. 9, 1390–1397 (2003).
Boring, L., Gosling, J., Cleary, M. & Charo, I.F. Decreased lesion formation in CCR2−/− mice reveals a role for chemokines in the initiation of atherosclerosis. Nature 394, 894–897 (1998).
Kim, N.D., Chou, R.C., Seung, E., Tager, A.M. & Luster, A.D. A unique requirement for the leukotriene B4 receptor BLT1 for neutrophil recruitment in inflammatory arthritis. J. Exp. Med. 203, 829–835 (2006).
Diaz-Gonzalez, F. et al. Clinical trial of a leucotriene B4 receptor antagonist, BIIL 284, in patients with rheumatoid arthritis. Ann. Rheum. Dis. 66, 628–632 (2007).
Gladue, R. & Brown, M. Current status of CCR1 antagonists in clinical trials. in Chemokine Biology—Basic Research and Clinical Application Vol. II (eds. Neote, K., Letts, G.L. & Moser, B.) 103–113 (Birkhauser, Basel, Switzerland, 2007).
Schneider, M.A., Meingassner, J.G., Lipp, M., Moore, H.D. & Rot, A. CCR7 is required for the in vivo function of CD4+ CD25+ regulatory T cells. J. Exp. Med. 204, 735–745 (2007).
Qin, S. et al. The chemokine receptors CXCR3 and CCR5 mark subsets of T cells associated with certain inflammatory reactions. J. Clin. Invest. 101, 746–754 (1998).
Wheeler, J., McHale, M., Jackson, V. & Penny, M. Assessing theoretical risk and benefit suggested by genetic association studies of CCR5: experience in a drug development programme for maraviroc. Antivir. Ther. 12, 233–245 (2007).
Fischereder, M. et al. CC chemokine receptor 5 and renal-transplant survival. Lancet 357, 1758–1761 (2001).
Bogunia-Kubik, K., Duda, D., Suchnicki, K. & Lange, A. CCR5 deletion mutation and its association with the risk of developing acute graft-versus-host disease after allogeneic hematopoietic stem cell transplantation. Haematologica 91, 1628–1634 (2006).
Glass, W.G. et al. CCR5 deficiency increases risk of symptomatic West Nile virus infection. J. Exp. Med. 203, 35–40 (2006).
Glass, W.G. et al. Chemokine receptor CCR5 promotes leukocyte trafficking to the brain and survival in West Nile virus infection. J. Exp. Med. 202, 1087–1098 (2005).
Mohan, K. & Issekutz, T.B. Blockade of chemokine receptor CXCR3 inhibits T cell recruitment to inflamed joints and decreases the severity of adjuvant arthritis. J. Immunol. 179, 8463–8469 (2007).
Heath, H. et al. Chemokine receptor usage by human eosinophils. The importance of CCR3 demonstrated using an antagonistic monoclonal antibody. J. Clin. Invest. 99, 178–184 (1997).
Ma, W. et al. CCR3 is essential for skin eosinophilia and airway hyperresponsiveness in a murine model of allergic skin inflammation. J. Clin. Invest. 109, 621–628 (2002).
Fulkerson, P.C. et al. A central regulatory role for eosinophils and the eotaxin/CCR3 axis in chronic experimental allergic airway inflammation. Proc. Natl. Acad. Sci. USA 103, 16418–16423 (2006).
Fryer, A.D. et al. Neuronal eotaxin and the effects of CCR3 antagonist on airway hyperreactivity and M2 receptor dysfunction. J. Clin. Invest. 116, 228–236 (2006).
Blanchard, C. et al. Eotaxin-3 and a uniquely conserved gene-expression profile in eosinophilic esophagitis. J. Clin. Invest. 116, 536–547 (2006).
De Lucca, G.V. et al. Discovery of CC chemokine receptor-3 (CCR3) antagonists with picomolar potency. J. Med. Chem. 48, 2194–2211 (2005).
Pettipher, R., Hansel, T.T. & Armer, R. Antagonism of the prostaglandin D2 receptors DP1 and CRTH2 as an approach to treat allergic diseases. Nat. Rev. Drug Discov. 6, 313–325 (2007).
Ulven, T. & Kostenis, E. Targeting the prostaglandin D2 receptors DP and CRTH2 for treatment of inflammation. Curr. Top. Med. Chem. 6, 1427–1444 (2006).
Bettelli, E., Oukka, M. & Kuchroo, V.K. TH-17 cells in the circle of immunity and autoimmunity. Nat. Immunol. 8, 345–350 (2007).
Acosta-Rodriguez, E.V. et al. Surface phenotype and antigenic specificity of human interleukin 17-producing T helper memory cells. Nat. Immunol. 8, 639–646 (2007).
Sato, W., Aranami, T. & Yamamura, T. Cutting edge: human Th17 cells are identified as bearing CCR2+CCR5– phenotype. J. Immunol. 178, 7525–7529 (2007).
Laan, M. et al. Neutrophil recruitment by human IL-17 via C-X-C chemokine release in the airways. J. Immunol. 162, 2347–2352 (1999).
Hirota, K. et al. Preferential recruitment of CCR6-expressing Th17 cells to inflamed joints via CCL20 in rheumatoid arthritis and its animal model. J. Exp. Med. 204, 2803–2812 (2007).
Vinuesa, C.G., Tangye, S.G., Moser, B. & Mackay, C.R. Follicular B helper T cells in antibody responses and autoimmunity. Nat. Rev. Immunol. 5, 853–865 (2005).
Yu, D. et al. Roquin represses autoimmunity by limiting inducible T-cell co-stimulator messenger RNA. Nature 450, 299–303 (2007).
Sigmundsdottir, H. & Butcher, E.C. Environmental cues, dendritic cells and the programming of tissue-selective lymphocyte trafficking. Nat. Immunol. 9, 981–987 (2008).
von Andrian, U.H. & Mackay, C.R. T-cell function and migration. Two sides of the same coin. N. Engl. J. Med. 343, 1020–1034 (2000).
Hesterberg, P.E. et al. Rapid resolution of chronic colitis in the cotton-top tamarin with an antibody to a gut-homing integrin alpha 4 beta 7. Gastroenterology 111, 1373–1380 (1996).
Feagan, B.G. et al. Treatment of ulcerative colitis with a humanized antibody to the α4β7 integrin. N. Engl. J. Med. 352, 2499–2507 (2005).
Homey, B. et al. CCL27–CCR10 interactions regulate T cell-mediated skin inflammation. Nat. Med. 8, 157–165 (2002).
Chiba, K. et al. FTY720, a novel immunosuppressant, induces sequestration of circulating mature lymphocytes by acceleration of lymphocyte homing in rats. I. FTY720 selectively decreases the number of circulating mature lymphocytes by acceleration of lymphocyte homing. J. Immunol. 160, 5037–5044 (1998).
Schwab, S.R. & Cyster, J.G. Finding a way out: lymphocyte egress from lymphoid organs. Nat. Immunol. 8, 1295–1301 (2007).
Sawicka, E. et al. Inhibition of Th1- and Th2-mediated airway inflammation by the sphingosine 1-phosphate receptor agonist FTY720. J. Immunol. 171, 6206–6214 (2003).
Kappos, L. et al. Oral fingolimod (FTY720) for relapsing multiple sclerosis. N. Engl. J. Med. 355, 1124–1140 (2006).
Goodman, A. Fingolimod suppresses disease activity in relapsing-remitting MS. Neurol. Today 8, 16 (2008).
Zlotnik, A. Chemokines and cancer. Int. J. Cancer 119, 2026–2029 (2006).
Spring, H., Schuler, T., Arnold, B., Hammerling, G.J. & Ganss, R. Chemokines direct endothelial progenitors into tumor neovessels. Proc. Natl. Acad. Sci. USA 102, 18111–18116 (2005).
Orimo, A. et al. Stromal fibroblasts present in invasive human breast carcinomas promote tumor growth and angiogenesis through elevated SDF-1/CXCL12 secretion. Cell 121, 335–348 (2005).
Wang, D. et al. CXCL1 induced by prostaglandin E2 promotes angiogenesis in colorectal cancer. J. Exp. Med. 203, 941–951 (2006).
Maxwell, P.J. et al. HIF-1 and NF-κB-mediated upregulation of CXCR1 and CXCR2 expression promotes cell survival in hypoxic prostate cancer cells. Oncogene 26, 7333–7345 (2007).
Burns, J.M. et al. A novel chemokine receptor for SDF-1 and I-TAC involved in cell survival, cell adhesion, and tumor development. J. Exp. Med. 203, 2201–2213 (2006).
Miao, Z. et al. CXCR7 (RDC1) promotes breast and lung tumor growth in vivo and is expressed on tumor-associated vasculature. Proc. Natl. Acad. Sci. USA 104, 15735–15740 (2007).
Wislez, M. et al. High expression of ligands for chemokine receptor CXCR2 in alveolar epithelial neoplasia induced by oncogenic kras. Cancer Res. 66, 4198–4207 (2006).
Walser, T.C. et al. Antagonism of CXCR3 inhibits lung metastasis in a murine model of metastatic breast cancer. Cancer Res. 66, 7701–7707 (2006).
Wang, J. et al. The role of CXCR7/RDC1 as a chemokine receptor for CXCL12/SDF-1 in prostate cancer. J. Biol. Chem. 283, 4283–4294 (2008).
Sierro, F. et al. Disrupted cardiac development but normal hematopoiesis in mice deficient in the second CXCL12/SDF-1 receptor, CXCR7. Proc. Natl. Acad. Sci. USA 104, 14759–14764 (2007).
Smith, M.C. et al. CXCR4 regulates growth of both primary and metastatic breast cancer. Cancer Res. 64, 8604–8612 (2004).
Alcami, A. Viral mimicry of cytokines, chemokines and their receptors. Nat. Rev. Immunol. 3, 36–50 (2003).
Sohy, D., Parmentier, M. & Springael, J.Y. Allosteric transinhibition by specific antagonists in CCR2/CXCR4 heterodimers. J. Biol. Chem. 282, 30062–30069 (2007).
Dragic, T. et al. A binding pocket for a small molecule inhibitor of HIV-1 entry within the transmembrane helices of CCR5. Proc. Natl. Acad. Sci. USA 97, 5639–5644 (2000).
Vermi, W. et al. Role of ChemR23 in directing the migration of myeloid and plasmacytoid dendritic cells to lymphoid organs and inflamed skin. J. Exp. Med. 201, 509–515 (2005).
Wong, A.K. et al. Small molecular probes for G-protein-coupled C5a receptors: conformationally constrained antagonists derived from the C terminus of the human plasma protein C5a. J. Med. Chem. 41, 3417–3425 (1998).
Thelen, M. & Stein, J.V. How chemokines invite leukocytes to dance. Nat. Immunol. 9, 953–959 (2008).
Rommel, C., Camps, M. & Ji, H. PI3Kδ and PI3Kγ: partners in crime in inflammation in rheumatoid arthritis and beyond? Nat. Rev. Immunol. 7, 191–201 (2007).
Sasaki, T. et al. Function of PI3Kγ in thymocyte development, T cell activation, and neutrophil migration. Science 287, 1040–1046 (2000).
Hirsch, E. et al. Central role for G protein-coupled phosphoinositide 3-kinase γ in inflammation. Science 287, 1049–1053 (2000).
Camps, M. et al. Blockade of PI3Kγ suppresses joint inflammation and damage in mouse models of rheumatoid arthritis. Nat. Med. 11, 936–943 (2005).
Barber, D.F. et al. PI3Kγ inhibition blocks glomerulonephritis and extends lifespan in a mouse model of systemic lupus. Nat. Med. 11, 933–935 (2005).
Ruckle, T., Schwarz, M.K. & Rommel, C. PI3Kγ inhibition: towards an 'aspirin of the 21st century'? Nat. Rev. Drug Discov. 5, 903–918 (2006).
Neote, K., Letts, G.L. & Moser, B., eds. Chemokine Biology—Basic Research and Clinical Application Vol. II Pathophysiology of Chemokines (Birkhauser, Basel, Switzerland, 2007).
Moatti, D. et al. Polymorphism in the fractalkine receptor CX3CR1 as a genetic risk factor for coronary artery disease. Blood 97, 1925–1928 (2001).
Abdi, R. et al. Chemokine receptor polymorphism and risk of acute rejection in human renal transplantation. J. Am. Soc. Nephrol. 13, 754–758 (2002).
Valdes, A.M. et al. Val64Ile polymorphism in the C–C chemokine receptor 2 is associated with reduced coronary artery calcification. Arterioscler. Thromb. Vasc. Biol. 22, 1924–1928 (2002).
Wang, L. et al. A functional promoter polymorphism in monocyte chemoattractant protein-1 is associated with psoriasis. Int. J. Immunogenet. 35, 45–49 (2008).
Huang, J.L. et al. Sequence variants of the gene encoding chemoattractant receptor expressed on Th2 cells (CRTH2) are associated with asthma and differentially influence mRNA stability. Hum. Mol. Genet. 13, 2691–2697 (2004).
Acknowledgements
I thank A. Rot, J.-C. Gutierrez Ramos and I. Mackay for helpful suggestions. Supported by the Australian National Health and Medical Research Council and the Cooperative Research Center for Asthma and Airways.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
C.R.S. has equity in a small biotech company that developed and licensed to Novo Nordisk a drug that inhibits C5aR. He also has other commercially related interests around CXCR7 and CCR6.
Rights and permissions
About this article
Cite this article
Mackay, C. Moving targets: cell migration inhibitors as new anti-inflammatory therapies. Nat Immunol 9, 988–998 (2008). https://doi.org/10.1038/ni.f.210
Published:
Issue Date:
DOI: https://doi.org/10.1038/ni.f.210
This article is cited by
-
Polymeric particle-based therapies for acute inflammatory diseases
Nature Reviews Materials (2022)
-
Amino terminal recognition by a CCR6 chemokine receptor antibody blocks CCL20 signaling and IL-17 expression via β-arrestin
BMC Biotechnology (2021)
-
Tumor microenvironmental plasmacytoid dendritic cells contribute to breast cancer lymph node metastasis via CXCR4/SDF-1 axis
Breast Cancer Research and Treatment (2019)
-
A High-Throughput, Multi-Cell Phenotype Assay for the Identification of Novel Inhibitors of Chemotaxis/Migration
Scientific Reports (2016)
-
Pharmacological Beta-Adrenergic Receptor Activation Attenuates Neutrophil Recruitment by a Mechanism Dependent on Nicotinic Receptor and the Spleen
Inflammation (2016)
