
Abstract
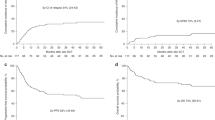
This study compares outcome of reduced-intensity conditioned transplant (RIT) with outcome of conventional non-transplant therapy in patients with Hodgkin's lymphoma relapsing following autograft. There were 72 patients in two groups who had relapsed, and received salvage therapy with chemotherapy±radiotherapy. One group (n=38) then underwent alemtuzumab-containing RIT. The second group—historical controls (n=34), relapsing before the advent of RIT—had no further high-dose therapy. This group was required to respond to salvage therapy and live for over 12 months post-relapse, demonstrating potential eligibility for RIT, had this been available. Overall survival (OS) from diagnosis was superior following RIT (48% at 10 years versus 15%; P=0.0014), as was survival from autograft (65% at 5 years versus 15%; P⩽0.0001). For the RIT group, OS at 5 years from allograft was 51%, and in chemoresponsive patients was 58%, with current progression-free survival of 42%. Responses were seen in 8 of 15 patients receiving donor lymphocyte infusions (DLI) for relapse/progression, with durable remission in five patients at median follow-up from DLI of 45 months (28–55). These data demonstrate the potential efficacy of RIT in heavily pre-treated patients whose outlook with conventional therapy is dismal, and provide evidence of a clinically relevant graft-versus-lymphoma effect.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others

References
Linch DC, Winfield D, Goldstone AH, Moir D, Hancock B, McMillan A et al. Dose intensification with autologous bone-marrow transplantation in relapsed and resistant Hodgkin's disease: results of a BNLI randomised trial. Lancet 1993; 341: 1051–1054.
Schmitz N, Pfistner B, Sextro M, Sieber M, Carella AM, Haenel M et al. Aggressive conventional chemotherapy compared with high-dose chemotherapy with autologous haemopoietic stem-cell transplantation for relapsed chemosensitive Hodgkin's disease: a randomised trial. Lancet 2002; 359: 2065–2071.
Milpied N, Fielding AK, Pearce RM, Ernst P, Goldstone AH . Allogeneic bone marrow transplant is not better than autologous transplant for patients with relapsed Hodgkin's disease. European Group for Blood and Bone Marrow Transplantation. J Clin Oncol 1996; 14: 1291–1296.
Vose JM, Bierman PJ, Anderson JR, Kessinger A, Pierson J, Nelson J et al. Progressive disease after high-dose therapy and autologous transplantation for lymphoid malignancy: clinical course and patient follow-up. Blood 1992; 80: 2142–2148.
Varterasian M, Ratanatharathorn V, Uberti JP, Karanes C, Abella E, Momin F et al. Clinical course and outcome of patients with Hodgkin's disease who progress after autologous transplantation. Leuk Lymphoma 1995; 20: 59–65.
Carella AM, Beltrami G, Carella Jr M, Corsetti MT, Scalzulli RP, Greco M . Immunosuppressive non-myeloablative allografting as salvage therapy in advanced Hodgkin's disease. Haematologica 2001; 86: 1121–1123.
Anderlini P, Saliba R, Acholonu S, Okoroji GJ, Donato M, Giralt S et al. Reduced-intensity allogeneic stem cell transplantation in relapsed and refractory Hodgkin's disease: low transplant-related mortality and impact of intensity of conditioning regimen. Bone Marrow Transplant 2005; 35: 943–951.
Peggs KS, Hunter A, Chopra R, Parker A, Mahendra P, Milligan D et al. Clinical evidence of a graft-versus-Hodgkin's-lymphoma effect after reduced-intensity allogeneic transplantation. Lancet 2005; 365: 1934–1941.
Gajewski JL, Phillips GL, Sobocinski KA, Armitage JO, Gale RP, Champlin RE et al. Bone marrow transplants from HLA-identical siblings in advanced Hodgkin's disease. J Clin Oncol 1996; 14: 572–578.
Akpek G, Ambinder RF, Piantadosi S, Abrams RA, Brodsky RA, Vogelsang GB et al. Long-term results of blood and marrow transplantation for Hodgkin's lymphoma. J Clin Oncol 2001; 19: 4314–4321.
Anderson JE, Litzow MR, Appelbaum FR, Schoch G, Fisher LD, Buckner CD et al. Allogeneic, syngeneic, and autologous marrow transplantation for Hodgkin's disease: the 21-year Seattle experience. J Clin Oncol 1993; 11: 2342–2350.
Tsai T, Goodman S, Saez R, Schiller G, Adkins D, Callander N et al. Allogeneic bone marrow transplantation in patients who relapse after autologous transplantation. Bone Marrow Transplant 1997; 20: 859–863.
di Grazia C, Raiola AM, Van Lint MT, Lamparelli T, Gualandi F, Berisso G et al. Conventional hematopoietic stem cell transplants from identical or alternative donors are feasible in recipients relapsing after an autograft. Haematologica 2001; 86: 646–651.
Robinson SP, Goldstone AH, Mackinnon S, Carella A, Russell N, de Elvira CR et al. Chemoresistant or aggressive lymphoma predicts for a poor outcome following reduced-intensity allogeneic progenitor cell transplantation: an analysis from the Lymphoma Working Party of the European Group for Blood and Bone Marrow Transplantation. Blood 2002; 100: 4310–4316.
Faulkner RD, Craddock C, Byrne JL, Mahendra P, Haynes AP, Prentice HG et al. BEAM-alemtuzumab reduced-intensity allogeneic stem cell transplantation for lymphoproliferative diseases: GVHD, toxicity, and survival in 65 patients. Blood 2004; 103: 428–434.
Corradini P, Zallio F, Mariotti J, Farina L, Bregni M, Valagussa P et al. Effect of age and previous autologous transplantation on nonrelapse mortality and survival in patients treated with reduced-intensity conditioning and allografting for advanced hematologic malignancies. J Clin Oncol 2005; 23: 6690–6698.
Porter DL, Stadtmauer EA, Lazarus HM . ‘GVHD’: graft-versus-host disease or graft-versus-Hodgkin's disease? An old acronym with new meaning. Bone Marrow Transplant 2003; 31: 739–746.
Anderlini P, Acholonu SA, Okoroji GJ, Andersson BS, Couriel DR, De Lima MJ et al. Donor leukocyte infusions in relapsed Hodgkin's lymphoma following allogeneic stem cell transplantation: CD3+ cell dose, GVHD and disease response. Bone Marrow Transplant 2004; 34: 511–514.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Thomson, K., Peggs, K., Smith, P. et al. Superiority of reduced-intensity allogeneic transplantation over conventional treatment for relapse of Hodgkin's lymphoma following autologous stem cell transplantation. Bone Marrow Transplant 41, 765–770 (2008). https://doi.org/10.1038/sj.bmt.1705977
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1705977
Keywords
This article is cited by
-
Management of classical Hodgkin lymphoma: a look at up to date evidence and current treatment approaches
Experimental Hematology & Oncology (2022)
-
Haploidentical related donor compared to HLA-identical donor transplantation for chemosensitive Hodgkin lymphoma patients
BMC Cancer (2020)
-
Is It Time to Revisit the Role of Allogeneic Transplantation in Lymphoma?
Current Oncology Reports (2019)
-
Haploidentical transplantation with post-infusion cyclophosphamide in advanced Hodgkin lymphoma
Bone Marrow Transplantation (2017)
-
Allogeneic hematopoietic stem cell transplantation in Hodgkin lymphoma: a systematic review and meta-analysis
Bone Marrow Transplantation (2016)
