
Abstract
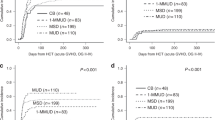
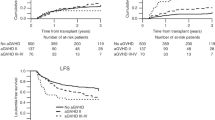
To determine graft-versus-leukemia (GVL) effect after hematopoietic stem cell transplantation (HSCT), we studied the outcome of consecutive children with acute lymphoblastic leukemia (ALL) who received fully matched marrow allografts comparing relapse rate post HSCT between matched sibling donor (MSD) and matched unrelated donor (MUD) recipients. Furthermore, we estimated event-free survival (EFS) on the basis of the occurrence of acute graft-versus-host disease (aGVHD). Between 1998 and 2006 we performed 37 fully MSD and 36 fully MUD HSCTs. All patients received identical conditioning regimens with cyclophosphamide/total body irradiation and dual GVHD prophylaxis with cyclosporine (CSA) and methotrexate (MTX). Three-year cumulative incidence of relapse for the MSD and MUD groups were 55.6±12.3 and 22.0±8.1%, respectively (P=0.03). Three-year EFS according to aGVHD was 32.7±12.2% for no aGVHD, 61.2±10.0% for grade I–II aGVHD and 66.7±11.1% for grade III–IV aGVHD. Three-year EFS and overall survival (OS) were 40.5±11.6, 49.1±9.5% for the MSD group, and 60.5±8.7, 62.3±8.4% for the MUD group. In children with ALL receiving dual GVHD prophylaxis, relapse rate is significantly higher among recipients of MSD compared to MUD transplantation, which may in part be attributed to a better GVL effect with the unrelated graft.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

References
Zikos P, Van Lint MT, Lamparelli T, Gualandi F, Occhini D, Bregante S et al. Allogeneic hemopoietic stem cell transplantation for patients with high risk acute lymphoblastic leukemia: favorable impact of chronic graft-versus-host disease on survival and relapse. Haematologica 1998; 83: 896–903.
Cornelissen JJ, Carston M, Kollman C, King R, Dekker AW, Löwenberg B et al. Unrelated marrow transplantation for adult patients with poor-risk acute lymphoblastic leukemia: strong graft-versus-leukemia effect and risk factors determining outcome. Blood 2001; 97: 1572–1577.
Remberger M, Mattsson J, Hentschke P, Aschan J, Barkholt L, Svennilson J et al. The graft-versus-leukaemia effect in haematopoietic stem cell transplantation using unrelated donors. Bone Marrow Transplant 2002; 30: 761–768.
Gustafsson Jernberg A, Remberger M, Ringden O, Winiarski J . Graft-versus-leukaemia effect in children: chronic GVHD has a significant impact on relapse and survival. Bone Marrow Transplant 2003; 31: 175–181.
Al-Kasim FA, Thornley I, Rolland M, Lau W, Tsang R, Freedman MH et al. Single-centre experience with allogeneic bone marrow transplantation for acute lymphoblastic leukaemia in childhood: similar survival after matched-related and matched-unrelated donor transplants. Br J Haematol 2002; 116: 483–490.
Locatelli F, Zecca M, Messina C, Rondelli R, Lanino E, Sacchi N et al. Improvement over time in outcome for children with acute lymphoblastic leukemia in second remission given hematopoietic stem cell transplantation from unrelated donors. Leukemia 2002; 16: 2228–2237.
Hagglund H, Bostrom L, Ringden O, Nilsson B, Remberger M . Risk factors for acute graft-versus-host disease in 325 consecutive bone marrow recipients. Transplant Proc 1994; 26: 1821–1822.
Benesch M, Deeg HJ . Acute graft-versus-host disease. In: Clinical Bone Marrow and Blood Stem Cell Transplantation, 3rd edn. Cambridge University Press: Cambridge, UK, 2004, pp 1109–1132.
Nordlander A, Mattsson J, Ringdén O, Leblanc K, Gustafsson B, Ljungman P et al. Graft-versus-host disease is associated with a lower relapse incidence after hematopoietic stem cell transplantation in patients with acute lymphoblastic leukemia. Biol Blood Marrow Transplant 2004; 10: 195–203.
Thomas ED, Storb R, Clift RA, Fefer A, Johnson L, Neiman PE et al. Bone-marrow transplantation. N Engl J Med 1979; 292: 832–843, 895–902.
Goodman JL, Winston DJ, Greenfield RA, Chandrasekar PH, Fox B, Kaizer H et al. A controlled trial of fluconazole to prevent infections in patients undergoing bone marrow transplantation. N Engl J Med 1992; 326: 845–851.
Goodrich JM, Bowden RA, Fisher L, Keller C, Meyers JD . Ganciclovir prophylaxis to prevent cytomegalovirus disease after allogeneic marrow transplant. Ann Intern Med 1993; 18: 173–178.
Glucksberg H, Storb R, Fefer A, Buckner CD, Neiman PE, Clift RA et al. Clinical manifestation of graft-versus-host disease in human recipients of marrow from HLA-matched sibling donors. Transplantation 1974; 18: 295–304.
Atkinson K, Horowitz MM, Gale RP, Lee MB, Rimm AA, Bortin MM . Consensus among bone marrow transplanters for diagnosis, grading and treatment of chronic graft-versus-host disease. Bone Marrow Transplant 1989; 4: 247–254.
Sullivan KM, Deeg HJ, Sanders J, Klosterman A, Amos D, Shulman H et al. Hyperacute graft-v-host disease in patients not given immunosuppression after allogeneic marrow transplantation. Blood 1986; 67: 1172–1175.
Lee KH, Choi SJ, Lee JH, Kim S, Seol M, Lee YS et al. Cyclosporine alone vs cyclosporine plus methotrexate for post-transplant immunosuppression after HLA-identical sibling bone marrow transplantation: a randomized prospective study. Bone Marrow Transplant 2004; 34: 627–636.
Storb R, Deeg HJ, Fisher L, Appelbaum F, Buckner CD, Bensinger W et al. Cyclosporine v methotrexate for graft-v-host disease prevention in patients given marrow grafts for leukemia: long-term follow-up of three controlled trails. Blood 1988; 71: 293–298.
Storb R, Deeg HJ, Whitehead J, Appelbaum F, Beatty P, Bensinger W et al. Methotrexate and cyclosporine compared with cyclosporine alone for prophylaxis of acute graft versus host disease after marrow transplantation for leukemia. N Engl J Med 1986; 314: 729–735.
Zikos P, Van Lint MT, Frassoni F, Lamparelli T, Gualandi F, Occhini D et al. Low transplant mortality in allogeneic bone marrow transplantation for acute myeloid leukemia: a randomized study of low-dose cyclosporine vs low-dose cyclosporine and low-dose methotrexate. Blood 1998; 91: 3503–3508.
Zecca M, Prete A, Rondelli R, Lanino E, Balduzzi A, Messina C et al. Chronic graft-versus-host disease in children: incidence, risk factors, and impact on outcome. Blood 2000; 100: 1192–1200.
Locatelli F, Zecca M, Rondelli R, Bonetti F, Dini G, Prete A et al. Graft versus host disease prophylaxis with low-dose cyclosporine-A reduces the risk of relapse in children with acute leukemia given HLA-identical sibling bone marrow transplantation: results of a randomized trial. Blood 2000; 95: 1572–1579.
Peters C, Minkov M, Gadner H, Klingebiel T, Vossen J, Locatelli F . European Group for Blood and Marrow Transplantation (EBMT) working party paediatric diseases; International BFM study group—subcommittee bone marrow transplantation (IBFM-SG). Statement of current majority practices in graft-versus-host disease prophylaxis and treatment in children. Bone Marrow Transplant 2000; 26: 405–411.
Bensinger W . Stem cell trialists' collaborative group. Individual patient data meta-analysis of allogeneic peripheral blood stem cell transplant vs bone marrow transplant in the management of hematological malignancies: indirect assessment of the effect of day 11 methotrexate administration. Bone Marrow Transplant 2006; 38: 539–546.
Acknowledgements
We are indebted to the patients, patients' families, nursing and medical staff of the 8B unit and the oncology units at our partner centers for the provision of excellent patient care, which has been crucial for the achievement of the results reported here.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gassas, A., Sung, L., Saunders, E. et al. Graft-versus-leukemia effect in hematopoietic stem cell transplantation for pediatric acute lymphoblastic leukemia: significantly lower relapse rate in unrelated transplantations. Bone Marrow Transplant 40, 951–955 (2007). https://doi.org/10.1038/sj.bmt.1705853
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1705853
Keywords
This article is cited by
-
AlloHSCT in paediatric ALL and AML in complete remission: improvement over time impacted by accreditation?
Bone Marrow Transplantation (2019)
-
Hematopoietic Stem Cell Transplantation for Childhood Acute Lymphoblastic Leukemia and the Role of MRD: A Single Centre Experience from India
Indian Journal of Hematology and Blood Transfusion (2018)
-
How to Treat Relapsed Acute Lymphoblastic Leukemia: Transplant vs. Conventional Chemotherapy
The Indian Journal of Pediatrics (2013)
-
Early evaluation of immune reconstitution following allogeneic CD3/CD19-depleted grafts from alternative donors in childhood acute leukemia
Bone Marrow Transplantation (2012)
-
Early lymphocyte recovery after allogeneic hematopoietic SCT is associated with significant GVL effect in pediatric ALL but not acute myelogenous leukemia—Update study
Bone Marrow Transplantation (2009)
