
Abstract
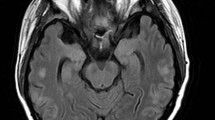
We report a case of posterior reversible leuko- encephalopathy (PRL) following the infusion of dimethylsulfoxide (DMSO) cryopreserved autologous stem cells in the setting of myeloablative chemotherapy in a patient with recurrent Ewing’s sarcoma. Magnetic resonance (MR) imaging revealed white matter changes which resolved over the next 2 months. Bone Marrow Transplantation (2000) 26, 797–800.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others


References
Hinchey J, Chaves C, Appignani B et al. A reversible posterior leukoencephalopathy syndrome New Engl J Med 1996 334: 494–500
Schwartz RB, Jones KM, Kalina P et al. Hypertensive encephalopathy: findings on CT, MR imaging, and SPECT imaging in 14 cases AJR 1992 159: 379–383
Digre KB, Varner MW, Osborn AG, Crawford S . Cranial magnetic imaging in severe pre-eclampsia vs eclampsia Arch Neurol 1993 50: 399–406
Reece DE, Frei-Lahr DA, Shephard JD et al. Neurologiccomplications in allogenic bone marrow transplant patients receiving cyclosporine Bone Marrow Transplant 1991 8: 393–401
Small SL, Fukui MB, Bramblett GT, Eidelman BH . Immunosuppression-induced leukoencephalopathy from tacrolimus Ann Neurol 1996 40: 575–580
Dhodapkar M, Goldberg SL, Tefferi A, Gertz MA . Reversible encephalopathy after cryopreserved peripheral stem cell infusion Am J Hematol 1994 45: 187–188
Gerhards E, Gibian H . The metabolism of dimethyl sulfoxide and its metabolic effects in man and animals Ann NY Acad Sci 1967 141: 65–76
Yellowlees P, Greenfield C, McIntyre N . Dimethylsulphoxide-induced toxicity Lancet 1980 ii: 1004–1006
Egorin MJ, Rosen DM, Sridhara R et al. Plasma concentrations and pharmacokinetics of dimethylsulfoxide and its metabolites in patients undergoing peripheral-blood stem-cell transplants J Clin Oncol 1998 16: 610–615
Shirley SW, Stewart BH, Mirelman S . Dimethyl sulfoxide in treatment of inflammatory genitourinary disorders Urology 1978 11: 215–220
Engel MF . Indications and contraindications for the use of DMSO in clinical dermatology Ann NY Acad Sci 1967 141: 638–645
Smith ER, Hadidian Z, Mason MM . The single and repeated dose toxicity of dimethyl sulfoxide Ann NY Acad Sci 1967 141: 96–109
Alessandrino EP, Bernasconi P, Caldera D et al. Adverse events occurring during bone marrow or peripheral blood progenitor cell infusion: analysis of 126 cases Bone Marrow Transplant 1999 23: 533–537
Zambelli A, Poggi G, Da Pradda GA et al. Clinical toxicity of cryopreserved circulating progentitor cells infusion Anticancer Res 1998 18: 4705–4708
Port JD, Beauchamp NJ . Reversible intracerebral pathological entities mediated by vascular autoregulatory dysfunction Radiographics 1998 18: 353–367
Antunes NL, Small TN, George D et al. Posterior leukoencephalopathy may not be reversible Pediatr Neurol 1999 20: 241–243
Cain MS, Burton GV, Holcombe RF . Fatal leukoencephalopathy in a patient with non-Hodgkin’s lymphoma treated with CHOP chemotherapy and high-dose steroids Am J Med Sci 1998 315: 202–207
Acknowledgements
We thank Dr Georgia Vogelsang for her comments on the paper.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Higman, M., Port, J., Beauchamp, N. et al. Reversible leukoencephalopathy associated with re-infusion of DMSO preserved stem cells. Bone Marrow Transplant 26, 797–800 (2000). https://doi.org/10.1038/sj.bmt.1702589
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1702589
