
Abstract
Background:
Patients who have completed initial cancer treatment (cancer survivors) have been relatively neglected. We need data to help us better understand the needs of this group and to underpin evidence-based service development.
Methods:
Scoping reviews of research published in the last two decades focussing on the problems faced by cancer survivors, and the effectiveness of interventions for these problems were undertaken. The aim was to identify what we know, what we do not know and opportunities where research could provide new information. We searched for, retrieved and rapidly appraised systematic reviews sourced from the most common electronic databases supplemented by more recently published individual studies.
Results:
The research evidence is surprisingly limited. We have some knowledge of the prevalence and nature of depression, pain and fatigue in cancer survivors. We know much less about cognitive and physical impairment, employment, financial well-being and relationships. Even where we have evidence, it is mostly of only moderate quality, is most often only for breast cancer and focuses almost exclusively on the early phase of survivorship. We have good evidence for the effectiveness of drug treatments for pain and moderate evidence for fatigue and depression, but not for other symptoms. Interventions based on rehabilitative and self-management approaches remain in the early stages of evaluation.
Interpretation:
There has been a substantial amount of research describing many of the problems experienced by the cancer survivors. This is strongest in the area of symptoms in the period soon after treatment. However, the quality of the evidence is often poor, and some topics have been little examined. We urgently need data on the natural evolution and scale of the problems of cancer survivors obtained from well-designed, large-scale cohort studies and the robust testing of interventions in clinical trials. Given the current financially constrained research funding environment, we suggest areas in which strategic investment might give findings that have the potential to make a major impact on patient well-being in a 5-year time scale.
Similar content being viewed by others
Main
As cancer incidence rises, cancer mortality falls and the population ages, the number of people living with and beyond cancer will continue to grow by more than 3% a year (Maddams et al, 2009). Although this figure is a testament to advances in the early detection and better treatment of some cancers, there has been growing concern that the services required to meet the physical and emotional needs of survivors have not been adequately developed. A study from the US National Health Interview Study (Hewitt et al, 2003) comparing nearly 5000 cancer survivors with 90 000 people without a history of cancer found that survivors were more likely to report being in poor health and have psychological or functional disability than those without a cancer diagnosis, and the likelihood of poor health was much higher among those who also had another comorbid condition in addition to their cancer. (Elliot and Corner, 2011).
In the UK and internationally, there have been calls for more detailed consideration to be given to the needs of cancer survivors alongside a desire to discover the most effective ways of meeting those needs (Hewitt et al, 2005; Cancer Journey Action Group of the Canadian Partnership Against Cancer, 2008; Department of Health, 2010). For example, in UK, the National Cancer Survivorship Initiative (NCSI) has called for a fundamental shift in the way cancer survivors are supported, moving from a formulaic medical emphasis in follow-up to an approach based on individualised needs and preferences and the promotion of recovery, health and well-being.
Research can have a central role in supporting such shifts, providing the evidence to build a picture of the range and extent of problems that cancer survivors face and testing approaches designed to prevent and alleviate those problems. The research reported here was commissioned to support the research work stream of the NCSI.
We aimed in this review to summarise what is known from existing research about the problems faced by cancer survivors and the effectiveness of different solutions to these problems. We also sought to identify areas in which research investment might have an impact on the care of cancer survivors within the next 5 years to inform the future research priorities of the NCSI. The term ‘cancer survivor’ has been widely interpreted; we have taken this to mean someone who has completed initial cancer treatment and has no evidence of active disease, or is living with progressive disease but is not in the terminal phase of their illness or has had cancer in the past (Macmillan Cancer Support, 2008). We concentrated on the stages of the cancer journey covered by: (1) the period immediately following treatment and (2) the short- and long-term consequences of cancer. Owing to the breadth of the topic area, we used scoping review methodologies. Through the application of this method, we sought to identify what we know, what we do not know and opportunities for research to improve our knowledge of cancer survivorship.
Materials and methods
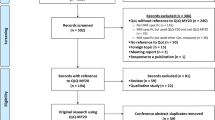
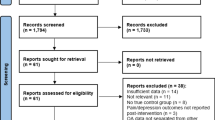
Scoping reviews ‘aim to map rapidly the key concepts underpinning a research area and the main sources and types of evidence available… [suitable for] …an area is complex or has not been reviewed comprehensively before’ (Arksey and O’ Malley, 2005). They are often used to gain a preliminary assessment of potentially relevant literature and its size. Our methods broadly followed those of Arksey and O’ Malley (2005). Two separate but linked reviews focussed on (1) problems faced by cancer survivors and (2) the effectiveness of interventions for these problems. In order to make the task manageable in the time available, we searched for, retrieved and rapidly appraised systematic reviews (rather than original publications) sourced from the most common electronic databases (including Medline, EMBASE, Psychlit, PsychINFO, Cochrane Library, CINAHL, Web of Science and British Nursing Index) up to the end of 2009. The reviews were supplemented with more recently published individual studies. Detailed explanations of the methods used can be found elsewhere (Foster et al, 2009; Richardson et al, 2009; Ziegler et al, 2009; Brearley et al, 2011).
Review one
The first review focussed on the descriptions of the ‘health and well-being’ of cancer survivors including physical, psychological, social and practical aspects.
Inclusion and exclusion criteria
Reviews (including systematic, comprehensive or other types of literature reviews of research evidence of both qualitative and/or quantitative studies) were included if they were written in English, published between 1 January 2000 and 31 December 2009 and focussed on health and well-being in the acute, sub-acute, long-term and disease-free phases of cancer survivorship. Reviews related to childhood and adolescent cancer were excluded (as they were subject to a different piece of work), as were drug trials and review articles other than research literature reviews (e.g., retrospective data review; overview; review of treatment outcome; review of an individual patient case).
Review two
The second scoping review was targeted at scoping and collating research evidence on the effectiveness of solutions to the problems cancer survivors faced. Therefore, the focus of this review was on retrieving systematic reviews and randomised controlled trials (RCTs) of interventions for common problems including symptoms of depression, anxiety and fear of recurrence, emotional distress, fatigue and pain and impairments to physical functioning, social functioning (including relationships), work and employment and cognitive functioning.
Inclusion and exclusion criteria
Published reviews were included if they were written in the English language, published between 1990 and the end of 2009, included an intervention that had relief of one of the above as its primary aim and conducted using systematic review methods. The searching extended to both pharmacological- and non-pharmacological-type interventions and professional-delivered and self-help-type interventions. We excluded reviews devoted to childhood and adolescent cancer and review articles other than those of randomised controlled trials.
Procedures
Abstracts and titles of review articles considered potentially relevant were selected for further examination. The bibliographic details, keywords, abstracts, website address (where available) of identified articles were imported into bibliographic databases. Relevant reviews were selected for synthesis with reference to inclusion/exclusion criteria.
Data were extracted and summarised using data extraction sheets suitable to the different types of reviews. Each review identified for possible inclusion in the problems in the health and well-being element of the scoping review was awarded a quality score (out of 7) as a broad indication of quality. A review was included if it achieved a score of ⩾2. Assessment of the quality of reviews in review 1 was informed by the checklists advocated by the CASP-UK (2011) and Centre for Reviews and Dissemination (2008). Almost all the reviews in the solutions scoping review were high-quality Cochrane-type reviews, and quality screening was not undertaken. Judgments about the study quality of the individual studies included in the reviews were drawn from the commentary available in the systematic reviews. This constitutes a broad assessment of this feature of the research and relies on what we could infer from comments made by the original review authors. Consequently, we only provide a very broad and general indication of whether the quality of the research evidence in relation to each topic was low, medium or high. In terms of the quantity of research contained in the reviews, this could not always be precisely determined, as sometimes review authors (especially in relation to the health and well-being review) did not state explicitly the number of studies they reviewed, but referenced studies throughout the text. Because there was scope for error in counting these, we chose to use approximations and applied a banding system (low, moderate and high amounts of research), and therefore a precise number of studies are not offered (see Table 1 for a summary of criteria used).
To supplement the search for reviews, additional searches to identify primary research papers published after the time frame of the included reviews were performed. This was an extremely time-limited exercise, and we adopted a simple and pragmatic method of focussing on high-quality publications whereby we only included those studies published in journals with an impact factor of more >3 for studies of health and well-being and >5 for studies of interventions.
Results
We included 25 reviews and 61 primary research papers describing problems of health and well-being in review 1, and 49 reviews and 21 primary research papers with respect to solutions in review 2.
Bringing reviews 1 and 2 together, the specific topics addressed in detail were: fatigue and physical functioning, pain, sexual functioning, cognitive functioning, general distress, depression, anxiety, social needs and employment, finance and employment/return to work. Tables 2, 3 and 4 draw together findings in relation to physical, psychological and social dimensions of survivorship in terms of amount, scope and quality of research. Appendix contains a full list of papers included in the scoping review in relation to physical and practical well-being, psychological and social problems, and the systematic reviews of interventions. Review papers are listed in Appendix if they met the initial criteria and were selected and appraised during the data extraction process; however, some do not appear in the Tables 2, 3 and 4 because of their lack of contribution to the final conclusions and/or because they did not relate to the specific areas we addressed in the combined synthesis (for example, we did not address quality of life in general). Each area is now addressed in turn.
Physical functioning and fatigue
The problem
Impairment in physical function has been commonly researched in relation to fatigue. There is strong evidence that cancer survivors experience fatigue soon after treatment, but only modest evidence for increased fatigue in the longer term. There is modest evidence that fatigue is associated with other symptoms such as pain and sleep disturbance and that it impacts quality of life. Most evidence relates to disease-free women with breast and ovarian cancer and survivors of Hodgkin's lymphoma.
Solutions
There is a modest amount of research testing interventions for fatigue and physical functioning, mainly patient education, and rehabilitative approaches such as exercise and cognitive behavioural therapy (CBT). The best evidence is for exercise. No clear overall recommendations for treatment can be made.
Pain
The problem
The evidence clearly shows that pain is a problem for many cancer survivors and specifically that chronic pain is more prevalent in breast cancer survivors than it is in the general population. Radiotherapy and younger age are predictors. Some cancer treatments may cause pain.
Solutions
There is very good evidence that non-steroidal anti-inflammatory drugs and opiates are effective for pain in the general population. There is moderate evidence that these are effective for pain in cancer survivors, but less evidence about how to organise services to effectively deliver these treatments to those who need them.
Sexual problems
The problem
There is strong evidence that cancer and its different forms of treatment can have consequences for a survivor's sexual function. This has been most studied in ovarian, testicular, prostate, bladder and cervical cancer. There is also evidence to suggest that symptoms that accompany treatment-induced menopause are distressing.
Solutions
There is limited evidence for the use of drug treatments and mechanical devices to improve sexual function in patients with gynaecological and urological cancers. Psychological and behavioural treatments have been little researched and the findings are inconclusive.
Cognitive functioning
The problem
There is some evidence that cognitive dysfunction occurs as a consequence of cancer treatment and affects quality of life, but much of the evidence is limited to women with breast cancer. We need more understanding of the incidence, course and effect of alterations in cognitive function in cancer survivors.
Solutions
We did not find any reviews of RCTs of interventions specifically intended to address cognitive impairment.
Employment, return to work and finance
The problem
This important problem has received little attention from researchers. We have a reasonable understanding of the issues and problems people confront as they try to return to work, and there is good evidence that those who have survived cancer are more likely to be unemployed than the general population. There is also good evidence that those who have head and neck cancer do a job that involves manual labour and perceive their work environment to be unsupportive are less likely to return to work. More understanding is needed of the effect of different types of cancer treatment, different types of cancer and other factors on return to work.
Solutions
No evidence on the effectiveness of interventions was located. The application of vocational rehabilitation in other fields could be explored to identify potential approaches.
Emotional distress
The problem
There is very good evidence that cancer survivors suffer from increased distress during and soon after active treatment, but less evidence for its occurrence in long-term survivors. However, there is clearly a subgroup of long-term survivors (for example, those with actual and fear of recurrence) who have high levels of distress that merit help. Most at risk are women, those with a lower socioeconomic status and those with disabling and disfiguring cancers such as head and neck cancers. Most of the evidence is limited to women with breast cancer.
Solutions
There is a large amount of poor-quality research evaluating a range of psychological interventions such as counselling and group therapy. The best evidence is for CBT. There is evidence of temporary benefit only from complementary and alternative medicines. Much of the research is flawed by attempts to treat all patients rather than confining the intervention to those with distress. No clear overall recommendations for treatment can be made at present.
Depression
The problem
There is good evidence for a significantly increased rate of depression in cancer survivors during and soon after active treatment. However, there is less evidence concerning long-term survivors; persistent and recurrent depression is likely to be a problem for an important minority. Those most at risk are people who are younger, female and who have more advanced disease. Much of the evidence is limited to women with breast cancer.
Solutions
There is good evidence that antidepressant drugs, CBT and complex treatment models such as collaborative care are effective for depression in the general population. However, there is only moderately good evidence that antidepressants, CBT and collaborative care are effective in reducing depression specifically in cancer survivors. We do not know how best to identify depression in long-term survivors.
Anxiety
The problem
There is some evidence for increased anxiety after treatment; this is connected with anxiety about check-ups and medical follow-up appointments. There is little evidence concerning long-term survivors, but anxiety, especially about recurrence, is a problem for a proportion. Those most at risk are younger, have more physical symptoms, are closer to point of diagnosis and have more advanced disease. Most of the evidence is limited to women, particularly those with breast and ovarian cancer.
Solutions
There is limited evidence about effective interventions for anxiety. Cognitive behavioural therapy is likely to help, but has not been adequately evaluated. Aromatherapy massage may bring some short-term relief. Exercise may also have a role.
Social needs
The problem
The social impact of cancer and the influence of social support on outcomes such as emotional well-being and quality of life have been studied mainly in breast cancer. There is modest evidence that perceived social support is positively associated with well-being and quality of life. The psychosocial implications of cancer survivorship for family members have not been well studied. Evidence to date suggests that distress in family members persists over 5 years following diagnosis.
Solutions
There is modest evidence that support groups have a positive effect on marital satisfaction and sexual relationships, and some evidence that interventions targeted at spouses might improve marital relationships. No other clear recommendations can be made about approaches that might prove effective with respect to meeting social need.
Quality of the primary research
Although a scoping review does not offer a detailed critique of the methods adopted or study quality, through the process of conducting our review we were struck by a number of recurrent methodological problems that were frequently highlighted by those conducting systematic reviews. These shortcomings are as follows:
Research questions
A key and all too common problem is the lack of precision in the research questions that are asked (e.g., the effect of a vaguely specified intervention on a wide range of vaguely specified outcomes). Such studies, not surprisingly, produce only vague answers.
Samples studied
The origin of samples is sometimes poorly described and they are often not representative of the population studied. Most research has been carried out on women with breast cancer; other cancers have been neglected. There is little research into the needs of minority groups and certain cancers, such as lung and the less common cancers. Most study samples are simply too small to give robust results.
Measures
A wide variety of measures have been used, with little consistency between studies, making the combination of data across studies problematic.
Study design
A common criticism is that studies are methodologically weak and subject to multiple sources of bias, which may make results unreliable. Another major problem of design is the lack of long-term follow-up, both in studies of need and of interventions.
Interventions
The interventions evaluated have often been poorly characterised and may not be of a form that could realistically be implemented in practice.
Interpretation
The research evidence is surprisingly limited. We have some knowledge of the prevalence and nature of depression, pain and fatigue in cancer survivors. We know much less about cognitive and physical impairment, employment, financial well-being and relationships. Even where we have evidence, it is mostly of only moderate quality, is most often focussed on breast cancer and almost exclusively on the early phase of survivorship. We have good evidence of the effectiveness of treatments for pain, and moderate evidence for fatigue and depression, but not for other symptoms. Interventions based on rehabilitative and self-management approaches remain in the early stages of evaluation. Our lack of knowledge about how to address the problems of cancer survivors is compounded by a lack of research into how to implement interventions as part of routinely offered programmes of care. We certainly need more research if we are to address the problems of cancer survivors more effectively.
Limitations of the review
Our review of this large area of research is necessarily limited in scope by the time and resources available to complete it. Primarily, reviews of studies rather than original research reports were examined. Where we did search for individual studies after the publication date of the most recent reviews, we confined this exercise to journals that had a particular impact factor. This may have impacted our findings, particularly judgments about the amount of research available in relation to an individual topic, as some of the journals that publish studies in this field (e.g., Supportive Cancer Care, Cancer Nursing and European Journal of Cancer Care) had not achieved the impact factor selected to merit inclusion. There was a focus on the more common problems and widely used treatments for them to the neglect of other topics. For example, we did not address the organisation and delivery of care, information and support (e.g., the process of care planning and methods of care delivery), the impact on families and the lifestyle dimensions of survivorship.
Setting priorities for future research
Identifying research priorities is not as simple as it might first appear. Critically, it is not as simple as identifying the ‘gaps’ in the evidence described above. The presence of ‘gaps’ in evidence may indicate an area difficult to research that would need many years of investment to address. Furthermore, even in areas where we have the information we need about a problem, including possible solutions, research may still be needed to work out how to implement these solutions in everyday practice.
It is also important to note that research takes more than money; although money is essential, it also requires skilled researchers with an interest in the question to deliver high-quality answers. Such people remain in very short supply for many of the questions posed here, despite this being recognised some years ago (National Cancer Research Institute, 2004).
Scoping reviews, especially those designed to identify research gaps, are often enhanced, and results can be made more useful if policymakers, clinicians and service users contribute to the work in the form of consultation (Arksey and O’ Malley, 2005). Our study also included a consultation and prioritisation element (details can be found in (Armes et al, 2009)). Contributors to this exercise included researchers, commissioners and consumers of survivorship research in the UK. The top five priorities to emerge from a survey and consensus event included: studies to understand the epidemiology of needs; methods to identify and manage consequences of cancer and treatment; the organisation and delivery of care; psychosocial issues; and informal carers and families (Armes et al, 2009). The consultation served to inform and, in some cases, validate the findings from the scoping review. For example, the strong desire for research to determine optimum ways to organise and deliver services emerged in this way.
The shrewd investor in research might therefore be well advised to fund areas of research where not only are there ‘gaps’ in evidence about important topics but where there is also a likelihood of the findings being ‘implementation ready’ in a reasonable time scale and for which there are existing groups with a track record of delivering high-quality research. These represent what we refer to as ‘best buys’ for research investment and are collated in Table 5. We use periods of less than 2 years (very short term), 2–5 years (medium term) and greater than 5 years to qualify these recommendations. These take into account the stage the research has reached, and the relative complexity, scale and length of time it might take to undertake it. We would suggest that funders do not spend limited funds on yet more small-scale research studies unless these comprise a development phase of more significant, large-scale research. Rather, we need well-funded, coordinated research efforts executed by skilled research teams working in partnership with clinicians and cancer survivors. Priorities should be (1) large-scale prospective cohort studies that sufficiently describe needs of long-term survivors and to predict those most at risk; (2) robust randomised trials of well-specified ‘delivery ready’ interventions; (3) research to determine the most effective and efficient ways to organise care.
References
Arksey H, O’ Malley L (2005) Scoping studies: towards a methodological framework. Int J Social Res Methodol 8: 19–32
Armes J, Richardson A, Addington-Hall J (2009) Report on National Cancer Survivorship Consultation on Research Priorities. Technical Report. King's College London and University of Southampton: London
Brearley S, Stamataki Z, Addington-Hall J, Foster C, Hodges L, Jarrett N, Richardson A, Scott I, Sharpe M, Stark D, Siller C, Ziegler L, Amir Z (2011) The physical and practical problems experienced by cancer survivors: a rapid review and synthesis of the literature. Eur J Oncol Nurs 15 (3): 199–288
Cancer Journey Action Group of the Canadian Partnership Against Cancer (2008) Canadian invitational cancer survivorship workshop: creating an agenda for cancer survivorship March 25–26, 2008 Toronto, Ontario
CASP-UK (2011) Critical skills appraisal programme: making sense of evidence. Accessed at www.casp-uk.net/casp-downloads/checklists/. 15 August 2011
Centre for Reviews and Dissemination (2008) Systematic Reviews: CRD's Guidance for Undertaking Reviews in Health Care. CRD, University of York: York
Department of Health, Macmillan Cancer Support, NHS Improvement (2010) National Cancer Survivorship Initiative Vision. Department of Health: London
Elliot J, Fallows A, Staetsky L, Smith PWF, Foster CL, Maher EJ, Corner J (2011) The health and well-being of cancer survivors in the UK: findings from a population-based survey. Br J Cancer 105 (Suppl 1): S11–S20
Foster C, Amir Z, Jarrett N, Stamataki Z, Brearley S, Scott I (2009) Scoping of Research Evidence Regarding the Health and Well-Being of Cancer Survivors: Psychological and Social Problems Faced by Cancer Survivors, and their Physical and Practical Well-Being. Technical Report. University of Southampton and University of Manchester: UK
Hewitt M, Greenfield S, Stovall E (eds) (2005) From Cancer Patient to Cancer Survivor. Lost in Transition. The National Academies Press: Washington DC
Hewitt M, Rowland J, Yancik R (2003) Cancer survivors in the United States. J Gerontol 58 (1): 82–91
Macmillan Cancer Support (2008) Two Million Reasons. The Cancer Survivorship Agenda. Macmillan Cancer Support: London
Maddams J, Brewster D, Gavin A, Steward J, Elliot J, Utley M, Moller H (2009) Cancer prevalence in the United Kingdom: estimates for 2008. Br J Cancer 101: 541–547
National Cancer Research Institute (2004) Supportive and Palliative Care Research in the UK. Report of the NCRI Strategic Planning Group on Supportive and Palliative Care. National Cancer Research Institute: London
Richardson A, Addington-Hall J, Stark D, Foster C, Amir Z, Sharpe M (2009) Determining Research Priorities for Cancer Survivorship: Consultation and Evidence Review. COMPASS and CECO National Cancer Research Institute supportive and palliative care collaboratives: UK
Ziegler L, Hook J, Stark D, Neilly L, Hodges L, Walker J, Sharpe M (2009) Systematic Scope and Collation of Research Evidence Regarding Interventions. Technical Report. University of Leeds and University of Edinburgh: UK
Acknowledgements
We thank the COMPASS and CECo administrators, Susie Edwards and Anne-Marie McDonnell, for their support during the conduct of the study and Liz Neilly and Linda Robertson, librarians at the University of Leeds and University of Southampton, respectively. We also thank those who contributed to the survey and consensus event about research priorities and Jim Elliott and John Neate, Joint Leads of the National Cancer Survivorship Initiative research work stream, for their guidance. The research upon which this paper is based was funded by Macmillan Cancer Support on behalf of the Department of Health and the National Cancer Survivorship Initiative. The views expressed here are those of the authors and not necessarily those of Macmillan Cancer Support or the Department of Health.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Bibliography
-
1)
Absolom K, Eiser C, Turner L, Ledger W, Ross R, Davies H, Coleman R, Hancock B, Snowden J, Greenfield D (2008) Ovarian failure following cancer treatment: current management and quality of life. Hum Reprod 23(11): 2506–2512
-
2)
Ahmed RL, Prizment A, Lazovich D, Schmitz KH, Folsom AR (2008) Lymphedema and quality of life in breast cancer survivors: the Iowa Women's Health Study. J Clin Oncol 26(35): 5689–5696
-
3)
Allareddy V, Kennedy J, West MM, Konety BR (2006) Quality of life in long-term survivors of bladder cancer. Cancer 106(11): 2355–2362
-
4)
Allen JD, Savadatti S, Levy AG (2009) The transition from breast cancer ‘patient’ to ‘survivor. Psychooncology 18: 71–78
-
5)
Arden-Close E, Gidron Y, Moss-Morris R (2008) Psychological distress and its correlates in ovarian cancer: a systematic review. Psychooncology 17(11): 1061–1072
-
6)
Armes J, Chalder T, Addington-Hall J, Richardson A, Hotopf M (2007) A randomized controlled trial to evaluate the effectiveness of a brief, behaviorally oriented intervention for cancer-related fatigue. Cancer 110(6): 1385–1395
-
7)
Arndt V, Stegmaier C, Ziegler H, Brenner H (2006) A population-based study of the impact of specific symptoms on quality of life in women with breast cancer 1 year after diagnosis. Cancer 107(10): 2496–2503
-
8)
Avis NE, Deimling GT (2008) Cancer survivorship and aging. Cancer 113(12 Suppl): 3519–3529
-
9)
Bae JM, Kim S, Kim YW, Ryu KW, Lee JH, Noh JH, Sohn TS, Hong SK, Park SM, You CH, Kim JH, Lee MK, Yun YH (2006) Health-related quality of life among disease-free stomach cancer survivors in Korea. Qual Life Res 15(10): 1587–1596
-
10)
Bakitas M, Doyle Lyons KD, Hegel MT, Balan S, Brokaw FC, Seville J, Hull JG, Zhongze L, Tostetson TD, Byock IR, Ahles TA (2009) Effects of a palliative care intervention on clinical outcomes in patients with advanced cancer. The Project ENABLE II randomized controlled trial. JAMA 302(7): 741–749
-
11)
Bardia A, Barton DL, Prokop LJ, Bauer BA, Moynihan TJ (2006) Efficacy of complementary and alternative medicine therapies in relieving cancer pain: a systematic review. J Clin Oncol 24(34): 5457–5464
-
12)
Barsevick AM, Sweeney C, Haney E, Chung E (2002) A systematic qualitative analysis of psychoeducational interventions for depression in patients with cancer. Oncol Nurs Forum 29: 73–84
-
13)
Beesley V, Eakin E, Steginga S, Aitken J, Dunn J, Battistutta D (2008) Unmet needs of gynaecological cancer survivors: implications for developing community support services. Psychooncology 17: 392–400
-
14)
Beesley V, Janda M, Eakin E, Obermair A, Battistutta D (2007) Lymphedema after gynecological cancer treatment: prevalence, correlates, and supportive care needs. Cancer 109(12): 2607–2614
-
15)
Bellizzi KM, Blank TO (2006) Predicting posttraumatic growth in breast cancer survivors. Health Psychol 25: 47–56
-
16)
Bettencourt B, Schlegel RJ, Talley AE, Molix LA (2007) The breast cancer experience of rural women: a literature review. Psychooncology 16(10): 875–887
-
17)
Bloom JR, Petersen DM, Kang SH (2007) Multi-dimensional quality of life among long-term (5+ years) adult cancer survivors. Psychooncology 16(8): 691–706
-
18)
Bottomley A (1997) Where are we now: evaluating two decades of group interventions with adult cancer patients. J Psychiatr Ment Health Nurs 4 (4): 251–265
-
19)
Bowen DJ, Alfano CM, McGregor BA, Kuniyuki A, Bernstein L, Meeske K, Baumgartner KB, Fetherolf J, Reeve BB, Smith AW, Ganz PA, McTiernan A, Barbash RB (2007) Possible socioeconomic and ethnic disparities in quality of life in a cohort of breast cancer survivors. Breast Cancer Res Treat 106(1): 85–95
-
20)
Bradley CJ, Oberst K, Schenk M (2006) Absenteeism from work: the experience of employed breast and prostate cancer patients in the months following diagnosis. Psychooncology 15(8): 739–747
-
21)
Brothers BM, Andersen BL (2009) Hopelessness as a predictor of depressive symptoms for breast cancer patients coping with recurrence. Psychooncology 18: 267–275
-
22)
Bruera E, El Osta B, Valero V, Driver LC, Pei BL, Shen L, Poulter VA, Palmer JL (2007) Donepezil for cancer fatigue: a double-blind, randomized, placebo-controlled trial. J Clin Oncol 25(23): 3475–3481
-
23)
Campbell HS, Phaneuf MR, Deane K (2004) Cancer peer support programs: do they work? Patient Educ Couns 55: 3–15
-
24)
Carlsen K, Dalton SO, Diderichsen F, Johansen C (2008) Risk for unemployment of cancer survivors: a Danish cohort study. Eur J Cancer 44(13): 1866–1874
-
25)
Carr D, Goudas L, Lawrence D, Pirl W, Lau J, DeVine D, Kupelnick B, Miller K (2002) Management of cancer symptoms: pain, depression, and fatigue. Agency for Healthcare Research and Quality 61: 279
-
26)
Challapalli V, Tremont-Lukats IW, McNicol ED, Lau J, Carr DB (2005) Systemic administration of local anesthetic agents to relieve neuropathic pain. Cochrane Database Syst Rev Issue 4. CD003345.
-
27)
Clough-Gorr KM, Ganz PA, Silliman RA (2007) Older breast cancer survivors: factors associated with change in emotional well-being. J Clin Oncol 25: 1334–1340
-
28)
Collins RF, Bekker HL, Dodwell DJ (2004) Follow-up care of patients treated for breast cancer: a structured review. Cancer Treat Rev 30: 19–35
-
29)
Cooke B, Ernst E (2000) Aromatherapy: a systematic review. Br J Gen Pract 50: 493–496
-
30)
Costanzo ES, Ryff CD, Singer BH (2009) Psychosocial adjustment among cancer survivors: findings from a national survey of health and well-being. Health Psychol 28: 147–156
-
31)
Courneya KS, Segal RJ, Mackey JR, Gelmon K, Reid RD, Friedenreich CM, Ladha AB, Proulx C, Vallance JKH, Lane K, Yasui Y, McKenzie DC (2007) Effects of aerobic and resistance exercise in breast cancer patients receiving adjuvant chemotherapy: a multicenter randomized controlled trial. J Clin Oncol 25(28): 4396–4404
-
32)
Cramp F, Daniel J (2008) Exercise for the management of cancer-related fatigue in adults. Cochrane Database Syst Rev Issue 2. CD006145.
-
33)
Dahl AA, Bremnes R, Dahl O, Klepp O, Wist E, Fossa SD (2007) Is the sexual function compromised in long-term testicular cancer survivors? Eur Urol 52(5): 1438–1447
-
34)
Dahl AA, Haaland CF, Mykletun A, Bremnes R, Dahl O, Klepp O, Wist E, Fosså SD (2005) Study of anxiety disorder and depression in long-term survivors of testicular cancer. J Clin Oncol 23: 2389–2396
-
35)
Daley AJ, Crank H, Saxton JM, Mutrie N, Coleman R, Roalfe A (2007) Randomized trial of exercise therapy in women treated for breast cancer. J Clin Oncol 25(13): 1713–1721
-
36)
De Boer AGEM, Taskila T, Ojajarvi A, van Dijk FJH, Verbeek JHAM (2009) Cancer survivors and unemployment: a meta-analysis and meta-regression. JAMA 301(7): 753–762
-
37)
De Boer AGEM, Verbeek JHAM, Spelten ER, Uitterhoeve ALJ, Ansink A, de Reijke TM, Kammeijer M, Sprangers MAG, van Dijk FJH (2008) Work ability and return-to-work in cancer patients. Br J Cancer 98(8): 1342–1347
-
38)
De Bruin ML, Burgers JA, Baas P, van’t Veer MB, Noordijk EM, Louwman MWJ, Zijlstra JM, van den Berg H, Aleman BMP, van Leeuwen FE (2009) Malignant mesothelioma after radiation treatment for Hodgkin lymphoma. Blood 113(16): 3679–3681
-
39)
Denton AS, Maher J (2003) Interventions for the physical aspects of sexual dysfunction in women following pelvic radiotherapy. Cochrane Database Syst Rev Issue 1. CD003750.
-
40)
Edmondson D, Park CL, Blank TO, Fenster JR, Mills MA (2008) Deconstructing spiritual well-being: existential well-being and HRQOL in cancer survivors. Psychooncology 17: 161–169
-
41)
Edwards AGK, Hulbert-Williams N, Neal RD (2008) Psychological interventions for women with metastatic breast cancer. Cochrane Database Syst Rev Issue 3. CD004253.
-
42)
Elkins G, Marcus J, Stearns V, Perfect M, Rajab MH, Ruud C, Palamara L, Keith T (2008) Randomized trial of a hypnosis intervention for treatment of hot flashes among breast cancer survivors. J Clin Oncol 26(31): 5022–5026
-
43)
Ell K, Xie B, Quon B, Quinn DI, Dwight-Johnson M, Lee PJ (2008) Randomized controlled trial of collaborative care management of depression among low-income patients with cancer. J Clin Oncol 26(27): 4488–4496
-
44)
Espie CA, Fleming L, Cassidy J, Samuel L, Taylor LM, White CA, Douglas NJ, Engleman HM, Kelly HL, Paul J (2008) Randomized controlled clinical effectiveness trial of cognitive behavior therapy compared with treatment as usual for persistent insomnia in patients with cancer. J Clin Oncol 26(28): 4651–4658
-
45)
Eton DT, Lepore SJ (2002) Prostate cancer and health-related quality of life: a review of the literature. Psychooncology 11(4): 307–326
-
46)
Ezzo J, Richardson MA, Vickers A, Allen C, Dibble S, Issell BF, Lao L, Pearl M, Ramirez G, Roscoe JA, Shen J, Shivnan JC, Streitberger K, Treish I, Zhang G (2006) Acupuncture-point stimulation for chemotherapy-induced nausea or vomiting. Cochrane Database Syst Rev Issue 2. CD002285.
-
47)
Falagas ME, Zarkadoulia EA, Ioannidou EN, Peppas G, Christodoulou C, Rafailidis PI (2007) The effect of psychosocial factors on breast cancer outcome: a systematic review. Breast Cancer Res 9(R44)
-
48)
Fleer J, Hoekstra HJ, Sleijfer DT, Hoekstra-Weebers JE (2004) Quality of life of survivors of testicular germ cell cancer: a review of the literature. Support Care Cancer 12(7): 476–486
-
49)
Flynn P, Kew F, Kisely SR (2009) Interventions for psychosexual dysfunction in women treated for gynaecological malignancy. Cochrane Database Syst Rev Issue 2. CD004708.
-
50)
Foley KL, Farmer DF, Petronis VM, Smith RG, Mcgraw S, Smith K, Carver CS, Avis N (2006) A qualitative exploration of the cancer experience among long-term survivors: comparisons by cancer type, ethnicity, gender, and age. Psychooncology 15: 248–258
-
51)
Foster C, Wright D, Hill H, Hopkinson J, Roffe L (2009) Psychosocial implications of living 5 years or more following a cancer diagnosis: a systematic review of the research evidence. Eur J Cancer Care 18(3): 223–247
-
52)
Friedenreich CM, Courneya KS (1996) Exercise as rehabilitation for cancer patients. Clin J Sport Med 6(4): 237–244
-
53)
Goedendorp MM, Gielissen MFM, Verhagen CAHHVM, Bleijenberg G (2009) Psychosocial interventions for reducing fatigue during cancer treatment in adults. Cochrane Database Syst Rev Issue 1. CD006953.
-
54)
Goldzweig G, Andritsch E, Hubert A, Perry NWS, Brenner B, Baider L (2009) How relevant is marital status and gender variables in coping with colorectal cancer? A sample of middle-aged and older cancer survivors. Psychooncology 18: 866–874
-
55)
Goudas L, Carr DB, Bloch R, Balk E, Ioannidis JP, Terrin N, Gialeli-Goudas M, Chew P, Lau J (2001) Management of cancer pain. Volume 1. Volume 2: evidence tables. Agency for Healthcare Research and Quality
-
56)
Greimel ER, Winter R, Kapp KS, Haas J (2009) Quality of life and sexual functioning after cervical cancer treatment: a long-term follow-up study. Psychooncology 18: 476–482
-
57)
Grossman P, Deuring G, Garland SN, Campbell TS, Carlson LE (2008) Patterns of objective physical functioning and perception of mood and fatigue in posttreatment breast cancer patients and healthy controls: an ambulatory psychophysiological investigation. Psychosom Med 70(7): 819–828
-
58)
Gysels M, Higginson IJ (2007) Interactive technologies and videotapes for patient education in cancer care: systematic review and meta-analysis of randomised trials. Support Care Cancer 15: 7–20
-
59)
Harrison JD, Young JM, Price MA, Butow PN, Solomon MJ (2009) What are the unmet supportive care needs of people with cancer? A systematic review. Support Care Cancer 17(8): 1117–1128
-
60)
Haugnes HS, Aass N, Fossa SD, Dahl O, Brydoy M, Aasebo U, Wilsgaard T, Bremnes RM (2009) Pulmonary Function in Long-Term Survivors of Testicular Cancer. J Clin Oncol 27(17): 2779–2786
-
61)
Hayes SC, Janda M, Cornish B, Battistutta D, Newman B (2008) Lymphedema after breast cancer: Incidence, risk factors, and effect on upper body function. J Clin Oncol 26(21): 3536–3542
-
62)
Helgeson VS, Tomich PL (2005) Surviving Cancer: A comparison of 5-year disease-free breast cancer survivors with healthy women. Psychooncology 14: 307–317
-
63)
Hodgkinson K, Butow P, Hobbs KM, Hunt GE, Lo SK, Wain G (2007) Assessing unmet supportive care needs in partners of cancer survivors: The development and evaluation of the Cancer Survivors’ Partners Unmet Needs measure (CaSPUN). Psychooncology 16: 805–813
-
64)
Hodgkinson K, Butow P, Hunt GE, Pendlebury S, Hobbs KM, Wain SKL, Wain G (2007) The development and evaluation of a measure to assess cancer survivors’ unmet supportive care needs: The CaSUN (Cancer Survivors’ Unmet Needs measure). Psychooncology 16: 796–804
-
65)
Hormes JM, Lytle LA, Gross CR, Ahmed RL, Troxel AB, Schmitz KH (2008) The body image and relationships scale: development and validation of a measure of body image in female breast cancer survivors. J Clin Oncol 26: 1269–1274
-
66)
Horneber M, Bueschel G, Huber R, Linde K, Rostock M (2008) Mistletoe therapy in oncology. Cochrane Database Syst Rev Issue 2. CD003297.
-
67)
Irajpour A, Norman I, Griffiths P (2006) Interprofessional education to improve pain management. Br J Commun Nurs 11(1): 29–32
-
68)
Jeffery M, Hickey BE, Hider PN (2007) Follow-up strategies for patients treated for non-metastatic colorectal cancer. Cochrane Database Syst Rev Issue 1. CD002200.
-
69)
Jones RB, Pearson J, Cawsey AJ, Bental D, Barrett A, White J, White CA, Gilmour WH (2006) Effect of different forms of information produced for cancer patients on their use of the information, social support, and anxiety: randomised trial. BMJ 332(7547): 942–948
-
70)
Jonker-Pool G, Van de Wiel HBM, Hoekstra HJ, Sleijfer DTh, Van Driel MF, Van Basten JP, Schraffordt Koops H (2001) Sexual functioning after treatment for testicular cancer: review and meta-analysis of 36 empirical studies between 1975–2000. Arch Sex Behav 30: 55–74
-
71)
Kassab S, Cummings M, Berkovitz S, van Haselen R, Fisher P (2009) Homeopathic medicines for adverse effects of cancer treatments. Cochrane Database Syst Rev Issue 2. CD004845.
-
72)
Kenny PM, King MT, Viney RC, Boyer MJ, Pollicino CA, McLean JM, Fulham MJ, McCaughan BC (2008) Quality of life and survival in the 2 years after surgery for non–small-cell lung cancer. J Clin Oncol 28: 233–241
-
73)
Kirshbaum MN (2007) A review of the benefits of whole body exercise during and after treatment for breast cancer. J Clin Nurs 16: 104–121
-
74)
Kiserud CE, Schover LR, Dahl AA, Fosså A, Bjøro T, Loge JH, Holte H, Yuan Y, Fosså SD (2009) Do male lymphoma survivors have impaired sexual function? J Clin Oncol. Published online ahead of print. DOI: 10.1200/JCO.2009.23.2280
-
75)
Knols R, Aaronson NK, Uebelhart D, Fransen J, Aufdemkampe G (2005) Physical exercise in cancer patients during and after medical treatment: a systematic review of randomized and controlled clinical trials. J Clin Oncol 23: 3830–3842
-
76)
Kobayashi K, Morita S, Shimonagayoshi M, Kobayashi M, Fujiki Y, Uchida Y, Yamaguchi K (2008) Effects of socioeconomic factors and cancer survivors’ worries on their quality of life (QOL) in Japan. Psychooncology 17: 606–611
-
77)
Kornblith AB, Dowell JM, Herndon JE, Engelman BJ, Bauer-Wu S, Small EJ, Morrison VA, Atkins J, Cohen HJ, Holland JC (2006) Telephone monitoring of distress in patients aged 65 years or older with advanced stage cancer: a cancer and leukemia group B study. Cancer 107(11): 2706–2714
-
78)
Kornblith AB, Powell M, Regan MM, Bennett S, Krasner C, Moy B, Younger J, Goodman A, Berkowitz R, Winer E (2007) Long-term psychosocial adjustment of older vs younger survivors of breast and endometrial cancer. Psychooncology 16: 895–903
-
79)
Krischer MM, Xu P, Meade CD, Jacobsen PB (2007) Self-administered stress management training in patients undergoing radiotherapy. J Clin Oncol 25(29): 4657–4662
-
80)
Krouse RS, Herrinton LJ, Grant M, Wendel CS, Green SB, Mohler MJ, Baldwin CM, McMullen CK, Rawl SM, Matayoshi E, Coons SJ, Hornbrook MC (2009) Health-related quality of life among long-term rectal cancer survivors with an ostomy: manifestations by sex. J Clin Oncol 27(28): 4664–4670
-
81)
Krupski TL, Kwan L, Fink A, Sonn GA, Maliski S, Litwin MS (2006) Spirituality influences health related quality of life in men with prostate cancer. Psychooncology 15: 121–131
-
82)
Lee MK, Lee KM, Bae JM, Kim S, Kim YW, Ryu KW, Lee JH, Noh JH, Sohn TS, Hong SK, Yun YH (2008) Employment status and work-related difficulties in stomach cancer survivors compared with the general population. Br J Cancer 98(4): 708–715
-
83)
Leining MG, Gelber S, Rosenberg R, Przypyszny M, Winer EP, Partridge AH (2006) Menopausal-type symptoms in young breast cancer survivors. Ann Oncol 17(12): 1777–1782
-
84)
Lockwood-Rayermann S (2006) Survivorship issues in ovarian cancer: a review. Oncol Nurs Forum 33(3): 553–562
-
85)
Mansky P, Sannes T, Wallerstedt D, Ge A, Ryan M, Johnson LL, Chesney M, Gerber L (2006) Tai chi chuan: mind-body practice or exercise intervention? Studying the benefit for cancer survivors. Integr Cancer Ther 5: 192–201
-
86)
Markes M, Brockow T, Resch K-L (2006) Exercise for women receiving adjuvant therapy for breast cancer. Cochrane Database Syst Rev Issue 4. CD005001.
-
87)
Matei D, Miller AM, Monahan P, Gershenson D, Zhao QQ, Cella D, Champion VL, Williams SD (2009) Chronic physical effects and health care utilization in long-term ovarian germ cell tumor survivors: a gynecologic oncology group study. J Clin Oncol 27(25): 4142–4149
-
88)
McNeely ML, Parliament MB, Seikaly H, Jha N, Magee DJ, Haykowsky MJ, Courneya KS (2008) Effect of exercise on upper extremity pain and dysfunction in head and neck cancer survivors: a randomized controlled trial. Cancer 113(1): 214–222
-
89)
McPherson CJ, Higginson IJ, Hearn J (2001) Effective methods of giving information in cancer: a systematic literature review of randomized controlled trials. J Pub Health Med 23: 227–234
-
90)
Miles C, Candy B, Jones L, Williams R, Tookman A, King M (2007) Interventions for sexual dysfunction following treatments for cancer. Cochrane Database Syst Rev Issue 4. CD005540.
-
91)
Milne HM, Wallman KE, Gordon S, Courneya KS (2008) Effects of a combined aerobic and resistance exercise program in breast cancer survivors: a randomized controlled trial. Breast Cancer Res Treat 108(2): 279–288
-
92)
Minton O, Stone P, Richardson A, Sharpe M, Hotopf M (2008) Drug therapy for the management of cancer related fatigue. Cochrane Database Syst Rev Issue 1. CD006704
-
93)
Moadel AB, Shah C, Wylie-Rosett J, Harris MS, Patel SR, Hall CB, Sparano JA (2007) Randomized controlled trial of yoga among a multiethnic sample of breast cancer patients: effects on quality of life. J Clin Oncol 25(28): 4387–4395
-
94)
Mols F, Korfage IJ, Vingerhoets AJJM, Kil PJM, Coebergh JWW, Essink-Bot ML, Van de Poll-Franse LV (2009) Bowel, urinary, and sexual problems among long-term prostate cancer survivors: a population-based study. Int J Radiat Oncol Biol Phys 73(1): 30–38
-
95)
Mols F, Vingerhoets AJJM, Coebergh JW, Van De Poll-Franse LV (2005) Quality of life among long-term breast cancer survivors: a systematic review. Eur J Cancer 41(17): 2613–2619
-
96)
Morris ME, Grant M, Lynch JC (2007) Patient-reported family distress among long-term cancer survivors. Cancer Nurs 30(1): 1–8
-
97)
Neuhouser ML, Sorensen B, Hollis BW, Ambs A, Ulrich CM, McTiernan A, Bernstein L, Wayne S, Gilliland F, Baumgartner K, Baumgartner R, Ballard-Barbash R (2008) Vitamin D insufficiency in a multiethnic cohort of breast cancer survivors. Am J Clin Nutr 88(1): 133–139
-
98)
Newell SA, Sanson-Fisher RW, Savolainen NJ (2002) Systematic review of psychological therapies for cancer patients: overview and recommendations for future research. J Natl Cancer Inst 94: 558–584
-
99)
Nicholson AB (2007) Methadone for cancer pain. Cochrane Database Syst Rev Issue 4. CD003971.
-
100)
Northouse LL, Mood DW, Schafenacker A, Montie JE, Sandler HM, Forman JD, Hussain M, Pienta KJ, Smith DC, Kershaw T (2007) Randomized clinical trial of a family intervention for prostate cancer patients and their spouses. Cancer 110(12): 2809–2818
-
101)
Osborn RL, Demoncada AC, Feuerstein M (2006) Psychosocial interventions for depression, anxiety, and quality of life in cancer survivors: meta-analyses. Int J Psychiatry Med 36: 13–34
-
102)
Park CL, Gaffey AE (2007) Relationships between psychosocial factors and health behavior change in cancer survivors: an integrative review. Ann Behav Med 34(2): 115–134
-
103)
Park SY, Bae DS, Nam JH, Park CT, Cho CH, Lee JM, Lee MK, Kim SH, Park SM, Yun YH (2007) Quality of life and sexual problems in disease-free survivors of cervical cancer compared with the general population. Cancer 110(12): 2716–2725
-
104)
Parker PA, Pettaway CA, Babaian RJ, Pisters LL, Miles B, Fortier A, Wei Q, Carr DD, Cohen L (2009) The effects of a presurgical stress management intervention for men with prostate cancer undergoing radical prostatectomy. J Clin Oncol 27(19): 3169–3176
-
105)
Paskett ED, Herndon II JE, Day JM, Stark NN, Winer EP, Grubbs SS, Pavy MD, Shapiro CL, List MA, Hensley ML, Naughton MA, Kornblith AB, Habin KR, Fleming GF, Bittoni MA (2008) Applying a conceptual model for examining health related quality of life in long-term breast cancer survivors: CALGB study 79804. Psychooncology 17: 1108–1120
-
106)
Passalacqua R, Caminiti C, Campione F, Diodati F, Todeschini R, Bisagni G, Labianca R, Chiesa MD, Bracci R, Aragona M, Artioli F, Cavanna L, Masina A, De Falco F, Marzocchini B, Iacono C, Contu A, Costanzo FD, Bertetto O, Annunziata MA (2009) Prospective, multicenter, randomized trial of a new organizational modality for providing information and support to cancer patients. J Clin Oncol 27(11): 1794–1799
-
107)
Petticrew M, Bell R, Hunter D (2002) Influence of psychological coping on survival and recurrence in people with cancer: Systematic review. BMJ 325(7372): 1066–1069
-
108)
Peuckmann V, Ekholm O, Rasmussen NK, Groenvold M, Christiansen P, Moller S, Eriksen J, Sjogren P (2009) Chronic pain and other sequelae in long-term breast cancer survivors: Nationwide survey in Denmark. Eur J Pain 13(5): 478–485
-
109)
Pitkethly M, MacGillivray S, Ryan R (2008) Recordings or summaries of consultations for people with cancer. Cochrane Database Syst Rev Issue 3. CD001539.
-
110)
Quigley C (2002) Hydromorphone for acute and chronic pain. Cochrane Database Syst Rev Issue 1. CD003447.
-
111)
Rao AV, Demark-Wahnefried W (2006) The older cancer survivor. Crit Rev Oncol Hematol 60(2): 131–143
-
112)
Rehse B, Pukrop R (2003) Effects of psychosocial interventions on quality of life in adult cancer patients: meta analysis of 37 published controlled outcome studies. Patient Educ Couns 50: 179–186
-
113)
Richards KC, Gibson R, Overton-McCoy AL (2000) Effects of massage in acute and critical care. AACN Clinical Issues: Advanced Practice in Acute and Critical Care 11: 77–96
-
114)
Robb KA, Bennett MI, Johnson MI, Simpson KJ, Oxberry SG (2008) Transcutaneous electric nerve stimulation (TENS) for cancer pain in adults. Cochrane Database Syst Rev Issue 3. CD006276.
-
115)
Rodin G, Lloyd G, Katz M, Green E, Mackay JA, Wong RK (2007) The treatment of depression in cancer patients: a systematic review. Support Care Cancer 15: 123–136
-
116)
Roscoe JA, Kaufman ME, Matteson-Rusby SE, Palesh OG, Ryan JL, Kohli S, Perlis ML, Morrow GR (2007) Cancer-related fatigue and sleep disorders. Oncologist 12: 35–42
-
117)
Rossen PB, Pedersen A, Zachariae R, von der Maase H (2009) Health-related quality of life in long-term survivors of testicular cancer. J Clin Oncol. Published ahead of print. DOI:10.1200/JCO.2008.19.6931
-
118)
Russell KM, Von Ah DM, Giesler RB, Storniolo AM, Haase JE (2008) Quality of life of African American breast cancer survivors: how much do we know? Cancer Nurs 31(6): E36–E45
-
119)
Salsman JM, Segerstrom SC, Brechting EH, Carlson CR, Andrykowski MA (2009) Posttraumatic growth and PTSD symptomatology among colorectal cancer survivors: a 3-month longitudinal examination of cognitive processing. Psychooncology 18: 30–41
-
120)
Saquib N, Flatt SW, Natarajan L, Thomson CA, Bardwell WA, Caan B, Rock CL, Pierce JP (2007) Weight gain and recovery of pre-cancer weight after breast cancer treatments: evidence from the women's healthy eating and living (WHEL) study. Breast Cancer Res Treat 105(2): 177–186
-
121)
Schneider EC, Malin JL, Kahn KL, Ko CY, Adams J, Epstein AM (2007) Surviving colorectal cancer: patient-reported symptoms 4 years after diagnosis. Cancer 110(9): 2075–2082
-
122)
Sellick SM, Zaza C (1998) Critical review of 5 non-pharmacologic strategies for managing cancer pain. Cancer Prevent Control 2: 7–14
-
123)
Servaes P, Verhagen C, Bleijenberg G (2002) Fatigue in cancer patients during and after treatment: prevalence, correlates and interventions. Eur J Cancer 38(1): 27–43
-
124)
Sheard T, Maguire P (1999) The effect of psychological interventions on anxiety and depression in cancer patients: results of two meta analyses. Br J Cancer 80(11): 1770–1780
-
125)
Short PF, Vasey JJ, Belue R (2008) Work disability associated with cancer survivorship and other chronic conditions. Psychooncology 17(1): 91–97
-
126)
Skaali T, Fossa SD, Bremnes R, Dahl O, Haaland CF, Rønneberg Hauge E, Olbjør n Klepp, Oldenburg J, Wist E, Dahl AA (2009) Fear of recurrence in long-term testicular cancer survivors. Psychooncology 18: 580–588
-
127)
Smedslund G, Ringdal GI (2004) Meta-analysis of the effects of psychosocial interventions on survival time in cancer patients. J Psychosom Res 57(2): 123–131
-
128)
Smith JE, Richardson J, Hoffman C, Pilkington K (2005) Mindfulness-based stress reduction as supportive therapy in cancer care: systematic review. J Adv Nurs 52(3): 315–327
-
129)
Smith SK, Zimmerman S, Williams CS, Preisser JS, Clipp EC (2008) Post-traumatic stress outcomes in non-Hodgkin's lymphoma survivors. J Clin Oncol 28: 934–941
-
130)
Solà I, Thompson EM, Subirana Casacuberta M, Lopez C, Pascual A (2004) Non-invasive interventions for improving well-being and quality of life in patients with lung cancer. Cochrane Database Syst Rev Issue 4. CD004282.
-
131)
Somani BK, Kumar V, Wong S, Pickard R, Ramsay C, Nabi G, Grant A, N’Dow J (2007) Bowel dysfunction after transposition of intestinal segments into the urinary tract: 8-year prospective cohort study. J Urol 177(5): 1793–1798
-
132)
Spelten E, Sprangers M, Verbeek J (2002) Factors reported to influence the return to work of cancer survivors: a literature review. Psychooncology 11(2): 31
-
133)
Steginga SK, Lynch BM, Hawkes A, Dunn J, Aitken J (2009) Antecedents of domain-specific quality of life after colorectal cancer. Psychooncology 18: 216–220
-
134)
Strong V, Waters R, Hibberd C, Murray G, Wall L, Walker J, McHugh G, Walker A, Sharpe M (2008) Management of depression for people with cancer (SMaRT oncology 1): a randomised trial. Lancet 372(9632): 40–48
-
135)
Syrjala KL, Abrams JR, Polissar NL, Hansberry J, Robison J, DuPen S, Stillman M, Fredrickson M, Rivkin S, Feldman E, Gralow J, Rieke JW, Raish RJ, Lee DJ, Cleeland CS, DuPen A (2008) Patient training in cancer pain management using integrated print and video materials: a multisite randomized controlled trial. Pain 135(1–2): 175–186
-
136)
Taskila T, Martikainen R, Hietanen P, Lindbohm ML (2007) Comparative study of work ability between cancer survivors and their referents. Eur J Cancer 43(5): 914–920
-
137)
Tatrow K, Montgomery GH (2006) Cognitive behavioral therapy techniques for distress and pain in breast cancer patients: a meta-analysis. J Behav Med 29: 17–27
-
138)
Thornton AA, Perez MA (2006) Posttraumatic growth in prostate cancer survivors and their partners. Psychooncology 15: 285–296
-
139)
Vallance JKH, Courneya KS, Plotnikoff RC, Yasui Y, Mackey JR (2007) Randomized controlled trial of the effects of print materials and step pedometers on physical activity and quality of life in breast cancer survivors. J Clin Oncol 25(17): 2352–2359
-
140)
Van den Beuken-van Everdingen MHJ, Peters ML, De Rijke JM, Schouten HC, Van Kleef M, Patijn J (2008) Concerns of former breast cancer patients about disease recurrence: a validation and prevalence study. Psychooncology 17: 1137–1145
-
141)
Visovsky C, Schneider SM (2003) Cancer-related fatigue. Online J Issues Nurs 8(3): 8
-
142)
Vivar CG, Canga N, Canga AD, Arantzamendi M (2009) The psychosocial impact of recurrence on cancer survivors and family members: a narrative review. J Adv Nurs 65(4): 724–736
-
143)
Vivar CG, McQueen A (2005) Informational and emotional needs of long-term survivors of breast cancer. J Adv Nurs 51(5): 520–528
-
144)
Walsh RA, Girgis A, Sanson-Fisher RW (1998) Breaking bad news 2: what evidence is available to guide clinicians? Behav Med 24(2): 61–72
-
145)
Weathers B, Barg FK, Collier A, Halbert CH (2006) Perceptions of changes in weight among African American breast cancer survivors. Psychooncology 15(2): 174–179
-
146)
Weber BA, Sherwill-Navarro P (2005) Psychosocial consequences of prostate cancer: 30 years of research. Geriatr Nurs 26(3): 166–175
-
147)
Wessex Institute for Health Research and Development (1998). Psycho-social interventions in oncology: counselling services for women with breast cancer. Southampton: Wessex Institute for Health Research and Development. Development and Evaluation Committee Report; 86
-
148)
Wiffen PJ, McQuay HJ (2007) Oral morphine for cancer pain. Cochrane Database Syst Rev Issue 4. CD003868.
-
149)
Wilkinson SM, Love SB, Westcombe AM, Gambles MA, Burgess CC, Cargill A, Young T, Maher EJ, Ramirez AJ (2007) Effectiveness of aromatherapy massage in the management of anxiety and depression in patients with cancer: a multicenter randomized controlled trial. J Clin Oncol 25(5): 532–539
-
150)
Williams S, Dale J (2006) The effectiveness of treatment for depression/depressive symptoms in adults with cancer: a systematic review. Br J Cancer 94(3): 372–390
-
151)
Wootten AC, Burney S, Foroudi F, Frydenberg M, Coleman G, Ng KT (2007) Psychological adjustment of survivors of localised prostate cancer: investigating the role of dyadic adjustment, cognitive appraisal and coping style. Psychooncology 16: 994–1002
-
152)
Zabalegui A, Sanchez S, Sanchez PD, Juando C (2005) Nursing and cancer support groups. J Adv Nurs 51(4): 369–381
-
153)
Zebrack BJ, Yi J, Petersen L, Ganz PA (2008) The impact of cancer and quality of life for long-term survivors. Psychooncology 17: 891–900
-
154)
Zeppetella G, Ribeiro MDC (2006) Opioids for the management of breakthrough (episodic) pain in cancer patients. Cochrane Database Syst Rev Issue 1. CD004311.
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Richardson, A., Addington-Hall, J., Amir, Z. et al. Knowledge, ignorance and priorities for research in key areas of cancer survivorship: findings from a scoping review. Br J Cancer 105 (Suppl 1), S82–S94 (2011). https://doi.org/10.1038/bjc.2011.425
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2011.425
Keywords
This article is cited by
-
The challenges of returning to work for differentiated thyroid cancer survivors in china: a qualitative study
Supportive Care in Cancer (2023)
-
Defining research and infrastructure priorities for cancer survivorship in Australia: a modified Delphi study
Supportive Care in Cancer (2022)
-
A scoping review of return to work decision-making and experiences of breast cancer survivors in Korea
Supportive Care in Cancer (2021)
-
Relaxation versus exercise for improved quality of life in lymphoma survivors—a randomised controlled trial
Journal of Cancer Survivorship (2021)
-
Return-to-Work and Breast Cancer Survivorship Care
Current Breast Cancer Reports (2020)
