
Abstract
Background:
There are few known risk factors for renal cell carcinoma (RCC). Two small hospital-based case–control studies suggested an association between short blood telomere length (TL) and increased RCC risk.
Methods:
We conducted a large population-based case–control study in two metropolitan regions of the United States comparing relative TL in DNA derived from peripheral blood samples from 891 RCC cases and 894 controls. Odds ratios and 95% confidence intervals were estimated using unconditional logistic regression in both unadjusted and adjusted models.
Results:
Median TL was 0.85 for both cases and controls (P=0.40), and no differences in RCC risk by quartiles of TL were observed. Results of analyses stratified by age, sex, race, tumour stage, and time from RCC diagnosis to blood collection were similarly null. In multivariate analyses among controls, increasing age and history of hypertension were associated with shorter TL (P<0.001 and P=0.07, respectively), and African Americans had longer TL than Caucasians (P<0.001).
Conclusion:
These data do not support the hypothesis that blood TL is associated with RCC. This population-based case–control study is, to our knowledge, the largest investigation to date of TL and RCC.
Similar content being viewed by others


Main
Telomeres are nucleotide repeats and a protein complex at chromosome ends that are essential for chromosomal stability. Telomere attrition occurs with each cell division due to inefficient replication at the ends of linear DNA. Critically short telomeres trigger cellular senescence and death, but cancer cells divide despite the resultant genomic instability. Telomere length (TL) is a suspected marker of cancer risk (De Lange, 2005). Two small hospital-based case–control studies (32 and 65 cases, respectively) reported an increased risk of renal cell carcinoma (RCC) in relation to shorter TL (Wu et al, 2003; Shao et al, 2007). To follow up on these findings, we evaluated RCC risk in relation to TL in a large case–control study.
Materials and methods
Study population, data and sample collection, and sample processing
Subject recruitment and data and specimen collection methods have been described (Colt et al, 2011). Briefly, this population-based case–control study of Caucasians and African Americans was conducted in Detroit, MI, USA (Wayne, Oakland, and Macomb Counties) from 2002–2007, and in Chicago, IL, USA (Cook County) in 2003; according to US census estimates from 2000, the populations of these two metropolitan areas had generally similar racial distributions (56.3% Caucasian and 26.1% African American in Cook County; 68.9% Caucasian and 25.0% African American in Wayne, Oakland, and Macomb Counties, combined). To maximise enrolment of African Americans, we over-sampled African American cases relative to Caucasian cases, and we frequency matched controls to cases at a 2 : 1 ratio for African Americans and a 1 : 1 ratio for Caucasians to increase statistical power for analyses stratified by race. Subjects with stored blood samples (whole blood or buffy coat) were included in this analysis. Eight cases with benign tumours, non-RCC histology, or cancer in a transplanted kidney were excluded. Telomere length could not be measured for one control subject, who was also excluded, leaving 891 cases (658 Caucasians and 233 African Americans) and 894 controls (550 Caucasians and 344 African Americans). Blood samples were collected from cases and controls at the time of the personal interview. Among cases, the median time from RCC diagnosis to blood sample collection was ∼4 months. Samples of DNA were extracted via Qiagen kits; DNA was derived from whole blood samples for most study subjects (cases: 627 whole blood, 264 buffy coat; controls: 768 whole blood, 126 buffy coat). The distribution of the source material for DNA extraction was similar for each study centre. Study procedures were approved by Institutional Review Boards at collaborating institutions, and written informed consent was obtained from all subjects.
TL measurements
A quantitative PCR assay was used to measure TL; assay methods have been described (Cawthon, 2002). Briefly, telomere repeat (T) and single gene (S) copy numbers were measured in individual samples and adjusted in comparison to standard reference DNA; the standardised T/S ratio characterises relative TL. In TL measurements for blinded duplicate QC samples from 59 subjects, the coefficient of variation (CV) was 9.9% and the intraclass correlation coefficient was 0.85 (95% confidence interval (CI): 0.76, 0.91).
Statistical analysis
Telomere length data were natural log-transformed to achieve a normal distribution. We compared TL between cases and controls, and evaluated differences in TL by demographic and personal characteristics among controls in bivariate and multivariate analyses. Odds ratios (ORs) and 95% CIs were calculated using unconditional logistic regression. Quartiles of TL were determined based on the distribution among controls. Adjusted analyses included terms for age (10-year categories), sex, race, smoking, body mass index (BMI), history of hypertension, education, study centre, and material type (whole blood or buffy coat). Analyses stratified by these covariates, tumour stage/grade, RCC treatment modality, and time from RCC diagnosis to blood collection were also performed.
Results
Cases and controls had similar age and sex distributions. Cases were more likely to be obese (BMI⩾30), to smoke, and to have a history of hypertension, as reported previously (Karami et al, 2010). The vast majority of cases with treatment information available had surgery alone without adjuvant therapy (N=803; 92%), and most cases with information on stage at diagnosis had localised disease (N=611; 81%).
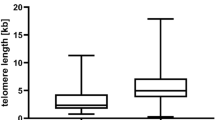
Median relative TL (5th–95th percentile distributions) was 0.85 (0.58–1.25) and 0.85 (0.58–1.23) for cases and controls, respectively (P=0.40, Wilcoxon rank sum test). A box plot showing the distribution of TL measurements among cases and controls is available online (Supplementary Figure 1). No differences in TL between cases and controls were observed after stratifying by material type. The expected age-related decline in TL was observed in both cases and controls. In multivariate analyses among controls, TL was significantly longer among African Americans than among Caucasians (P<0.001), and we observed a borderline significant association between hypertension and shorter TL (P=0.07; Table 1).
No overall associations between TL and RCC were observed (Table 2). Analyses stratified by sex, race, age, or other variables did not reveal any consistent subgroup-specific associations between TL and RCC. No differences in the relationship between TL and RCC by tumour stage (localised vs other) were observed, nor when we restricted our analysis to cases treated by surgery alone. We did not observe any differences in TL by days from RCC diagnosis to blood collection (adjusted β=−2.95 × 10−5; 95% CI: −9.01 × 10−5, 3.11 × 10−5), and risk estimates did not differ after stratifying by time since diagnosis (data not shown).
Discussion
The results of this case–control study do not support the hypothesis that blood TL is associated with RCC. Our study did not replicate findings from two hospital-based case–control studies with 32 and 65 RCC cases, respectively, that reported an inverse association between TL and RCC (Wu et al, 2003; Shao et al, 2007). Both prior studies measured TL using a Q-FISH assay; it has been demonstrated that Q-FISH measurements are highly correlated with measurements by the QPCR method used in this study (Cawthon, 2002). Because measurements in our study were highly reproducible in blind replicates (CV=9.9%), it is unlikely that measurement error could explain the difference in findings between our study and previous studies.
This population-based case–control study is, to our knowledge, the largest investigation of TL and RCC to date. We had 89% power to detect a trend in ORs with decreasing quartiles of TL assuming an OR of 1.5 comparing the lowest and highest quartiles. Our findings of shorter TL with increasing age and history of hypertension are consistent with previous reports (Demissie et al, 2006; Mirabello et al, 2009), which supports the validity of these findings. Differences in TL by race are inconsistent in previous studies (Hunt et al, 2008; Roux et al, 2009) and additional research is needed to confirm these findings. Numerous studies have investigated TL in relation to smoking and BMI (Wu et al, 2003; Valdes et al, 2005; Nordfjall et al, 2008; Kim et al, 2009; Mirabello et al, 2009; Fitzpatrick et al, 2011; Lee et al, 2011; Shen et al, 2011). Overall, the totality of the evidence linking these exposures to TL is inconsistent, with only some studies reporting inverse associations with smoking (Valdes et al, 2005; Mirabello et al, 2009; Fitzpatrick et al, 2011; Shen et al, 2011) and BMI (Valdes et al, 2005; Nordfjall et al, 2008; Kim et al, 2009; Lee et al, 2011).
Measurement of TL in samples collected retrospectively is an inherent limitation of case–control studies. Previous studies of various cancers have reported strong associations between short TL and cancer risk in retrospective studies but not in studies with prospective sample collection (Pooley et al, 2010; Wentzensen et al, 2011). However, in our study, we did not observe any differences in the relation between TL and RCC after stratifying by tumour stage, tumour grade, and time from RCC diagnosis to blood collection, nor when we restricted to cases treated by surgery only. Furthermore, Svenson et al (2009) found that among cases with non-metastatic disease (consistent with most of the cases included in our study) TL was not related to survival until >10 months after RCC diagnosis. Since the vast majority of samples in our study were collected from RCC cases within 10 months of diagnosis, we would not expect our findings to be biased as a result of differential survival. Moreover, since long TL was associated with poor survival, any bias due to a survival effect would be expected to exaggerate (rather than to obscure) an association between short TL and RCC risk. Given this evidence from our study and the analysis by Svenson et al (2009), it is unlikely that disease- or treatment-related changes in TL would have affected our findings. In conclusion, we found no evidence of an association between blood TL and RCC risk in this population-based case–control study, to our knowledge the largest such investigation to date.
Change history
29 March 2012
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Cawthon RM (2002) Telomere measurement by quantitative PCR. Nucleic Acids Res 30: e47
Colt JS, Schwartz K, Graubard BI, Davis F, Ruterbusch J, Digaetano R, Purdue M, Rothman N, Wacholder S, Chow WH (2011) Hypertension and risk of renal cell carcinoma among white and black Americans. Epidemiology 22 (6): 797–804
De Lange T (2005) Telomere-related genome instability in cancer. Cold Spring Harb Symp Quant Biol 70: 197–204
Demissie S, Levy D, Benjamin EJ, Cupples LA, Gardner JP, Herbert A, Kimura M, Larson MG, Meigs JB, Keaney JF, Aviv A (2006) Insulin resistance, oxidative stress, hypertension, and leukocyte telomere length in men from the Framingham Heart Study. Aging Cell 5: 325–330
Fitzpatrick AL, Kronmal RA, Kimura M, Gardner JP, Psaty BM, Jenny NS, Tracy RP, Hardikar S, Aviv A (2011) Leukocyte telomere length and mortality in the Cardiovascular Health Study. J Gerontol A Biol Sci Med Sci 66: 421–429
Hunt SC, Chen W, Gardner JP, Kimura M, Srinivasan SR, Eckfeldt JH, Berenson GS, Aviv A (2008) Leukocyte telomeres are longer in African Americans than in whites: the National Heart, Lung, and Blood Institute Family Heart Study and the Bogalusa Heart Study. Aging Cell 7: 451–458
Karami S, Schwartz K, Purdue MP, Davis FG, Ruterbusch JJ, Munuo SS, Wacholder S, Graubard BI, Colt JS, Chow WH (2010) Family history of cancer and renal cell cancer risk in Caucasians and African Americans. Br J Cancer 102: 1676–1680
Kim S, Parks CG, DeRoo LA, Chen H, Taylor JA, Cawthon RM, Sandler DP (2009) Obesity and weight gain in adulthood and telomere length. Cancer Epidemiol Biomarkers Prev 18: 816–820
Lee M, Martin H, Firpo MA, Demerath EW (2011) Inverse association between adiposity and telomere length: the Fels Longitudinal Study. Am J Hum Biol 23: 100–106
Mirabello L, Huang WY, Wong JY, Chatterjee N, Reding D, Crawford ED, De Vivo I, Hayes RB, Savage SA (2009) The association between leukocyte telomere length and cigarette smoking, dietary and physical variables, and risk of prostate cancer. Aging Cell 8: 405–413
Nordfjall K, Eliasson M, Stegmayr B, Melander O, Nilsson P, Roos G (2008) Telomere length is associated with obesity parameters but with a gender difference. Obesity (Silver Spring) 16: 2682–2689
Pooley KA, Sandhu MS, Tyrer J, Shah M, Driver KE, Luben RN, Bingham SA, Ponder BA, Pharoah PD, Khaw KT, Easton DF, Dunning AM (2010) Telomere length in prospective and retrospective cancer case-control studies. Cancer Res 70: 3170–3176
Roux AV, Ranjit N, Jenny NS, Shea S, Cushman M, Fitzpatrick A, Seeman T (2009) Race/ethnicity and telomere length in the Multi-Ethnic Study of Atherosclerosis. Aging Cell 8: 251–257
Shao L, Wood CG, Zhang D, Tannir NM, Matin S, Dinney CP, Wu X (2007) Telomere dysfunction in peripheral lymphocytes as a potential predisposition factor for renal cancer. J Urol 178: 1492–1496
Shen M, Cawthon R, Rothman N, Weinstein SJ, Virtamo J, Hosgood HD, Hu W, Lim U, Albanes D, Lan Q (2011) A prospective study of telomere length measured by monochrome multiplex quantitative PCR and risk of lung cancer. Lung Cancer 73: 133–137
Svenson U, Ljungberg B, Roos G (2009) Telomere length in peripheral blood predicts survival in clear cell renal cell carcinoma. Cancer Res 69: 2896–2901
Valdes AM, Andrew T, Gardner JP, Kimura M, Oelsner E, Cherkas LF, Aviv A, Spector TD (2005) Obesity, cigarette smoking, and telomere length in women. Lancet 366: 662–664
Wentzensen IM, Mirabello L, Pfeiffer RM, Savage SA (2011) The association of telomere length and cancer: a meta-analysis. Cancer Epidemiol Biomarkers Prev 20 (6): 1238–1250
Wu X, Amos CI, Zhu Y, Zhao H, Grossman BH, Shay JW, Luo S, Hong WK, Spitz MR (2003) Telomere dysfunction: a potential cancer predisposition factor. J Natl Cancer Inst 95: 1211–1218
Acknowledgements
This research was supported in part by the Intramural Research Program of the National Institutes of Health, National Cancer Institute, Division of Cancer Epidemiology and Genetics. We thank Kate Torres, Marsha Dunn, and other staff at Westat, Inc. and Stella Munuo and other staff at Information Management Services, Inc. for their efforts on this project. Finally, we express our gratitude to the participants in this study for their involvement.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
Dr Baccarelli receives salary support from New Investigator funding from the HSPH-NIEHS Center for Environmental Health (ES000002). The other authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on British Journal of Cancer website
Supplementary information
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Hofmann, J., Baccarelli, A., Schwartz, K. et al. Risk of renal cell carcinoma in relation to blood telomere length in a population-based case–control study. Br J Cancer 105, 1772–1775 (2011). https://doi.org/10.1038/bjc.2011.444
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2011.444
Keywords
This article is cited by
-
Leukocyte telomere length and renal cell carcinoma survival in two studies
British Journal of Cancer (2017)
-
The association between telomere length and cancer risk in population studies
Scientific Reports (2016)
