
Key Points
-
Highlights that detecting early complications can lead to more predictable treatment outcomes.
-
Aids an understanding that the patient can help with detecting disease.
-
Provides an understanding of what the patient can perceive and what they cannot in terms of detecting complications.
Abstract
Objectives This study investigated if the patient can have a role in reporting early peri-implant complications.
Design An exploratory, single-centred study comparing patient's perceptions of implant success to the clinical success at an examination.
Setting, materials and methods Seventy-five patients were randomly selected from patients who had received implant treatment at an implant referral practice. Phase 1 – Patient perception: Patients were asked to complete a questionnaire relating to the health of their implants. Phase 2 – Clinical examination: The patients were examined for implant health/disease.
Main outcome measures The responses from the patient perception questionnaires were correlated to the variables of the clinical examination. The null hypothesis 'Patients cannot perceive the difference between a successful implant and an implant that is suffering from complications' was then tested using Fisher's exact test.
Results All the variables tested statistically show a positive association between patient perception and clinical examination (p <0.001). All variables gave a significant result for Fisher's exact test. Therefore, the null hypothesis can be rejected.
Conclusions This study demonstrated that using validated questions an educated patient can perceive peri-implant health/disease. This can play a role in the early diagnosis of peri-implant complications.
Similar content being viewed by others

Objectives
Dental implants are a common treatment modality to replace missing teeth, and high survival rates in several 10-year, follow-up studies have encouraged their widespread prescription.1 However, with an increase in the provision of dental implants there is an increase in the number and frequency of patients that are affected by complications.1
This is further complicated by different stages of treatment often being carried out by multiple clinicians. This multi-disciplinary approach is encouraged; however, it makes follow up and auditing treatment outcomes more challenging, particularly when the maintenance and review is undertaken by GDPs with little or no training in the detection of peri-implant complications and disease
Implant complications, both mechanical and biological, can eventually lead to bone loss around the implant and ultimately implant loss.2 Hence, it is essential to detect and treat complications early, and although the data is limited for the treatment of peri-implant complications, there is evidence that an early diagnosis will allow an early intervention and a more predictable resolution.3,4,5 If early signs are missed, in particular with reference to peri-implant mucositis, this will develop into peri-implantitis which is more complicated and less predictable to treat.3,4,5
In this study we wanted to investigate if the patient can have a role in reporting complications early in order to achieve a more predictable treatment outcome. Therefore, the aim of this study was to determine if a patient who has received a dental implant could detect peri-implant complications.
Design
A consensus approach (nominal group technique) was undertaken to determine the most frequent complications associated with dental implant treatment. Based on these frequent complications, an exploratory, single-centred study was undertaken comparing patients perceptions of implant success to the clinical success at an examination.
Setting, materials and methods
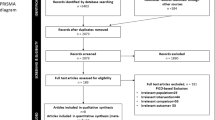
Seventy-five patients were randomly selected from patients who had received implant treatment at an implant referral practice on the Wirral in the last year. This was done by targeting every patient that had a pre-planned routine review appointment within an agreed time period. The patients either belonged to the practice or were referred from general dental practices for the placement of dental implants. The target group of patients consisted of patients with at least one implant and no complicating medical histories.
Patients were asked to give their informed consent to taking part, after being told the study would consist of them answering a questionnaire and undergoing a clinical examination. No patients declined to be involved. As this was part of their normal maintenance programme and they were not NHS patients, no ethical approval was required. The age range of the patients was 23–92 years, and were a mixture of male and female patients. Implants had been placed from a range of 1–11 months previously, by one of two dentists at the practice.
Interventions
Phase 1 – Patient perception
At the fit of the dental implant restoration, the patients were given standardised maintenance and advice both written and verbally. This was done as a routine protocol at the referral practice and was not modified for the study.
The patients were assessed as part of their normal recall programme. They were asked to complete a questionnaire relating to the health of their implants and peri-implant tissues (Table 1). Full instruction on how to complete the questionnaire was given and a member of staff, not the examiners, were available to help and collect the questionnaires.
The patients were given the assurance of anonymity and confidentially, as well as confirmation that they could stop completing the questionnaire at any time, without the need to give a reason. Clear and accurate contact details of who to approach for further information was given.
Phase 2 – Clinical examination
The patients were examined for implant health/disease (Table 2). The examiners did not have access to the patient questionnaires and did not see the answers given at any time.
The questionnaires were numbered to match the clinical examinations forms but patient names were not recorded. Two calibrated examiners carried out the clinical examinations by a defined protocol.
Main outcome measures
The responses from the patient perception questionnaires were correlated to the variables of the clinical examination (Table 3). Each variable was correlated to determine if there is an association between patient perception and the clinical examination using Phi correlation.
The null hypothesis 'Patients cannot perceive the difference between a successful implant and an implant that is suffering from complications' was then tested using Fisher's exact test.
The results were also presented as sensitivity and specificity of each particular response.
Results
Data collection
Twenty-eight of the respondents were male and 41 were female. Data was absent for six respondents as to their sex. This gives valid percentages of 40.6% of respondents were male and 59.4% respondents were female. Fifty-four (72.0%) of the implants were in the aesthetic zone, whereas 16 (21.3%) were not. Data was not recorded for one patient.
Results
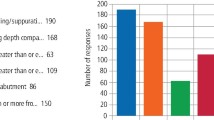
Table 4 shows the valid percentage frequencies of the positive and negative variables respectively. Correlations were statistically calculated for five variables that relate specifically to the implant and its restoration:
-
1
Aesthetics
-
2
Loose restorations
-
3
Bleeding and/or pus
-
4
Occlusion
-
5
Fractured restoration.
Table 5 shows the Phi coefficient for the five variables. All the five variables tested statistically show a positive association between patient perception and clinical examination (p <0.001). Aesthetics and loose restoration showed a strong positive correlation. Bleeding/pus, occlusion and fractured restoration show a good positive correlation.
Fisher's exact test
The null hypothesis: 'Patients cannot perceive the difference between a successful implant and an implant that is suffering from complications' was tested statistically using Fisher's exact test (Table 6). All five variables gave a significant result for Fisher's exact test. Therefore the null hypothesis can be rejected.
Sensitivity and specificity
Table 7 shows the sensitivity and specificity of five of the questionnaire responses (aesthetics, loose restoration, bleeding and/or pus, and fractured restoration).
Four out of the five questions produced sensitivity scores greater than 0.5 and all questions produced specificity scores of greater than 0.5. Hence patients with implant disease were correctly aware of problems in relation to aesthetics, loose restorations, presence of bleeding and/or pus, and fractured restorations (sensitivity scores: 1.0, 0.8, 0.6 and 1.0, respectively). However, in relation the question concerning occlusion, patients were not aware of problems when in fact problems were present (sensitivity score 0.25).
All five questions produced specificity scores above 0.5. Hence patients without implant disease were correctly aware of implant health in relation to aesthetics, loose restorations, presence of bleeding and/or pus, occlusion and fractured restorations (specificity scores: 0.99, 0.95, 0.97, 1.0 and 0.96, respectively).
Discussion
Early diagnosis is imperative for predictable treatment outcomes. In particular, it is stated that peri-implant mucositis is inflammation confined to the peri-implant soft tissue and is reversible;5 however, once allowed to progress to peri-implantitis treatment is less predictable and bone loss will occur.6,7 The purpose of this study was to aid early diagnosis, so complications can be treated predictably. This was effectively done via a self-reporting questionnaire.
Self-reporting questionnaires have been used previously for basic tooth conditions with varying degrees of success. Several have been used for periodontal disease.8 Gilbert and Nuttall8 found that correlations were weak between the self-assessment and the clinical evaluation and, therefore, should not be used as a substitute for a clinical evaluation. It is not the intention to use the questionnaire as a substitute for the clinical examination, merely to determine if it can help to aid an early diagnosis of peri-implant complications. Several studies have shown that patients can perceive oral health problems.8,9,10 Therefore, it is possible we could use self-perception as an aid to diagnosis of implant problems.
The questionnaire in this study consisted of ten questions asked to patients during a routine recall visit. Out of these questions and the variables of the examination, only six could be compared and used in the correlations and hypothesis testing. These related to aesthetics, loose restorations, bleeding and/or pus, oral hygiene, occlusion and fractured restorations.
All 75 patients thought they had adequate oral hygiene. This then meant that correlations and hypothesis testing could not be carried out using oral hygiene as a variable as it became a constant.
The frequencies of patient perception of a fractured restoration (5.3%) are higher than the actual frequency (1.3%) and this is the same for the variable of a loose restoration. Patient perception for a loose restoration is 14.7% compared to the 13.3% that were actually found to be loose. This is reversed with occlusion. Patient perception is lower (1.3%) than the actual examination (5.3%) for occlusal problems. This can perhaps be explained by the fact that patients can perceive a problem with the implant restoration but cannot describe the actual problem. It may be an occlusal issue but they perceive it as a loose or fractured restoration. They do, however, perceive a problem with the implant restoration.
Overall correlations were calculated using Phi correlation. The strongest associations were made between patient perception and the clinical examination for aesthetics and loose restorations (0.702 and 0.724, respectively). The reason for this may be that aesthetics are important to the patients. A loose implant is also easily perceived. There is also a good correlation between patient perception of bleeding and/or pus present, and the clinical situation (0.627), this means that patients are able to perceive peri-implant problems early on.
This study found that 72% of the implants were placed in the aesthetic zone and 21.3% in the non-aesthetic zone. Data were not recorded in 6.7% of cases. It is easier for a patient to monitor their anterior teeth compared to their posterior teeth, and patients are usually more concerned with teeth in the aesthetic zone compared to the non-aesthetic zone.11 This may have a bearing on why we obtained a positive association for patient perception for all the variables tested. Further research should be undertaken in relation to the implant position.
The null hypothesis 'Patients cannot perceive the difference between a successful implant and an implant that is suffering from complications' can be rejected according to the results of the Fisher's exact test. The Fisher's exact test produced significant results for all five variables tested. Three of the results (aesthetics, loose restoration, and bleeding and/or pus) were below p <0.05 level, and two (occlusion and fractured restoration) were 0.05, hence significant at p <0.1. The alternative hypothesis can be accepted that a patient can perceive implant health and more importantly implant disease. This, therefore, can help lead to an early diagnosis of implant problems and early treatment of such problems.
It is important to note that all the patients were appropriately educated in implant care following placement, and before placement they were assessed for risks and understood the nature of implant treatment.
The study shows patients are able to perceive implant problems/disease. To determine if a questionnaire may be used to prompt the patient to assess the health, sensitivity and specificity tests were applied to five questions used in the other statistical tests:
-
1
Are you happy with the appearance of your implants?
-
2
Do any of the restorations feel loose?
-
3
Does the gum around any of your implants bleed or discharge any pus or fluid?
-
4
Does the 'bite' feel normal when you close your teeth together?
-
5
Has anything broken or fractured from your restoration?
The sensitivity and specificity values for all the questions, except the question for the 'bite', are above 0.5 and are therefore sufficient to enable the development of a question set which would be satisfactory as an indicator for patient perception of implant health/disease problems. Patients were unable to determine problems with the bite and, therefore, this question should not be used (sensitivity 0.25).
Thus, we may use the questionnaire (self-perception) as an aid to an early diagnosis. It is not reliable alone or as a substitute for the clinical examination.8 However, the clinician can be alerted to a perceived problem and follow up the results of the questionnaire with a clinical examination.
Conclusions
Implications for practice
This study demonstrated that important clinical parameters in the diagnosis of peri-implant complications can be assessed using the following validated questions:
-
Are you happy with the appearance of your implant?
-
Do any of the restorations feel loose?
-
Does the gum around any of your implants bleed or discharge any pus or fluid?
-
Has anything broken or fractured from your restorations?
A patient can perceive peri-implant health and disease, and the use of these questions should allow them to play a major role in the early diagnosis of peri-implant complications.12 An early diagnosis of peri-implant complications allows treatment to be carried out predictably before progression for which treatment is less predictable and less successful.13
Using these questions, a patient feedback tool can be produced to aid early reporting of complications. Patients can use this in their own time in between review appointments and contact the dentist if an implant problem is flagged or perceived. The patient will then undergo a clinical examination to confirm a problem and receive the necessary treatment.
Implications for research
More research with a larger sample size is needed to fully evaluate the role of patient perception in implant health and implant disease. A larger sample size will allow correlations using Pearson's correlation coefficient and the Pearson Chi-square test rather than using Phi and Fisher's exact test.
Research could be carried out to determine patients' perception of implant health and disease according to the position of the implant in the mouth. Implant position may have an effect on patient perception. For example, patients are able to observe anterior teeth more easily than posterior teeth and are more concerned by teeth in the aesthetic zone compared to the non-aesthetic zone. Thus, patients may be able to perceive implant health and disease in the anterior regions to a greater extent than posterior regions.
Further research is required to investigate the reproducibility and validity of the role of patient perception in the early diagnosis of peri-implant complications.
References
Albrektsson T, Zarb G, Worthington P, Eriksson A R . 1986. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. Int J Oral Maxillofac Implants 1986; 1: 11–25.
Heasman P, Esmail Z, Barclay C . Peri-implant diseases. Dent Update 2010; 37: 511–512, 514–516.
Heitz-Mayfield L J . Diagnosis and management of peri-implant diseases. Aust Dent J 2008; 53: S43–S48.
Algraffee H, Borumandi F, Cascarini L . Peri-implantitis. Br J OralMaxillofac Surg 2012; 50: 689–694.
Zeza B, Pilloni A . Peri-implant mucositis treatments in humans: a systematic review. Ann Stomatol (Roma) 2012; 3: 83–89.
Serino G, Turri A, Lang N P . Probing at implants with peri-implantitis and its relation to clinical peri-implant bone loss. Clin Oral Implants Res 2013; 24: 91–95.
Heitz-Mayfield L J . Peri-implant diseases: diagnosis and risk indicators. J Clin Perio 2008; 35: 292–304.
Gilbert A D, Nuttall N M . Self-reporting of periodontal health status. Br Dent J 1999; 186: 241–244.
Pinelli C, de Castro Monteiro Loffredo L . Reproducibility and validity of self-perceived oral health conditions. Clin Oral Investig 2007; 11: 431–437.
McGrath C, Lam O, Lang N . An evidence-based review of patient-reported outcome measures in dental implant research among dentate subjects. J Clin Periodontol 2012; 39: 193–201.
Tomasi C, Derks J . Clinical research of peri-implant diseases quality of reporting, case definitions and methods to study incidence, prevalence and risk factors of peri-implant diseases. J Clin Periodontol 2012; 39: 207–223.
Graziani F, Figuero E, Herrera D . Systematic review of quality of reporting, outcome measurements and methods to study efficacy of preventive and therapeutic approaches to peri-implant diseases. J Clin Periodontol 2012; 39: 224–244.
Lang N P, Berglundh T, Working Group 4 of Seventh European Workshop on Periodontology. Periimplant diseases: where are we now? Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol 2011; 38: 178–181.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Wright, S., Archer, C. An exploratory study to investigate if patients are able to aid the early diagnosis of peri-implant complications. Br Dent J 218, 637–640 (2015). https://doi.org/10.1038/sj.bdj.2015.503
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2015.503
