
Abstract
The lymphocyte-to-monocyte ratio (LMR) has been reported to predict clinical outcomes in multiple malignancies. The aim of this study was to assess the prognostic role of pretreatment LMR in hepatocellular carcinoma (HCC). A total of seven studies comprising 2,738 patients were included in the meta-analysis. Pooled results showed that elevated LMR was significantly associated with increased overall survival (OS) (HR: 0.31, 95% CI: 0.20–0.47, p < 0.001), disease-free survival (DFS)/recurrence-free survival (RFS) (HR: 0.57, 95% CI: 0.49–0.67, p < 0.001). The favorable prognostic impact of high LMR on OS was observed in all subgroup with different sample size, type of publication, NOS score, and the cut-off value of LMR. In addition, low LMR was significantly correlated with TNM stage and BCLC stage. We therefore conclude that elevated pretreatment LMR could be a favorable prognostic factor for clinical outcomes in patients with HCC.
Similar content being viewed by others
Introduction
According to the American Cancer Society, hepatocellular carcinoma (HCC) is the fifth most common malignancy and the second cause of cancer-related mortality in the United States in 20151,2. Around the world, there were an estimated 500,000 to 1 million people died of HCC per year3. Liver resection is the most effective therapy for the majority of patients with resectable HCC, but unfortunately most of patients are not eligible for curative resection at the time of diagnosis4. In addition, postoperative recurrence rate for patients with early stage HCC can be high at 50% to 70% after liver resection5. Therefore, the overall prognosis of HCC patients remains poor. It is vital to develop novel potential biomarker to select appropriate treatment strategies and predict prognosis.
Systemic inflammatory responses can largely influence the formation and recurrence of HCC6,7,8. Several inflammatory biomarkers, such as neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), and platelet-to-lymphocyte ratio (PLR) are identified as prognostic indicators in a wide variety of solid tumors9,10,11,12. These tests are simple and inexpensive to perform, and they are readily available in daily oncologic practice. LMR is a readily available, routinely measured, and inexpensive inflammatory biomarker, which can be easily applied into in daily oncologic practice. Accumulating evidence shows that lymphocytes are known to play a crucial role in suppressing HCC progression through immunoselection in an immunosuppressive network, which dictates immune responses to tumors13. A low lymphocyte count is associated with the systemic inflammatory responses and is known to promote cancer progression through effects upon cell-mediated immunity14. Conversely, activated circulating monocytes can secrete multiple proinflammatory cytokines, which are involved in tumor development and progression15,16. As a consequence high monocyte counts are associated with microvascular invasion and poor prognosis in patients with HCC17. Moreover, a high LMR, which is defined as absolute lymphocyte counts divided by monocyte counts, is reported to correlate with favorable prognosis in patients with HCC18,19.
Nevertheless, there has been no meta-analysis to assess the correlation between pretreatment LMR and the survival of HCC patients. Therefore, we conducted a meta-analysis to assess the effects of pretreatment LMR on OS and DFS/RFS in HCC. In addition, the correlations between LMR and the clinicopathological features was also examined.
Materials and Methods
Search strategies
We searched MEDLINE, EMBASE, PubMed, and Cochrane databases from inception up to February 2017. Search terms included “HCC” or “hepatocellular carcinoma” or “liver cancer” or “liver tumor” or “liver neoplasms” or “liver cell carcinoma”, “LMR” or “lymphocyte monocyte ratio” or “lymphocyte to monocyte ratio” or “lymphocyte-to-monocyte ratio” or “lymphocyte-monocyte ratio”, “survival” or “prognostic” or “prognosis” or “recurrence” or “clinical outcome”. The references of eligible studies, relevant systematic reviews and meta-analyses in this field were manually retrieved.
Inclusion criteria
The criteria for inclusion were listed as follows: (1) the diagnosis of HCC were confirmed by pathology; (2) studies assessing the association of pretreatment LMR with OS, DFS/RFS, or CSS; (3) the cut-off value of LMR was reported; and (4) studies supplied sufficient information for calculating hazard ratio (HR) and 95% confidence interval (CI).
Exclusion criteria
The exclusion criteria were as follows: (1) reviews, letters, case reports, and comments; (2) reporting insufficient data for calculating an HR and 95% CI; and (3) overlapping or duplicate data.
Data extraction and Assessment of risk of bias
The two reviewers independently reviewed all eligible studies and extracted data. Any disagreement was resolved by a third reviewer. The following information was captured using data abstraction forms:
Study characteristics included first author’s name, year of publication, study design (prospective or retrospective), type of publication, country, ethnicity, survival analysis methods (multivariate, univariate), and time of follow-up. Patient characteristics included patient ages and genders, number of patients, disease stage, treatment, and cut-off value. Outcome measures included HRs for OS, DFS, RFS, or CSS as well as their 95% CIs. HRs were extracted from multivariate or univariate analyses or estimated from Kaplan-Meier survival curves20.
The study quality was evaluated in accordance with the Newcastle-Ottawa Scale (NOS)21. This included an assessment of subject selection, comparability of groups, and clinical outcome. A total of nine items were extracted and each item scored 1. The maximum score is 9 and those studies with a NOS score ≥7 were considered as high-quality studies.
Statistical analysis
The meta-analysis was conducted using RevMan 5.3 software (Cochrane Collaboration, Copenhagen, Denmark). Heterogeneity between studies was estimated using Cochrane’s Q statistic and I2 statistic22. A p-value < 0.1 for the Q-test or I2 > 50% indicated significant heterogeneity. When there was no statistically significant heterogeneity, we used the fixed-effects model for pooling the results; otherwise, the random-effects model was applied. HRs and their 95% CIs were searched in the original articles or extrapolated using methods described by Tierney and Parmar20,23. The log HR and standard error (SE) were used for aggregation of the survival results23. The associations between LMR and clinicopathologic features were expressed as odds ratios (ORs) and its 95% CIs. P < 0.05 was defined as statistically significant. Subgroup analyses were conducted for: the sample size, type of publication, NOS score, and the cut-off value of LMR. Sensitivity analyses were carried out to evaluate result stability excluding each study.
Results
Search results
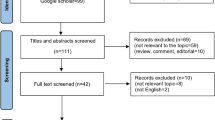
Our search strategy yielded 63 potentially relevant records. After duplicates removal (21 records), 42 articles were screened for eligibility. Of these, 32 were excluded through titles and abstracts, leaving 10 articles for further evaluation. Subsequently, 3 articles did not meet the inclusion criteria and were therefore excluded. Eventually, seven studies, comprising a total of 2,507 patients, were considered eligible for the present meta-analysis18,24,25,26,27,28,29. The PRISMA flow diagram of the study selection process was shown in Fig. 1.

Flow diagram of the study selection process.
Characteristics of the included studies
According to the publication type, 6 and 1 studies were published in full-text and abstract forms, respectively. All included studies were from China and were published between 2014 and 2017. The sample sizes ranged from 208 to 1,020. There were six studies for OS, and all for DFS/RFS. The cut-off values for LMR ranged from 0.83 to 3.77. All included studies consisted of two groups: high and low LMR. HR and 95% CI was extracted directly from the seven studies. In methodological quality of studies, the NOS scores of the included studies ranged from 5 to 8. Detailed patient characteristics and methodological quality are shown in Table 1.
Meta-analysis
LMR and OS in HCC
Six of the included studies reported the data of LMR and OS in HCC. Overall, elevated LMR had a significant association with increased OS (HR: 0.31, 95% CI: 0.20–0.47, p < 0.001) with significant heterogeneity (p = 0.002, I2 = 74%; Fig. 2).

Forest plots for the association between LMR and OS.
To detect the potential heterogeneity, subgroup analyses stratified by sample size, type of publication, NOS score, and the cut-off value of LMR (Table 2). Subgroup analysis revealed that high LMR predicted increased OS in patient with HCC, regardless of the sample size (≥300 and <300), type of publication (full-text and abstract), NOS score (≥7 and <7), and the cut-off value of LMR (≥3 and <3).
LMR and DFS/RFS in HCC
All included studies reported the data of LMR and DFS/RFS in HCC. A combined analysis demonstrated that elevated LMR was significantly correlated with increased DFS/RFS (HR: 0.57, 95% CI: 0.49–0.67, p < 0.001), with no significant heterogeneity between studies (p = 0.21, I2 = 28%; Fig. 3).

Forest plots for the association between LMR and DFS/RFS.
LMR and clinicopathological features
To further explore the impact of LMR on the clinical features in HCC, we identified 9 clinical factors in HCC. The pooled analysis demonstrated that low LMR was significantly correlated with TNM stage (III-IV vs. I-II; HR = 1.78, 95% CI: 1.19–2.68, P = 0.005) and BCLC stage (B/C vs. A; HR = 1.70, 95% CI: 1.21–2.39, P = 0.002). Whereas no significant association was found with gender, AFP, liver cirrhosis, tumor differentiation, tumor number, tumor size, and vascular invasion. The correlation between LMR expression and clinicopathological parameters of HCC is shown in Table 3.
Sensitivity analysis
In order to assess the influence of single studies on the overall estimate, the sensitivity analysis was performed. Each single study was removed each time to estimate the influence of individual data sets on the combined HR for OS. The results showed that no study had a significant effect on the observed effect size (pooled HR), indicating the robustness of our findings.
Discussion
Hepatocellular carcinoma (HCC) is mainly caused by viral infections such as hepatitis B virals (HBV) and hepatitis C virals (HCV)3. Mounting studies indicated that infiltration of inflammatory cells in the tumor microenvironment significantly affected the biological behavior of HCC25. In the tumor microenvironment, the inflammatory immune cells have been implicated in HCC progression30,31. The pretreatment LMR, as a promising inflammatory biomarker, is reportedly linked to prognosis in patients with HCC18,19,28. Therefore, LMR may serve as a promising prognostic factors for HCC patients. To our knowledge, this is the first meta-analysis to investigate the prognostic effect of pretreatment LMR in HCC.
Our meta-analysis provides strong evidence that the presence of high LMR significantly increases OS and DFS/RFS in patients with HCC. Stratified analysis demonstrated that high LMR was significantly correlated with increased OS in patient with HCC, regardless of the sample size, type of publication, NOS score, and the cut-off value of LMR. In addition, we further assessed the correlation between pretreatment LMR and clinicopathological features. The pooled data showed low LMR was linked with TNM stage and BCLC stage. Therefore, pretreatment LMR may serve as a promising prognostic biomarker for estimating HCC prognosis. Furthermore, we also performed sensitivity analysis and found that no study had a significant effect on the observed effect size (pooled HR), indicating the robustness of our findings.
The exact molecular mechanisms responsible for the prognostic impact of LMR in HCC are unclear. It has been suggested that cross-talk between the inflammatory response and tumor progression play a critical role in the initiation and progression of HCC14,32,33. In the tumor microenvironment, inflammatory infiltrates have a large influence on the biological behavior of HCC34,35. Tumor-infiltrating lymphocytes (TILs), as representative component of the immune microenvironment, are implicated in several stages of HCC progression, and TIL phenotypes may be a predictor for favorable prognosis36,37. Conversely, low lymphocyte counts might result in an insufficient immunological reaction, which lead to inferior survival in multiple cancers38,39. In addition, infiltrated CD4+ and CD8+ T cells interaction among each other are essential to the antitumor immune response by inducing tumor cell apoptosis40,41. Monocytes infiltrating tumor tissue are also involved in HCC development and progression42. Activated monocytes in HCC microenvironments can trigger and polarize T-cell responses and faciliate inflammation-induced tumor development43. Tumor-associated macrophages (TMAs) are derived from circulating monocytes. TAMs can accelerate HCC cell proliferation, tumor-associated angiogenesis, and metastasis30,37,44. Several studies showed that high infiltration of TAMs predicted decreased survival in various cancers45,46. Given this background, the observed favorable of high pretreatment LMR on OS of cancer patients may reflect the critical function of LMR in an inflammatory tumor microenvironment that inhibits tumor progression.
Nevertheless, there were several limitations to the present study. First, excessive heterogeneity existed among studies. Subgroup analyses didn’t find the potential sources of heterogeneity. In addition, we performed sensitivity analysis. The results showed that no study had a significant effect on the observed effect size. Second, the cut-off value for LMR was not unified in each study. Third, all included studies were retrospective analysis. Fourth, all included studies were from China, which limited our conclusions for other ethnic populations.
In conclusion, our findings demonstrated that an elevated pretreatment LMR is associated with favorable outcomes in patients with HCC.
Additional Information
How to cite this article: Song, W. et al. The pretreatment lymphocyte to monocyte ratio predicts clinical outcome for patients with hepatocellular carcinoma: A meta-analysis. Sci. Rep. 7, 46601; doi: 10.1038/srep46601 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Torre, L. A. et al. Global cancer statistics, 2012. CA Cancer J. Clin. 65, 87–108, doi: 10.3322/caac.21262 (2015).
Society, A. C. Cancer Facts & Figures 2015. Atlanta, GA: American Cancer Society 10–15 (2015).
Forner, A., Llovet, J. M. & Bruix, J. Hepatocellular carcinoma. Lancet 379, 1245–1255, doi: 10.1016/s0140-6736(11)61347-0 (2012).
Bruix, J. & Sherman, M. Management of hepatocellular carcinoma: an update. Hepatology (Baltimore, Md.) 53, 1020–1022, doi: 10.1002/hep.24199 (2011).
Liver, E. A. f. t. S. o. t. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. European journal of cancer (Oxford, England: 1990) 48, 599–641, doi: 10.1016/j.ejca.2011.12.021 (2012).
Chen, L. et al. Viral and host inflammation-related factors that can predict the prognosis of hepatocellular carcinoma. European journal of cancer (Oxford, England: 1990) 48, 1977–1987, doi: 10.1016/j.ejca.2012.01.015 (2012).
Barash, H. et al. Accelerated carcinogenesis following liver regeneration is associated with chronic inflammation-induced double-strand DNA breaks. Proc. Natl. Acad. Sci. USA 107, 2207–2212, doi: 10.1073/pnas.0908867107 (2010).
Kuang, D. M. et al. Peritumoral neutrophils link inflammatory response to disease progression by fostering angiogenesis in hepatocellular carcinoma. Journal of hepatology 54, 948–955, doi: 10.1016/j.jhep.2010.08.041 (2011).
Tian, X. C., Liu, X. L., Zeng, F. R., Chen, Z. & Wu, D. H. Platelet-to-lymphocyte ratio acts as an independent risk factor for patients with hepatitis B virus-related hepatocellular carcinoma who received transarterial chemoembolization. Eur. Rev. Med. Pharmacol. Sci. 20, 2302–2309 (2016).
Nakamura, K. et al. Neutrophil to lymphocyte ratio in the pre-treatment phase of final-line chemotherapy predicts the outcome of patients with recurrent ovarian cancer. Oncol. Lett. 11, 3975–3981, doi: 10.3892/ol.2016.4513 (2016).
Glazer, E. S., Rashid, O. M., Pimiento, J. M., Hodul, P. J. & Malafa, M. P. Increased neutrophil-to-lymphocyte ratio after neoadjuvant therapy is associated with worse survival after resection of borderline resectable pancreatic ductal adenocarcinoma. Surgery, doi: 10.1016/j.surg.2016.04.039 (2016).
Ozawa, T. et al. Impact of a lymphocyte to monocyte ratio in stage IV colorectal cancer. The Journal of surgical research 199, 386–392, doi: 10.1016/j.jss.2015.06.014 (2015).
Schreiber, R. D., Old, L. J. & Smyth, M. J. Cancer immunoediting: integrating immunity’s roles in cancer suppression and promotion. Science 331, 1565–1570, doi: 10.1126/science.1203486 (2011).
Grivennikov, S. I., Greten, F. R. & Karin, M. Immunity, inflammation, and cancer. Cell 140, 883–899, doi: 10.1016/j.cell.2010.01.025 (2010).
Balkwill, F. Tumour necrosis factor and cancer. Nat. Rev. Cancer 9, 361–371 (2009).
Lippitz, B. E. & Harris, R. A. Cytokine patterns in cancer patients: A review of the correlation between interleukin 6 and prognosis. Oncoimmunology 5, e1093722, doi: 10.1080/2162402x.2015.1093722 (2016).
Ding, T. et al. High tumor-infiltrating macrophage density predicts poor prognosis in patients with primary hepatocellular carcinoma after resection. Hum. Pathol. 40, 381–389, doi: 10.1016/j.humpath.2008.08.011 (2009).
Liao, R. et al. Systemic and intratumoral balances between monocytes/macrophages and lymphocytes predict prognosis in hepatocellular carcinoma patients after surgery. Oncotarget, doi: 10.18632/oncotarget.9049 (2016).
Neal, C. P. et al. Prognostic performance of inflammation-based prognostic indices in patients with resectable colorectal liver metastases. Medical Oncology 32, 144 (2015).
Parmar, M. K., Torri, V. & Stewart, L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat. Med. 17, 2815–2834 (1998).
Wells, G., Shea, B. & O’Connell, D. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses (2013).
Higgins, J., Thompson, S., Deeks, J. & Altman, D. Statistical heterogeneity in systematic reviews of clinical trials: a critical appraisal of guidelines and practice. J. Health Serv. Res. Policy 7, 51–61 (2002).
Tierney, J. F., Stewart, L. A., Ghersi, D., Burdett, S. & Sydes, M. R. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 8, 16, doi: 10.1186/1745-6215-8-16 (2007).
Li, G. J., Ji, J. J., Yang, F., Xu, H. W. & Bai, Y. Preoperative lymphocyte-to-monocyte ratio predicts survival in primary hepatitis B virus-positive hepatocellular carcinoma after curative resection. Onco Targets Ther. 10, 1181–1189, doi: 10.2147/ott.s110411 (2017).
Lin, Z. X. et al. Lymphocyte-to-monocyte ratio predicts survival of patients with hepatocellular carcinoma after curative resection. World journal of gastroenterology: WJG 21, 10898–10906, doi: 10.3748/wjg.v21.i38.10898 (2015).
Lin, Z. X. et al. Prognostic value of preoperative lymphocyte-to-monocyte ratio in patients with hepatocellular carcinoma after curative resection. Journal of Clinical Oncology. Conference 32 (2014).
Tang, T., Liao, R., Li, J. & Du, C. Y. Analysis of prognostic factors of patients with hepatocellular carcinoma after radical resection. Zhonghua wai ke za zhi [Chinese journal of surgery] 54, 439–443, doi: 10.3760/cma.j.issn.0529-5815.2016.06.010 (2016).
Wu, S. J. et al. Lymphocyte to monocyte ratio and prognostic nutritional index predict survival outcomes of hepatitis B virus-associated hepatocellular carcinoma patients after curative hepatectomy. Journal of surgical oncology 114, 202–210, doi: 10.1002/jso.24297 (2016).
Yang, T. et al. Lymphocyte to monocyte ratio and neutrophil to lymphocyte ratio are superior inflammation-based predictors of recurrence in patients with hepatocellular carcinoma after hepatic resection. Journal of surgical oncology, doi: 10.1002/jso.24549 (2017).
Mano, Y. et al. Tumor-associated macrophage promotes tumor progression via STAT3 signaling in hepatocellular carcinoma. Pathobiology 80, 146–154, doi: 10.1159/000346196 (2013).
Kong, L. Q. et al. The clinical significance of the CD163+ and CD68+ macrophages in patients with hepatocellular carcinoma. PloS One 8, e59771, doi: 10.1371/journal.pone.0059771 (2013).
Palumbo, J. S. & Degen, J. L. Mechanisms coupling the hemostatic system to colitis-associated cancer. Thrombosis research 125 Suppl 2, S39–43, doi: 10.1016/s0049-3848(10)70011-6 (2010).
Mantovani, A., Allavena, P., Sica, A. & Balkwill, F. Cancer-related inflammation. Nature 454, 436–444, doi: 10.1038/nature07205 (2008).
Allavena, P., Sica, A., Solinas, G., Porta, C. & Mantovani, A. The inflammatory micro-environment in tumor progression: the role of tumor-associated macrophages. Crit. Rev. Oncol. Hematol. 66, 1–9, doi: 10.1016/j.critrevonc.2007.07.004 (2008).
Peng, S. H. et al. Significance and relationship between infiltrating inflammatory cell and tumor angiogenesis in hepatocellular carcinoma tissues. World journal of gastroenterology: WJG 11, 6521–6524 (2005).
Chen, K. J. et al. Intratumoral regulatory T cells alone or in combination with cytotoxic T cells predict prognosis of hepatocellular carcinoma after resection. Med. Oncol. 29, 1817–1826, doi: 10.1007/s12032-011-0006-x (2012).
Zhou, J. et al. Increased intratumoral regulatory T cells are related to intratumoral macrophages and poor prognosis in hepatocellular carcinoma patients. Int. J. Cancer 125, 1640–1648, doi: 10.1002/ijc.24556 (2009).
Hoffmann, T. K. et al. Spontaneous apoptosis of circulating T lymphocytes in patients with head and neck cancer and its clinical importance. Clinical cancer research: an official journal of the American Association for Cancer Research 8, 2553–2562 (2002).
Vayrynen, J. P. et al. Detailed analysis of inflammatory cell infiltration in colorectal cancer. British journal of cancer 109, 1839–1847, doi: 10.1038/bjc.2013.508 (2013).
Rosenberg, S. A. Progress in human tumour immunology and immunotherapy. Nature 411, 380–384, doi: 10.1038/35077246 (2001).
Zikos, T. A., Donnenberg, A. D., Landreneau, R. J., Luketich, J. D. & Donnenberg, V. S. Lung T-cell subset composition at the time of surgical resection is a prognostic indicator in non-small cell lung cancer. Cancer Immunol. Immunother. 60, 819–827, doi: 10.1007/s00262-011-0996-4 (2011).
Lee, S. D., Kim, S. H., Kim, Y. K., Lee, S. A. & Park, S. J. Prognostic significance of preoperative peripheral blood monocyte ratio in patients with hepatocellular carcinoma. World journal of surgery 38, 2377–2385, doi: 10.1007/s00268-014-2545-8 (2014).
Kuang, D. M. et al. Activated monocytes in peritumoral stroma of hepatocellular carcinoma promote expansion of memory T helper 17 cells. Hepatology (Baltimore, Md.) 51, 154–164, doi: 10.1002/hep.23291 (2010).
Chanmee, T., Ontong, P., Konno, K. & Itano, N. Tumor-associated macrophages as major players in the tumor microenvironment. Cancers (Basel) 6, 1670–1690, doi: 10.3390/cancers6031670 (2014).
Ishigami, S. et al. Tumor-associated macrophage (TAM) infiltration in gastric cancer. Anticancer research 23, 4079–4083 (2003).
Lin, J. Y., Li, X. Y., Tadashi, N. & Dong, P. Clinical significance of tumor-associated macrophage infiltration in supraglottic laryngeal carcinoma. Chin. J. Cancer 30, 280–286 (2011).
Acknowledgements
We acknowledge all clinical researchers of the selected studies and patients related to these studies.
Author information
Authors and Affiliations
Contributions
W.S. and S.B.Z. conceived and designed the study. W.S., C.T. and R.J.Z. searched databases and collected the data. W.S., C.T. and K.W. analyzed and interpreted the data. W.S., C.T., K.W. and S.B.Z. wrote the manuscript. All authors reviewed the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Song, W., Tian, C., Wang, K. et al. The pretreatment lymphocyte to monocyte ratio predicts clinical outcome for patients with hepatocellular carcinoma: A meta-analysis. Sci Rep 7, 46601 (2017). https://doi.org/10.1038/srep46601
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep46601
This article is cited by
-
Development of nomogram models of inflammatory markers based on clinical database to predict prognosis for hepatocellular carcinoma after surgical resection
BMC Cancer (2022)
-
Prognostic utility of systemic inflammatory markers and chronic hepatitis C virus infection status in hepatocellular carcinoma patients treated with local ablation
BMC Cancer (2022)
-
Inflammatory indexes in preoperative blood routine to predict early recurrence of hepatocellular carcinoma after curative hepatectomy
BMC Surgery (2021)
-
The association of neutrophil-lymphocyte ratio and lymphocyte-monocyte ratio with 3-month clinical outcome after mechanical thrombectomy following stroke
Journal of Neuroinflammation (2020)
-
Lymphocyte to monocyte ratio-based nomogram for predicting outcomes of hepatocellular carcinoma treated with sorafenib
Hepatology International (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
