
Abstract
We investigated the association of physical activity, TV watching time, sleeping time with the risks of obesity and hyperglycemia among 1263 offspring aged 1–5 years of mothers with gestational diabetes (GDM) in a cross-sectional study. Logistic regression models were used to obtain the odd ratios (ORs) (95% confidence intervals [CI]) of childhood obesity and hyperglycemia associated with different levels of indoor activity, outdoor activity, TV watching, and sleeping time. The multivariable-adjusted ORs of obesity based on different levels of TV watching time (0, <1.0, and ≥1.0 hour/day) were 1.00, 1.21 (95% CI 0.72–2.05), and 2.20 (95% CI 1.33–3.63) (Ptrend = 0.003), respectively. The multivariable-adjusted ORs of hyperglycemia based on different levels of indoor activity (<5.0, 5.0–6.9, and ≥7.0 hours/day) were 1.00, 0.74 (95% CI 0.45–1.21), and 0.49 (95% CI 0.28–0.84) (Ptrend = 0.034), respectively. The multivariable-adjusted ORs of hyperglycemia associated with different levels of sleeping time (<11.0, 11.0–11.9, and ≥12.0 hours/day) were 1.00, 0.67 (95% CI 0.42–1.05), and 0.39 (95% CI 0.23–0.67) (Ptrend = 0.003), respectively. The present study indicated a positive association of TV watching with the risk of obesity, and an inverse association of either indoor activity or sleeping time with the risk of hyperglycemia among offspring born to GDM mothers in Tianjin, China.
Similar content being viewed by others

Introduction
It is widely acknowledged that obesity has become a leading public health problem all over the world1,2. Especially the prevalence of obesity among children and adolescents which is increasing at an alarming rate is critical3, not only because obese children tend to become obese adults4,5, but also they are more likely to suffer from hyperlipidemia, hypertension, insulin resistance, respiratory problems and orthopedic complications than non-obese children6. In China, with the rapid economic development and urbanization, Chinese people’s lifestyle changed tremendously in recent years, which resulted in an increasing prevalence of obesity, and the prevalence of overweight/obesity in the urban population has reached the same level as that of some developed countries7. The International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE) has shown that the prevalence of obesity among Chinese children is far greater than the average of 12 countries8,9. Many studies showed evidence that the increased prevalence of childhood obesity has been attributed largely to behavioral and environment factors10. Thus identifying risk factors at early time and developing effective intervention programs might be a significant strategy for obesity prevention.
Several studies have found that decreases in physical activity and increases in sedentary behavior, such as TV viewing and video/computer use, blame on the secular trends in obesity among children8,9. A recent study found that short sleep duration was associated with a higher risk of childhood obesity11, however, another cohort study found that sleep restriction did not increase future risk of obesity12. Few studies assessed this association among children less than 5 years old, but the results remain elusive13. Understanding this question is very important because eating and physical activity habits that contribute to later obesity become established during formative pre-school years (2–6 years old) and these habits are more malleable at this time than in later childhood14. Moreover, the associations of physical activity, sedentary behavior, sleeping time with the risk of childhood obesity among the offspring of gestational diabetes mellitus (GDM) mothers are not clear. It has been shown that offspring of mothers exposed to GDM were at increased risk of neonatal adiposity and childhood obesity15,16,17,18, thus assessing different types of physical activity with the risk of obesity among offspring of mothers exposed to GDM is important, which might improve early intervention among these children. The purpose of this study is to investigate the association of physical activity, TV watching time, and sleeping time with the risks of obesity, central obesity and hyperglycemia among the offspring aged 1–5 years of GDM mothers who participated in the Tianjin Gestational Diabetes Mellitus Prevention Program (TGDMPP)19.
Results
Of 1263 children, the prevalence of obesity, central obesity, and hyperglycemia were 10.1%, 10.0%, and 10.0%, respectively. General characteristics of both mothers and children according to different childhood obesity, center obesity and hyperglycemia status are presented in Table 1.
The multivariable-adjusted ORs (model 1) of obesity associated with different levels of childhood TV watching time (0, <1.0, and ≥1 hour per day) were 1.00, 1.25 (95% CI 0.74–2.09), and 2.31 (95% CI 1.41–3.80) (Ptrend = 0.001) (Table 2). After further adjustment for indoor activity, outdoor activity and sleeping time (multivariable-adjusted model 2), this positive association was still significant (Ptrend = 0.003). There were no associations of indoor activity, outdoor activity, and sleeping time with the risk of childhood obesity.
The multivariable-adjusted ORs (model 1) of central obesity associated with different levels of childhood TV watching time (0, <1.0, ≥1.0 hour per day) were 1.00, 1.28 (95% CI 0.78–2.08), and 1.76 (95% CI 1.08–2.88) (Ptrend = 0.071) (Table 3). After additional adjustment for indoor activity, outdoor activity and sleeping time (multivariable-adjusted model 2), children who watched ≥1.0 hour TV per day had 73% (95% 1.05–2.84) high risk of central obesity compared with those who did not watch TV. There were no associations of indoor activity, outdoor activity, and sleeping time with the risk of central obesity.
Table 4 showed the associations of different levels of indoor activity, outdoor activity, TV watching time and sleeping time with the risk of hyperglycemia. The multivariable-adjusted ORs (model 1) of hyperglycemia based on different levels of indoor activity (<5.0, 5.0–6.9, and ≥7.0 hours per day) were 1.00, 0.71 (95% CI 0.43–1.17), and 0.52 (95% CI 0.31–0.88) (Ptrend = 0.052), respectively. This association became stronger after adjustment for outdoor activity, TV watching time and sleeping time (multivariable-adjusted model 2) (Ptrend = 0.034). The multivariable-adjusted ORs (model 1) of hyperglycemia associated with different levels of sleeping time (<11.0, 11.0–11.9, and ≥12.0 hours per day) were 1.00, 0.68 (95% CI 0.43–1.06), and 0.42 (95% CI 0.25–0.71) (Ptrend = 0.005). This inverse association was still significant after additional adjustment for indoor activity, outdoor activity, and TV watching time (multivariable-adjusted model 2) (Ptrend = 0.003). However, there were no associations of outdoor activity and TV watching time with the risk of hyperglycemia.
When each type of physical activity was examined as a continuous variable, multivariate-adjusted ORs (model 2) of obesity and central obesity associated with each 1 hour/day increase in TV watching time were 1.37 (95% CI, 1.16–1.63), and 1.24 (95% CI, 1.04–1.47) (Tables 2 and 3), respectively. Multivariate-adjusted ORs (model 2) of hyperglycemia were 0.90 (95% CI, 0.82–1.00) for each 1 hour/day increase in indoor activity, and 0.78 (95% CI, 0.66–0.91) for each 1 hour/day increase in sleeping time (Table 4).
Discussion
The present study indicated a positive association of TV watching time with the risk of obesity and central obesity, and an inverse association of either indoor activity or sleeping time with the risk of hyperglycemia among offspring born to GDM mothers in Tianjin.
To our knowledge, this is the first study assessing the association of indoor activity, outdoor activity, TV watching time, and sleeping time with the risks of obesity, central obesity and hyperglycemia among preschool offspring of mothers with gestational diabetes mellitus. Several studies have shown that diet, physical activity, and behavioral modifications are effective in reducing childhood obesity20,21, however, obesity is difficult to reverse in older children and adults14. Thus developing effective prevention and intervention programs for the children at formative pre-school years (2–6 years old) might be an important step in combating the childhood obesity epidemic.
Several studies have assessed the association between TV watching time and obesity risk among school-aged children22. A cross-sectional study conducted by Dennison, B. A. et al. found that TV viewing time and TV in the child’s bedroom were associated with overweight risk in preschool children23. Another cross-sectional study from 34 countries found that television viewing times were higher in overweight compared to normal weight youth at 10–16 years old24. The International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE) found a positive association between TV watching time and the risk of obesity among 6026 children at 9–11 years of age in 12 countries8. It has been suggested that TV watching as an aspect of sedentary behavior appears to be more strongly related to obesity than other sedentary behaviors25, because TV watching has a low metabolic rate and may replace other physical activities with higher energy demands. In addition, children usually eat something or take snacks with increased caloric intake when they watch TV. Very few studies have examined the association between TV watching and childhood obesity among children under 3–5 years old in China. Thus it was unclear how early in life TV viewing in children began to express the risk of childhood obesity. Childhood obesity experts suggest to discourage television viewing in children under two years of age but 14% of children aged 6 to 23 months watch 2 or more hours/day of media26 and TV viewing is common in this age group. In the present study, we found that 52% of children under 2 years old watched television, and 82% of children at 4 years old watched TV. Children who watched ≥1.0 hour TV per day had 129% and 78% high risk of obesity and central obesity compared with those who did not watch TV.
Some studies have assessed the association between physical activity and the risk of childhood obesity, and the results are controversial. Several studies provided supportive information of an inverse association8; however, others have reported no association27,28. In the present study, we found an inverse association of indoor activity and the risk of hyperglycemia, and no association of indoor activity and outdoor activity with the risk of childhood obesity and central obesity. There are several reasons for the difference in associations across studies. First, the information of physical activity was obtained based on parents’ reports, especially for young children, which might produce recall-bias. Second, the intensity of physical activity was not generally assessed by questionnaire which is known to be important especially for young children who may alternatively take part in the types of less vigorous-intensity activities.
A 12-country study has found a significant association between short sleep duration and obesity risk in children at 9–11 years of age8. One recent review and one meta-analysis have also shown a clear association between short sleep duration and an increased risk of childhood obesity, however, very few studies in this meta-analysis included children less than 5 years of age29,30. The present study found an inverse association between sleeping time and the risk of hyperglycemia, which supported the previous finding31. However, the present study did not find any associations between sleeping time and the risks of childhood obesity and central obesity. The reason may be that the sleep duration definition is conservative and the sleeping time is different between younger and older children. Thus large studies including children less than and more than 5 years old are needed.
One recent study based on the US population found that waist circumference and BMI could equally estimate total fat and visceral fat in children32. It has been hypothesized that Asian adults have a higher percentage of body fat at a given BMI value compared with European populations33. The present study did not find any different associations between obesity risk and central obesity risk with different types of physical activity.
This study has several strengths and limitations that warrant discussions. First, we extended to study the association of different types of physical activity and the risks of obesity, central obesity and hyperglycemia among children under 5 years old. Second, children’s weight, height, waist circumference and fasting glucose were measured by trained health workers rather than by parental report. There are several limitations in this study. First, using a parent-reported questionnaire to assess children’s indoor activity, outdoor activity, TV watching time, and sleeping time is crude and imprecise because the physical activity in preschool-aged children consists of short intermittent peaks of activity with frequent rest periods, which is different from the physical activity in adults characterized by constant or systematic periods. Although the performance of this questionnaire has been used in a longitudinal study in the same area of Tianjin34,35,36, studies of accurately measuring children’s physical activity such as using 24-hour accelerometers are needed. Another limitation of this study is that only part of children aged more than 24 months were asked diet habits by a parent self-administered food frequency questionnaire (FFQ). Thus we cannot control for dietary intake on the association of physical activity, TV watching time, and sleeping time with the risks of childhood obesity and hyperglycemia. We cannot completely exclude the effects of residual confounding resulting from measurement error in the assessment of confounding factors or some unmeasured factors. As our study was conducted among the offspring of GDM, we could not compare the influence of physical activity, sedentary behavior, sleeping time with the risk of childhood obesity between children from non-GDM mothers and those from GDM mothers. Several studies have shown that offspring of mothers exposed to GDM were at increased risk of neonatal adiposity and childhood obesity, however, the interaction of physical activity, sedentary behavior, sleeping time and maternal GDM with the risk of childhood obesity is not clear, thus further studies are needed to answer this question.
In summary, this study demonstrated that more time spending on TV watching appears to be associated with a higher risk of obesity and central obesity among 1–5 years old offspring of GDM mothers. The effect of short sleep duration on hyperglycemia risk in these children appears to be independent of other risk factors.
Methods
Tianjin Gestational Diabetes Mellitus Prevention Program
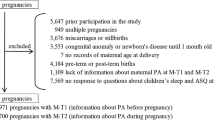
Tianjin is the fourth largest city in Northern China. All pregnant women who live in six urban districts have participated in the universal screening for GDM since 199937 by using the World Health Organization (WHO)’s GDM criteria38. From December 1998 to December 2009, a total of 128,125 pregnant women took part in the GDM screening program and 6,247 were diagnosed with GDM19. The average proportion of screened pregnancies was over 91% during 1999–200937.
Study samples
The sampling methods have been described previously in detail19. A total of 4,644 pregnant women who were diagnosed with GDM from 2005 to 2009 and their children in six urban districts were invited to participate in a baseline survey for the TGDMPP. Finally, 1263 GDM women and their children had completed the baseline survey for the TGDMPP from August 2009 to July 2011 (participation rate 27%)19,39,40,41,42,43. The study followed the guidelines of the Helsinki Declaration, and was approved by the Human Subjects Committee of the Tianjin Women’s and Children’s Health Center, informed consent was obtained for each participant.
Examinations
At baseline survey, all GDM mothers and their children completed a self-administered questionnaire and underwent a physical examination that included anthropometric and blood pressure measurements, immediate blood glucose, a 2-hour glucose 75 g OGTT (mothers only), and a fasting blood draw at the Tianjin Women’s and Children’s Health Center. Health workers from the Tianjin Women’s and Children’s Health Center collected and checked the completed questionnaire and also finished measurements. All health workers were intensively trained in meetings and in practical sessions. The questionnaire included questions on the mother’s socio-demographics (age, marital status, education, income, and occupation), history of GDM (values of fasting and 2-hour glucose in the OGTT at 26–30 gestational weeks from the Tianjin Women’s and Children’s Health Center GDM diagnosis and treatment register system), family history of chronic diseases, medical history (hypertension, diabetes, and hypercholesterolemia), and pregnancy outcomes (pre-pregnancy weight, weight gain during pregnancy, and number of children)42. We also asked the GDM children’s parents in advance to bring the child’s birth certificate and to fill in a self-administered questionnaire about the child’s birth date, sex, gestational weeks of birth, birth weight, birth recumbent length, Apgar score (above questions related to birth were copied from birth certificate), the mode and duration of infant feeding (exclusive breast feeding, mixed breast and formula feeding, and exclusive formula feeding), health characteristics (history of illness status and current health status), dietary habits (usual habits of eating breakfast, lunch, and dinner, usual frequency of intake of vegetables, fruits, sugar-sweetened beverages, and fast food), physical activity habits (duration of indoor activity, outdoor activity), usual sleeping time, and TV or computer watching time.
To determine indoor activity time, we asked the question “How many hours per day did your child play indoors during the past year ? ” and grouped it into 3 categories: <5.0, 5–6.9, and ≥7.0 hours per day. We asked the question “How many hours per day did your child play outdoors during the past year in each season separately ? ” and calculated daily mean time (sum of different seasons/4) and classified it into three categories: <1.5, 1.5–1.9, and ≥2.0 hours per day. TV watching time was assessed using the question “How many hours per day did your child watch TV during the past year ? ” and the response categories were 0, <1.0, and ≥1.0 hour per day. We also asked the question “How many hours per day did your child sleep during the past year ? ” and grouped it into 3 categories: <11.0, 11.0–11.9, and ≥12.0 hours per day. We have done classification for the indoor/outdoor activity time, TV watching time, and sleeping time based on the distributions and mean values of each activity, and then used tertiles or quartiles to assess different activities. We also investigated the association of indoor activity, outdoor activity, TV watching time, and sleeping time as continuous variables with the risks of childhood obesity, central obesity and hyperglycemia.
Children’s body weight was measured with a beam balance scale with participants wearing light indoor clothing without shoes, and height was measured by a stadiometer. Waist circumference was measured midway between the 10th rib and the top of the iliac crest. Weight was measured to the nearest 0.1 kg, height and waist circumference to the nearest 0.1 cm. Body mass index (BMI) was calculated by dividing weight in kilograms by the square of height in meters. BMI for age Z score was calculated, and we took a more recent expert committee recommendation44 that obesity was defined as a BMI more than the 95th percentiles (≥1.645 Z score) for age and gender specific distribution using WHO growth ref.45. Central obesity was defined as more than the 90th percentiles for age and gender specific distribution of waist circumference47. About 150 μl of at least 6-hour fasting capillary whole blood specimen was collected and the fasting time was recorded. Blood glucose level was immediately measured on an automatic analyzer (Biosen C-line; EKF Diagnostic GmbH, London, U.K.)48. Hyperglycemia was defined as more than the 90th percentiles of fasting glucose.
Statistical analyses
The general characteristics of both mothers and children according to different childhood obesity, central obesity and hyperglycemia status were compared using independent-samples T-Test for continuous variables and chi-square tests for categorical variables. Logistic regression was used to estimate the odd ratios (ORs) and 95% confidence intervals (CIs) of childhood obesity, central obesity and hyperglycemia associated with different levels of indoor activity, outdoor activity, TV watching time, and sleeping time. We set up two models: Model 1, adjusted for variables included maternal age, weight gain during pregnancy, education, occupation, family income, and child age, sex, gestational age, and mode of infant feeding; Model 2, adjusted for variables in Model 1 and, additionally, for TV watching time, and sleeping time (in physical activity analysis), indoor activity, outdoor activity and sleeping time (in TV watching time analysis), indoor activity, outdoor activity and TV watching time (in sleeping time analysis). All statistical analyses were performed with PASW for Windows, version 23.0 (Statistics 23, SPSS, IBM, USA).
Additional Information
How to cite this article: Zhang, T. et al. Physical Activity, TV Watching Time, Sleeping, and Risk of Obesity and Hyperglycemia in the Offspring of Mothers with Gestational Diabetes Mellitus. Sci. Rep. 7, 41115; doi: 10.1038/srep41115 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Yang, L. & Colditz, G. A. Prevalence of Overweight and Obesity in the United States, 2007–2012. JAMA internal medicine 175, 1412–1413, doi: 10.1001/jamainternmed.2015.2405 (2015).
Reynolds, K. et al. Prevalence and risk factors of overweight and obesity in China. Obesity (Silver Spring) 15, 10–18, doi: 10.1038/oby.2007.527 (2007).
Trost, S. G., Sirard, J. R., Dowda, M., Pfeiffer, K. A. & Pate, R. R. Physical activity in overweight and nonoverweight preschool children. International journal of obesity and related metabolic disorders : journal of the International Association for the Study of Obesity 27, 834–839, doi: 10.1038/sj.ijo.0802311 (2003).
Serdula, M. K. et al. Do Obese Children Become Obese Adults?A Review of the Literature. Preventive medicine 22, 167–177, 10.1006/pmed.1993.1014 (1993).
Whitaker, R. C., Wright, J. A., Pepe, M. S., Seidel, K. D. & Dietz, W. H. Predicting obesity in young adulthood from childhood and parental obesity. New England Journal of Medicine 337, 869–873 (1997).
Must, A. & Strauss, R. S. Risks and consequences of childhood and adolescent obesity. International journal of obesity and related metabolic disorders: journal of the International Association for the Study of Obesity 23, S2–11 (1999).
Ji, C. Y. Cooperative Study on Childhood Obesity: Working Group on Obesity in, C. The prevalence of childhood overweight/obesity and the epidemic changes in 1985–2000 for Chinese school-age children and adolescents. Obesity Reviews 9, 78–81, doi: 10.1111/j.1467-789X.2007.00443.x (2008).
Katzmarzyk, P. T. et al. Relationship between lifestyle behaviors and obesity in children ages 9–11: Results from a 12-country study. Obesity (Silver Spring) 23, 1696–1702, doi: 10.1002/oby.21152 (2015).
Katzmarzyk, P. T. et al. Physical Activity, Sedentary Time, and Obesity in an International Sample of Children. Medicine and science in sports and exercise 47, 2062–2069, doi: 10.1249/MSS.0000000000000649 (2015).
Hill, J. O. & Melanson, E. L. Overview of the determinants of overweight and obesity: current evidence and research issues. Medicine and science in sports and exercise 31, S515–521 (1999).
Brown, C. L., Halvorson, E. E., Cohen, G. M., Lazorick, S. & Skelton, J. A. Addressing Childhood Obesity: Opportunities for Prevention. Pediatric clinics of North America 62, 1241–1261, doi: 10.1016/j.pcl.2015.05.013 (2015).
Roberts, R. E. & Duong, H. T. Is There an Association Between Adolescent Sleep Restriction and Obesity. Journal of psychosomatic research 79, 651–656, doi: 10.1016/j.jpsychores.2015.05.012 (2015).
Sijtsma, A., Sauer, P. J., Stolk, R. P. & Corpeleijn, E. Is directly measured physical activity related to adiposity in preschool children? International Journal of Pediatric Obesity 6, 389–400 (2011).
Skouteris, H. et al. Preventing excessive gestational weight gain: a systematic review of interventions. Obesity reviews : an official journal of the International Association for the Study of Obesity 11, 757–768, doi: 10.1111/j.1467-789X.2010.00806.x (2010).
Dabelea, D. The predisposition to obesity and diabetes in offspring of diabetic mothers. Diabetes care 30 Suppl 2, S169–174, doi: 30/Supplement_2/S169 10.2337/dc07-s211 (2007).
Hillier, T. A. et al. Childhood obesity and metabolic imprinting: the ongoing effects of maternal hyperglycemia. Diabetes care 30, 2287–2292, doi: dc06-2361 10.2337/dc06-2361 (2007).
Dong, L. et al. Relationship between maternal fasting glucose levels at 4-12 gestational weeks and offspring growth and development in early infancy. Diabetes research and clinical practice 102, 210–217, doi: 10.1016/j.diabres.2013.10.017 (2013).
Liu, G. et al. Maternal OGTT glucose levels at 26-30 gestational weeks with offspring growth and development in early infancy. BioMed research international 2014, 516980, doi: 10.1155/2014/516980 (2014).
Hu, G. et al. Tianjin Gestational Diabetes Mellitus Prevention Program: Study design, methods, and 1-year interim report on the feasibility of lifestyle intervention program. Diabetes research and clinical practice 98, 508–517, doi: 10.1016/j.diabres.2012.09.015S0168-8227(12)00319-1 (2012).
Barlow, S. E. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics 120 Suppl 4, S164–192, doi: 120/Supplement_4/S16410.1542/peds.2007-2329C (2007).
O’Brien, M. et al. The ecology of childhood overweight: a 12-year longitudinal analysis. International journal of obesity 31, 1469–1478 (2007).
Rey-Lopez, J. P., Vicente-Rodríguez, G., Biosca, M. & Moreno, L. A. Sedentary behaviour and obesity development in children and adolescents. Nutrition, Metabolism and Cardiovascular Diseases 18, 242–251 (2008).
Dennison, B. A., Erb, T. A. & Jenkins, P. L. Television viewing and television in bedroom associated with overweight risk among low-income preschool children. Pediatrics 109, 1028–1035 (2002).
Janssen, I. et al. Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obesity reviews: an official journal of the International Association for the Study of Obesity 6, 123–132, doi: 10.1111/j.1467-789X.2005.00176.x (2005).
Tremblay, M. S. et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. The international journal of behavioral nutrition and physical activity 8, 98 (2011).
Rideout, V. & Hamel, E. The media family: Electronic media in the lives of infants, toddlers, preschoolers and their parents. (Henry J. Kaiser Family Foundation, 2006).
Grund, A. et al. Relationships between physical activity, physical fitness, muscle strength and nutritional state in 5-to 11-year-old children. European journal of applied physiology 82, 425–438 (2000).
Labree, W. et al. Differences in Overweight and Obesity among Children from Migrant and Native Origin: The Role of Physical Activity, Dietary Intake, and Sleep Duration. PloS one 10, e0123672, doi: 10.1371/journal.pone.0123672 (2015).
Chen, X., Beydoun, M. A. & Wang, Y. Is sleep duration associated with childhood obesity?A systematic review and meta‐analysis. Obesity 16, 265–274 (2008).
Ruan, H., Xun, P., Cai, W., He, K. & Tang, Q. Habitual sleep duration and risk of childhood obesity: systematic review and dose-response meta-analysis of prospective cohort studies. Scientific reports 5 (2015).
Koren, D. et al. Sleep architecture and glucose and insulin homeostasis in obese adolescents. Diabetes care 34, 2442–2447, doi: 10.2337/dc11-1093 (2011).
Katzmarzyk, P. T. & Bouchard, C. Where is the beef? Waist circumference is more highly correlated with BMI and total body fat than with abdominal visceral fat in children. International journal of obesity 38, 753–754 (2014).
Shiwaku, K., Anuurad, E., Enkhmaa, B., Kitajima, K. & Yamane, Y. Appropriate BMI for Asian populations. The Lancet 363, 1077 (2004).
Tian, Z. et al. Sleep duration and hyperglycemia among obese and nonobese children aged 3 to 6 years. Archives of pediatrics & adolescent medicine 164, 46–52, doi: 164/1/46 10.1001/archpediatrics.2009.233 (2010).
Bowers, K. et al. Birth weight, postnatal weight change, and risk for high blood pressure among chinese children. Pediatrics 127, e1272–1279, doi: peds.2010-2213 10.1542/peds. 2010–2213 (2011).
Zhang, X. et al. High birth weight and overweight or obesity among Chinese children 3-6 years old. Preventive medicine 49, 172–178, doi: S0091-7435(09)00347-8 10.1016/j.ypmed.2009.07.013 (2009).
Zhang, F. et al. Increasing prevalence of gestational diabetes mellitus in Chinese women from 1999 to 2008. Diabetic medicine : a journal of the British Diabetic Association 28, 652–657, doi: 10.1111/j.1464-5491.2010.03205.x (2011).
WHO Consultation. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus., (World Health Organisation, 1999).
Liu, H. et al. Prepregnancy body mass index and weight change on postpartum diabetes risk among gestational diabetes women. Obesity (Silver Spring) 22, 1560–1567, doi: 10.1002/oby.20722 (2014).
Wang, L. et al. Obesity index and the risk of diabetes among Chinese women with prior gestational diabetes. Diabetic medicine : a journal of the British Diabetic Association 31, 1368–1377, doi: 10.1111/dme.12532 (2014).
Li, W. et al. Different associations of diabetes with beta-cell dysfunction and insulin resistance among obese and nonobese Chinese women with prior gestational diabetes mellitus. Diabetes care 37, 2533–2539, doi: 10.2337/dc14-0573 (2014).
Zhang, S. et al. Maternal Glucose during Pregnancy and after Delivery in Women with Gestational Diabetes Mellitus on Overweight Status of Their Children. BioMed research international 2015, 9, doi: 10.1155/2015/543038 (2015).
Leng, J. et al. GDM Women’s Pre-Pregnancy Overweight/Obesity and Gestational Weight Gain on Offspring Overweight Status. PloS one 10, e0129536 (2015).
Krebs, N. F. et al. Assessment of child and adolescent overweight and obesity. Pediatrics 120 Suppl 4, S193–228, doi: 10.1542/peds.2007-2329D (2007).
World Health Organization The WHO Child Growth Standards., http://www.who.int/childgrowth/standards/en/.(2006).
Schwandt, P., Kelishadi, R. & Haas, G. M. First reference curves of waist circumference for German children in comparison to international values: the PEP Family Heart Study. World journal of pediatrics : WJP 4, 259–266, doi: 10.1007/s12519-008-0048-0 (2008).
Lee, J. M., Davis, M. M., Woolford, S. J. & Gurney, J. G. Waist circumference percentile thresholds for identifying adolescents with insulin resistance in clinical practice. Pediatric diabetes 10, 336–342, doi: 10.1111/j.1399-5448.2008.00474.x (2009).
Campbell, M. D. et al. A low-glycemic index meal and bedtime snack prevents postprandial hyperglycemia and associated rises in inflammatory markers, providing protection from early but not late nocturnal hypoglycemia following evening exercise in type 1 diabetes. Diabetes care 37, 1845–1853, doi: 10.2337/dc14-0186 (2014).
Acknowledgements
This study was supported by Tianjin Women’s and Children’s Health Center, Tianjin Public Health Bureau, European Foundation for the Study of Diabetes (EFSD)/Chinese Diabetes Society (CDS)/Lilly programme for Collaborative Research between China and Europe, and the National Institute Of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health under Award Number R01DK100790. We wish to thank the TGDMPP families who are participating in the study and their families, and the TGDMPP Research Group.
Author information
Authors and Affiliations
Contributions
Study concept and design: G.H., P.W., L.Q., J.T., X.Y., and Z.Y. Acquisition of data: H.L., L.W., W.L., J.L., N.L., and S.Z. Analysis and interpretation of data: T.Z. and G.H. All authors were involved in writing the paper and had final approval of the submitted and published versions.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Zhang, T., Wang, P., Liu, H. et al. Physical Activity, TV Watching Time, Sleeping, and Risk of Obesity and Hyperglycemia in the Offspring of Mothers with Gestational Diabetes Mellitus. Sci Rep 7, 41115 (2017). https://doi.org/10.1038/srep41115
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep41115
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
