
Abstract
The impact of anemia on the outcome of patients with stroke remains inconsistent. We performed a meta-analysis of cohort studies to assess the mortality risk in stroke patients with and without anemia. Systematic searches were conducted in the PubMed, China National Knowledge Infrastructure, Web of Science and Wanfang databases to identify relevant studies from inception to November 2015. The estimated odds ratio with a 95% confidence interval was pooled. subgroup analyses and sensitivity analyses were also conducted. We used Begg’s funnel plot and Egger’s test to detect the potential publication bias. Thirteen cohort studies with a total of 19239 patients with stroke were included in this meta-analysis. The heterogeneity among studies was slight (I2 = 59.0%, P = 0.031). The results from a random-effect model suggest that anemia is associated with an increased mortality risk in patients with stroke (adjusted odds ratio = 1.39, 95% confidence interval: 1.22–1.58, P < 0.001). The subgroup analyses are consistent with the total results. This meta-analysis of 13 cohort studies finds that anemia increases the mortality risk in patients with stroke. Future studies should perform longer follow-up to confirm this finding and explore its possible mechanism.
Similar content being viewed by others

Introduction
Anemia is a common condition for the older population and its prevalence increases with age. Previous studies have found that anemia is associated with mortality, poor physical performance and disability1,2,3. Additionally, anemia is an independent predictor of in-hospital mortality both in patients with acute myocardial infarction and in patients with congestive heart failure4,5. The cerebral oxygen supply depends on the cerebral blood flow and arterial oxygen content and the hemoglobin level determines the arterial oxygen content6. Anemia may cause a reduction in the oxygen-carrying ability, alterations in blood viscosity and impaired cerebral regulation7. It is reasonable that low hemoglobin or anemia has disadvantageous influences on the brain. Unfortunately, such a situation is adverse for patients with stroke and the current treatment guidelines do not recommend an appropriate cutoff of hemoglobin level for stroke8.
Stroke has many well-known risk factors, such as diabetes mellitus, smoking, aging, dyslipidemia and hypertension9,10. Recent studies have suggested that anemia is a risk factor for ischemic stroke and is related to high mortality in the hospital. However, the impact of anemia on the mortality risk of stroke remains unclear and several epidemiological studies show inconsistent results11,12,13. To our knowledge, the consistency and quality of evidence on this topic have not been well reviewed, which limits our comprehensive understanding of the impact of anemia on the outcomes and prognosis of stroke. Based on the current findings and accumulating evidence, we conducted a meta-analysis of published cohort studies to assess the mortality risk in patients with stroke.
Results
Study flow and characteristics
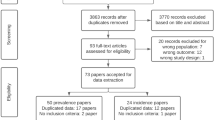
Our initial search returned 813 records and three additional records were identified through retrieving references lists. Of these, 503 records were left for further screening after the duplicates were removed. A total of 347 records were excluded for a variety of reasons, such as being a review, commentary, case reports, duplicates, letter, or irrelevant studies. A total of 156 records were ready for the third stage and 143 records were excluded after further screening. Finally, 13 were cohort studies entered into our meta-analysis12,13,14,15,16,17,18,19,20,21,22,23,24. The specific process of study selection is presented in Fig. 1.

The process of study selection.
Table 1 shows the general characteristics of the 13 cohort studies with a total of 10009 participants included in the meta-analysis. The included studies were published from 2007 to 2015. Seven studies were from China12,15,16,18,19,20,23 and the remaining six ones were from the USA22, Denmark13, Greece14, India17 Israel21 and Canada24. Two studies had a retrospective study design and 10 had a prospective cohort study design. The sample sizes ranged from 66 to 923014,24. The maximum duration of follow-up was three years12 and the minimum was 48 hours17. The prevalence of anemia ranged from 0.11% to 39.4%. Seven studies were conducted in a population with acute stroke and 6 were conducted in patients with non-acute stroke. Six studies provided the information from initial symptoms to admission (within 7 days), the rest are lack of this information. Of these,13 studies treated death as the measure index and two studies also include disability. Ten studies adopted the WHO criteria (male:<130 g/L, female:<120 g/L), 2 studies used self-defined criteria (male:<140 g/L, female:<120 g/L and male and female:<100 g/L) and 1 study adopted the China criteria (male<120 g/L and female:<110 g/L). The mean NOS score of study quality was 7.1. The additional file 1 shows the quality assessment of the study according to the NOS criteria.
Anemia and the mortality risk of stroke
Figure 2 shows the pooled prevalence of anemia in patients with stroke. The results from 13 studies show that the prevalence was 21.9% (95%CI: 13.6–30.3%). Figure 3 shows the estimated OR of anemia for stroke. The univariate results include six studies and the adjusted results have 13 studies. A total of 19,239 patients are included in the meta-analysis. The heterogeneity within the study is low (I2 = 0% to 59%). The random-effects model was conducted for the pooled OR. Both the univariate and adjusted analyses found that anemia is associated with an increased mortality risk in patients with stroke (for univariate: OR = 2.33, 95%CI: 2.00–2.72; for adjusted: OR = 1.39, 95%CI: 1.22–1.58). Table 2 also shows the subgroup results from the region and type of disease. The results of the subgroup analyses are consistent with the adjusted pooled results and the anemia remains related to mortality of stroke (Table 2).

Prevalence of anemia in patients with stroke.

Forest plot showing the mortality risk of anemia in patients with stroke.
Sensitivity analysis
We first assessed the influence of each study on the increased mortality risk by omitting one study each time. The results found no extensive change for the pooled estimation. To further examine the stability of the results, we also conducted extra analyses for the following four types: Type I: excluding 2 retrospective studies (OR = 1.36, 95%CI: 1.20–1.55); Type II: excluding 1 study with small sample size (OR = 1.58, 95%CI: 1.37–1.82); Type III: excluding 2 studies with low prevalence of anemia (OR = 1.50, 95%CI: 1.33–1.70); Type IV: excluding 3 studies with less than 3 months of follow-up (OR = 1.64, 95%CI: 1.41–1.91); Type V: excluding 3 studies with self-defined criteria of anemia (OR = 1.57, 95%CI: 1.38–1.78). The analyses suggested that our results are sufficiently robust to identify the increased mortality risk of anemia for patients with stroke.
Publication bias
The Begg’s and Egger’s test indicated that a slight publication bias exists (P < 0.05). Asymmetry is also found in the medium part of the funnel plot, in which approximately two negative studies are missing (Fig. 4). This asymmetry may potentially overestimate the risk of anemia for patients with stroke. Seven of the included studies are from China, which this may be the reason for this finding.

Funnel plot for the mortality risk of anemia in patients with stroke.
Discussion
The present meta-analysis of 13 cohort studies shows that anemia is an independent risk factor of unfavourable outcomes in patients with stroke. The stroke patients with anemia had a 39% increase in mortality risk compared with those without anemia. In addition, this relationship was found in some subgroup analyses. Our findings suggest that early intervention for patients with stroke and anemia could be important to decrease the risk of adverse clinical outcomes.
Previous studies have confirmed the relationship between anemia and short-term adverse outcomes in other patients settings such as chronic heart failure25, type 2 diabetes patients with chronic kidney disease26 and myocardial infarction27. The present study provides further support for the relationship between anemia and vascular condition. The prevalence of anemia in acute patients range from 17% to 29%11,12. We also estimated the prevalence of anemia of stroke patients in this meta-analysis. Our results found that the pooled prevalence of anemia in patients with stroke was 21.9% (95%CI: 13.6–30.3), which was significantly higher than the reported prevalence in the general elderly population, in which the prevalence was 7%28. Of the 13 studies, there were inconsistent results for the association between the mortality risk of stroke and anemia. In contrast to these reports, 2 studies found that anemia was not always associated with mortality in patents with stroke. Sico et al. conducted a 1-year follow-up in less severe ischemic stroke patients with a sample size of 1306. They found that anemia might be independently associated with outcome in patients with less severe stroke (adjusted OR = 4.17; 95% CI: 1.47–11.90), but not in patients with more severe strokes (adjusted OR, 0.82; 95%CI: 0.30–2.22). In parallel with these findings, Hao et al. found that anemia was not a risk factor of death and disability outcome (adjusted OR = 1.01, 95%CI: 0.71–1.44) in patient with acute ischemic stroke16. The reason for this result could be that the severity of stroke contributed to the mortality risk more than the other existing complications such as the presence of anemia17. Interestingly, Sico et al. also suggested a J-shaped relationship between the hematocrit level and a poor prognosis in severe stroke patients. This only explains why patients with more severe stroke tend to have adverse outcomes but did not confirm the relationship and risk in patients with less severe stroke. The remaining studies reported an increase risk of mortality in patients with anemia.
The oxygen supply of the brain is closely related to the hemoglobin level and blood viscosity. There could be three stages during the process of the adverse impact on the outcomes in patients with stroke. First, early-stage injury may occur to cerebral regulation when hemoglobin is at a low level. During this period, the cerebral vascular system can continue to regulate itself for normal function. A lower hemoglobin level is associated with a higher relative cerebral blood flow within the middle/inferior frontal regions, whereas higher hemoglobin level is associated with lower parenchymal cerebral blood flow and a decrease in parenchymal cerebral blood flow over time29,30. When anemia occurs in patients with stroke, the lack of oxygen and energy supply will have a great significant influence on the cerebral vascular regulation over time. In addition to other medical complications, anemia dominates for the accumulation damage course of cerebral autoregulation. With the progress of the disease, patients with anemia will suffer from many complications, such as heart failure31, chronic kidney disease32 and vascular endothelial cells33,34, which play a more important role than anemia in the development of stroke. This effect may partly explain why Sico and colleagues found a positive relationship in patients with less severe stroke but not in severe stroke17. In addition, anemia may be suggested to be related to the inflammation response and some inflammatory markers are increased in patients with anemia, such as C-reactive protein, tumour necrosis factor-α (TNF-α) and some interleukins (ILs)35. These inflammatory markers could affect the prognosis after stroke. TNF-α is involved in the process of ischemic injury and increased IL-6 has been found in the adverse prognosis after stroke. Moreover, C-reactive protein may be suggested to be related to increased mortality risk after stoke36,37,38 and anemia may affect outcomes after stroke through its relationship with inflammation.
The strengths of our meta-analysis are that only cohort studies with high quality were included and the adjusted results were reported. In addition, we conducted study selection, data extraction and analyses, which strictly complied with the MOOSE (Meta-analysis of Observational Studies in Epidemiology Statement) guidelines. These could reduce the possibility of recall bias, which is particularly important for observational studies.
Study limitations
There are several limitations for our meta-analysis. First, subgroup analyses are not the same as the adjusted pooled results with controlling for major potential confounding factors. We cannot conduct combined analysis because of the lack of data in subgroup analyses. There may be some confounders affecting the results, such as hemoglobin measurement, which occurs by capillary, venous, POCT equipment. Despite the report of a positive relationship between anemia and mortality risk of stroke, a study by Tnne et al. included some patients with intracerebral hemorrhage and a high loss of follow-up21. Second, patients with anemia could have more poor health problems, which could result in increasing the risk of mortality. Third, the maximum follow-up time was 3 years and therefore assessment of long-term effects of anemia post stroke is lacking. Some studies have suggested a significant association between anemia and adverse outcomes in patents with stroke, although the relationship is weak. The cut-off values of 95%CI are approximately equal to one. Anemia is more likely a bystander effect. A study with a longer follow-up time is needed. Finally, the funnel plot indicated the presence of publication bias, which may overestimate the risk effect of anemia because some negative results are missing.
In conclusion, this meta-analysis of 13 cohort studies finds that anemia increases the mortality risk in patients with stroke. Future studies should conduct longer follow-up to confirm and explore the possible mechanism for this finding.
Methods and Materials
The ethical approval is not necessary for the present study because this is a meta-analysis of the published studies. We conducted the meta-analysis and systematic review in accordance with the guidelines of MOOSE39.
Literature Search Strategy
We conducted systematic searches in the PubMed, China National Knowledge Infrastructure (CNKI), Web of science and Wanfang databases to identify relevant studies without language restrictions from inception to November 2015. The search terms included ‘anemia’, ‘anaemia’, ‘hypohemia’, ‘stroke’, ‘acute ischemic stroke’, ‘ischemic stroke’, ‘hemorrhagic stroke’, ‘AHS’ and ‘apoplexy’. We also retrieved the reference lists from recent reviews to obtain other potentially eligible studies that were not identified in our initial search.
Criteria for Inclusion
A study must have met the following criteria: (1) type of study: a prospective or retrospective study; (2) study population: patients diagnosed with stroke, including acute or non-acute ischemic stroke, hemorrhagic stroke; (3) comparison of factor: with and without anemia; (4) outcome: the primary outcome is death or with disability; (5) Definition: studies give specific WHO or other definition of anemia. (6) information: studies at least provide the risk estimation of anemia in a multivariate analysis. In addition, we only included those studies that contained the most recent and complete information if duplicated data were found in several studies.
Data Extraction and Quality Assessment
We used a standardized data collection sheet to extract the following information: first author, year of publication, region, study design, age of the study population, duration of follow-up, sample size, prevalence of anemia, number of female and male, adjusted factors in the multiple factor analysis, outcome measurement, the univariate estimated odds ratio (ORs) with 95% confidence intervals (95%CIs) and the adjusted ORs with 95%CIs. We also contacted the corresponding author of articles to obtain more information.
We used NOS (Newcastle-Ottawa Scales) items to assess the quality of included studies40. The NOS includes selection, comparability and outcome. The selection item includes four sub-item: exposed cohort, nonexposed cohort, ascertainment of exposure and outcome of interest. The outcome includes assessment, length of follow-up and adequacy of follow-up. We evaluated the quality of included studies as the following rules: priority (7–8 adequate items), high quality (equal or more than 5 items), low quality (less than 5 items) and extreme low quality (no description of study methods).
Two investigators independently performed the selection of included studies, data collection and quality assessment. A third investigator solved any disagreements.
Statistical Analysis
Nearly all studies used OR as a risk estimation between anemia and different types of stroke. Therefore, we pooled the OR of the included studies in this meta-analysis. We first estimated the prevalence of anemia in patients with stroke using DerSimonian-Laird in random effects model. The Cochran Q test and I2 were applied to examine the heterogeneity within studies. For the I2 statistic, low level was less than 25%, moderate was 25–50% and high level was more than 50%41,42. Random effects models are used for significant heterogeneity; otherwise fixed effects models are applied. To explore the possible inconsistency of results, we also conducted subgroup analyses in univariate and multivariate analyses, type of disease (acute vs non-acute), region (China vs others), follow-up duration (<6 months vs ≥6 months) and male/female ratio (median: ≤1.2 vs >1.2). To assess the stability of the pooled results, we conducted 5 types of sensitivity analyses: Type I, excluding 2 retrospective studies; Type II, excluding 1 study with small sample size; Type III, excluding two studies with low prevalence of anemia; Type IV, excluding 3 studies with less than 3 months of follow-up; Type V, excluding 3 studies with self-defined criteria of anemia. We also evaluated the influence of each study on the summarized estimation by omitting on study in each time. We used Begg’s funnel plot and Egger’s rank correlation test to detect the potential publication bias43,44. P < 0.05 was considered statistically significance. All statistical analyses were conducted using the Stata 12.0 software (Stata Corporation, College Station, TX, USA).
Additional Information
How to cite this article: Li, Z. et al. Anemia increases the mortality risk in patients with stroke: A meta-analysis of cohort studies. Sci. Rep. 6, 26636; doi: 10.1038/srep26636 (2016).
References
Liu, Z. Y. et al. Anemia, Physical Function and Mortality in Long-Lived Individuals Aged 95 and Older: A Population-Based Study. J Am Geriatr Soc 63, 2202–2204 (2015).
Owusu, C. et al. Anemia and Functional Disability in Older Adults with Cancer. J Natl Compr Canc Netw 13, 1233–1239 (2015).
Scott, S. P., Chen-Edinboro, L. P., Caulfield, L. E. & Murray-Kolb, L. E. The impact of anemia on child mortality: an updated review. Nutrients 6, 5915–5932 (2014).
Kosiborod, M., Smith, G. L., Radford, M. J., Foody, J. M. & Krumholz, H. M. The prognostic importance of anemia in patients with heart failure. Am J Med 114, 112–119 (2003).
Ayhan, E. et al. Patients with anemia on admission who have undergone primary angioplasty for ST elevation myocardial infarction: in-hospital and long-term clinical outcomes. Coron Artery Dis 22, 375–379 (2011).
Dhar, R. et al. Red blood cell transfusion increases cerebral oxygen delivery in anemic patients with subarachnoid hemorrhage. Stroke 40, 3039–3044 (2009).
Leal-Noval, S. R., Munoz-Gomez, M. & Murillo-Cabezas, F. Optimal hemoglobin concentration in patients with subarachnoid hemorrhage, acute ischemic stroke and traumatic brain injury. Curr Opin Crit Care 14, 156–162 (2008).
Goldstein, L. B. et al. Primary prevention of ischemic stroke: A statement for healthcare professionals from the Stroke Council of the American Heart Association. Stroke 32, 280–299 (2001).
Bang, O. Y., Ovbiagele, B. & Kim, J. S. Nontraditional Risk Factors for Ischemic Stroke: An Update. Stroke 46, 3571–3578 (2015).
Li, L. et al. Incidence, outcome, risk factors and long-term prognosis of cryptogenic transient ischaemic attack and ischaemic stroke: a population-based study. Lancet Neurol 14, 903–913 (2015).
Del, F. P. et al. Anemia and chronic kidney disease are potential risk factors for mortality in stroke patients: a historic cohort study. BMC Nephrol 11, 27 (2010).
Huang, W. Y., Chen, I. C., Meng, L., Weng, W. C. & Peng, T. I. The influence of anemia on clinical presentation and outcome of patients with first-ever atherosclerosis-related ischemic stroke. J Clin Neurosci 16, 645–649 (2009).
Nybo, M., Kristensen, S. R., Mickley, H. & Jensen, J. K. The influence of anaemia on stroke prognosis and its relation to N-terminal pro-brain natriuretic peptide. Eur J Neurol 14, 477–82 (2007).
Milionis, H. et al. Anemia on admission predicts short- and long-term outcomes in patients with acute ischemic stroke. Int J Stroke 10, 224–230 (2015).
Li, S. J. et al. Correlation between anemia and outcome in patients with acute cerebral infarction. Chin J Neuro 48, 652–656 (2015).
Hao, Z. et al. A cohort study of patients with anemia on admission and fatality after acute ischemic stroke. J Clin Neurosci 20, 37–42 (2013).
Sico, J. J. et al. Anemia is associated with poor outcomes in patients with less severe ischemic stroke. J Stroke Cerebrovasc Dis 22, 271–278 (2013).
Lin, L. C. et al. Predictors of clinical deterioration during hospitalization following acute ischemic stroke. Eur Neurol 67, 186–192 (2012).
Zhen, Z. Q. Related factor analysis in the prognosis with spontaneous hemorrhage stroke, PhD thesis, Zhengzhou University (2012).
Xu, J. et al. Chronic kidney disease is prevalent in Chinese patients admitted with verified cerebrovascular lesions and predicts short-term prognosis. Nephrol Dial Transplant 26, 2590–2594 (2011).
Tanne, D. et al. Anemia status, hemoglobin concentration and outcome after acute stroke: a cohort study. BMC Neurol 10, 22 (2010).
Kumar, M. A. et al. Anemia and hematoma volume in acute intracerebral hemorrhage. Crit Care Med 37, 1442–1427 (2009).
Huang, W. Y. et al. Predictive factors of outcome and stroke recurrence in patients with unilateral atherosclerosis-related internal carotid artery occlusion. Neurol India 56, 173–178 (2008).
Furlan, J. C., Fang, J. & Silver, F. L. Acute ischemic stroke and abnormal blood hemoglobin concentration. Acta Neurol Scand 10.1111/ane.12521 (2015). [Epub ahead of print].
Nakagawa, Y., Yasuno, S. & Kuwahara, K. Differential Relationships Between Anemia and Outcome in Subgroups of Patients with Chronic Heart Failure. Circ J 79, 1893–1894 (2015).
Theilade, S. et al. Pulse pressure is not an independent predictor of outcome in type 2 diabetes patients with chronic kidney disease and anemia-the Trial to Reduce Cardiovascular Events with Aranesp Therapy (TREAT). J Hum Hypertens 30, 46–52 (2016).
Cavusoglu, E. et al. Usefulness of anemia in men as an independent predictor of two-year cardiovascular outcome in patients presenting with acute coronary syndrome. Am J Cardiol 98, 580–584 (2006).
Corona, L. P., Duarte, Y. A. & Lebrao, M. L. Prevalence of anemia and associated factors in older adults: evidence from the SABE Study. Rev Saude Publica 48, 723–431 (2014).
van der Veen, P. H. et al. Hemoglobin, hematocrit and changes in cerebral blood flow: The Second Manifestations of ARTerial Disease-Magnetic Resonance study. Neurobiol Aging 36, 1417–1423 (2015).
Gottesman, R. F. et al. Patterns of regional cerebral blood flow associated with low hemoglobin in the Baltimore Longitudinal Study of Aging. J Gerontol Biol Sci Med Sci 67, 963–969 (2012).
Anand, I. S. & Rector, T. S. Pathogenesis of anemia in heart failure. Circ Heart Fail 7, 699–700 (2014).
Lau, B. C., Ong, K. Y., Yap, C. W., Vathsala, A. & How, P. Predictors of anemia in a multi-ethnic chronic kidney disease population: a case-control study. Springerplus 4, 233 (2015).
Strijbos, M. H. et al. Circulating endothelial cells: a potential parameter of organ damage in sickle cell anemia? Blood Cells Mol Dis 43, 63–67 (2009).
Blum, A. et al. Endothelial function in patients with sickle cell anemia during and after sickle cell crises. J Thromb Thrombolysis 19, 83–86 (2005).
Ferrucci, L. et al. Proinflammatory state and circulating erythropoietin in persons with and without anemia. Am J Med 118, 1288 (2005).
Barone, F. C. et al. Tumor necrosis factor-alpha. A mediator of focal ischemic brain injury. Stroke 28, 1233–1244 (1997).
Di Napoli, M., Papa, F. & Bocola, V. C-reactive protein in ischemic stroke: an independent prognostic factor. Stroke 32, 917–924 (2001).
Vila, N., Castillo, J., Davalos, A. & Chamorro, A. Proinflammatory cytokines and early neurological worsening in ischemic stroke. Stroke 31, 2325–2329 (2000).
Stroup, D. F. et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 283, 2008–2012 (2000).
Wells, G. A. et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality if nonrandomized studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed in December 10, 2015.
Higgins, J. P., Thompson, S. G., Deeks, J. J. & Altman, D. G. Measuring inconsistency in meta-analyses. BMJ 327, 557–560 (2003).
DerSimonian, R. & Laird, N. Meta-analysis in clinical trials. Control Clin Trials 7, 177–88 (1986).
Egger, M., Davey, S. G., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 315, 629–634 (1997).
Begg, C. B. & Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics, 50, 1088–1101 (1994).
Acknowledgements
We thank all our colleagues working in the Department of Epidemiology and Health Statistics, School of public health of Central South University. Hunan Province Science and Technology Project (2014SK2013), fundamental research funds for the central universities of central south university (2014zzts069) and Graduate Innovation Project of Hunan Province (CX2014B097).
Author information
Authors and Affiliations
Contributions
Z.Z.L. and L.Z.C. conceived the study, Y.Y.L. participated in the design; Z.Z.L. and P.C. collected the data. Z.Z.L. and L.Z.C. drafted the manuscript. T.Z. revised the manuscript and language. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Li, Z., Zhou, T., Li, Y. et al. Anemia increases the mortality risk in patients with stroke: A meta-analysis of cohort studies. Sci Rep 6, 26636 (2016). https://doi.org/10.1038/srep26636
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep26636
This article is cited by
-
Stroke risk in rheumatoid arthritis patients: exploring connections and implications for patient care
Clinical and Experimental Medicine (2024)
-
Cerebrovascular Complications of Anemia
Current Neurology and Neuroscience Reports (2021)
-
Machine learning to predict mortality after rehabilitation among patients with severe stroke
Scientific Reports (2020)
-
Anemia and iron metabolism in COVID-19: a systematic review and meta-analysis
European Journal of Epidemiology (2020)
-
Hemoglobin concentration does not impact 3-month outcome following acute ischemic stroke
BMC Neurology (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
