
Abstract
From 2010 to 2012, large outbreaks of EV-A71-related- hand foot and mouth disease (HFMD) occurred annually in China. Some cases had neurological complications and were closely associated with fatal cardiopulmonary collapse, but not all children with central nervous system (CNS) involvement demonstrated a poor prognosis. To identify which patients and which neurological complications are more likely to progress to cardiopulmonary failure, we retrospectively studied 1,125 paediatric inpatients diagnosed with EV-A71-related HFMD in Hunan province, including 1,017 cases with CNS involvement. These patients were divided into cardiopulmonary failure (976 people) group and group without cardiopulmonary failure (149 people). A logistic regression analysis was used to compare the clinical symptoms, laboratory test results and neurological complications between these two groups. The most significant risk factors included young age, fever duration ≥3 days, coma, limb weakness, drowsiness and ANS involvement. Patients with brainstem encephalitis and more CNS-involved regions were more likely to progress to cardiopulmonary failure. These findings can help front-line clinicians rapidly and accurately determine patient prognosis, thus rationally distributing the limited medical resources and implementing interventions as early as possible.
Similar content being viewed by others


Introduction
Since the EV-A71 virus was first isolated in California, USA, in 19691, it has become a threat to global public health. EV-A71 primarily infects children and its clinical manifestations include hand, foot and mouth disease (HFMD) and herpangina. Some cases are accompanied by neurological complications, which manifest as brainstem encephalitis, aseptic meningitis, encephalitis and acute flaccid paralysis (AFP) and some of the cases can progress to cardiopulmonary failure or even death2,3.
In the past 15 years, the Asia-Pacific region has witnessed several EV-A71 epidemics4,5,6. Nationwide epidemics in China began in 2008, with a total of 488,955 cases and 126 deaths while the population is 1328,020,0007,8. From 2010 to 2012, large nationwide outbreaks of HFMD occurred annually in mainland China, Hunan province in the central-south region of China was one of the hardest-hit regions. According to the data from the Hunan Provincial Center for Disease Control (CDC), there were 189,382 HFMD cases in Hunan in 2012, including 98 deaths while the population is 66,390,0009 and the mortality was ranked third among a total of 33 provinces around the country. Although an inactivated alum-adjuvant enterovirus 71 vaccine has completed Phase III clinical trials, it remains far from widespread application10,11,12. Thus far, the annual incidence, sequelae rate and mortality remain high in China and the demand for medical resources exceeded the supply at the peak of the epidemic. According to the Hunan Provincial CDC, the incidence in May 2012 was 71.15/100000 and the Xinhua Net13 reported that approximately 500 clinical HFMD patients visited the Hunan Children’s Hospital daily. Although this hospital reserved all of the beds in wards and all emergency clinics to admit and treat paediatric patients with HFMD, it remained difficult to treat all of the pediatric patients seeking admission. Therefore, a challenge for front-line clinicians is to identify which paediatric patients are more likely to develop cardiopulmonary failure to rationally allocate limited medical resources and to intervene in cardiopulmonary failure as early as possible.
The Guide to the Clinical Management and Public Health Response for HFMD14 (hereafter referred to as the Guide) suggests that the clinical development of HFMD can be divided into four stages: simple HFMD, central nervous system (CNS) involvement, autonomic nervous system (ANS) dysfunction and eventually, cardiopulmonary failure. CNS involvement is closely associated with severe sequelae and fatal cardiopulmonary collapse, but not all children with CNS involvement will demonstrate a poor prognosis. The results of a prospective clinical study during EV-A71 outbreaks in Sarawak showed that CNS complications were predicted by three risk factors (duration of fever ≥3 days, peak temperature ≥38.5 °C and a history of lethargy), but other early findings associated with severe or fatal disease have not been confirmed15. Therefore, it is very important for clinicians to rapidly determine which regions of the nervous system are affected and which neurological complications are more likely to lead to cardiopulmonary failure; these factors may predict the prognosis and prevent the progression as early as possible. However, reliable methods of predicting which patients with CNS involvement will develop into cardiopulmonary failure are still lacking2. The existing literature6,14,16,17,18,19,20 suggests that brainstem encephalitis may be a risk factor for cardiopulmonary failure, but the number of cases studied has been small and the data have not been statistically analysed. Huang et al. classified myoclonus as the clinical manifestation of grade I brainstem encephalitis20, but most cases demonstrate only myoclonus and no other evidence of brainstem encephalitis21. Myoclonus may occur in normal young children, particularly when they are asleep2. The literature has also reported that myoclonus alone cannot be used as a diagnostic indicator of brainstem encephalitis21. Moreover, the involvement of any one of the following areas can cause myoclonus: the cerebral cortex, the brainstem, the cerebellum and the spinal cord22. Therefore, in addition to the four neurological complications described by the Guide14, we also studied the association between EV-A71-related HFMD with simple myoclonus and cardiopulmonary failure.
In the present study, we analysed the medical records of 1,125 HFMD patients who were infected with EV-A71 and hospitalized in the Hunan Children’s Hospital (a Chinese provincial hospital designated for HFMD) during the period of 2010–2012, including 1,017 cases with CNS involvement, in an attempt to identify the possible predictive indicators of cardiopulmonary failure.
Methods
Our study was granted approval from the ethics committees of Xiangya Hospital and the Hunan Children’s Hospital. In addition, we obtained informed consent from patients whose photographs were used in this manuscript. This study was conducted in accordance with the approved guidelines and regulations, in line with the tenets of the Declaration of Helsinki.
Pathogen detection
Case specimens (throat swabs, stool samples, fluid from blisters and cerebrospinal fluid) of the patients were collected by the Hunan Children’s Hospital. Viral RNA extracted from samples submitted for diagnostic assays was performed using the Viral Nucleic Acid Extraction Kit II (Geneaid Biotech Ltd., Taiwan) according to the manufacturer’s instructions23. A diagnostic kit for CV-A16 and EV-A71 RNA (Fluorescent PCR) (Bioperfectus technologies, Jiangsu, China) was used to conduct simultaneous detection of human EV-A71 and CV-A16 by multiplex real-time PCR with an internal amplification control24. If any of the case specimens was positive, we can make the diagnosis of EV-A71 or CV-A165.
HFMD patients infected with EV-A71
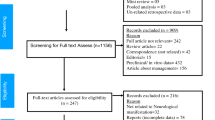
Among the clinically diagnosed HFMD patients hospitalized in the Hunan Children’s Hospital from January 2010 to December 2012, 1,392 cases were diagnosed as EV-A71-related HFMD based on EV-A71 positivity detected by PCR test. Our study focused on EV-A71 positive HFMD. To maximize the specificity of our results, patients with EV-A71/CV-A16 (coxsackievirus type A 16) co-infections were excluded. After removing 267 cases with CV-A16/EV-A71 double-infection, 1,125 medical records remained for the present retrospective study.
Case definition
The case definitions were based on the Guide14. HFMD was defined as a febrile illness with a typical rash on the mouth, palms and/or soles of the feet, which often occurs in infants and young children. HFMD patients with myoclonus alone included the presence of only myoclonus, without other neurological symptoms or signs. In our present study, there were 559 cases of myoclonus alone, which were more frequent compared with the previous normal period, indicating that the CNS was affected. However, we could not conclude which regions of the CNS were damaged because of myoclonus alone. Therefore, we thought of myoclonus alone as one type of the neurological complications. Neurological complications with or without myoclonuscan be divided into aseptic meningitis, brainstem encephalitis, encephalitis and acute flaccid paralysis (AFP). Aseptic meningitis was defined as a febrile illness with headache, vomiting and meningism associated with more than 10 white cells/mm3 cerebrospinal (CSF) fluid and negative results of CSF bacterial culture. Encephalitis was defined as impaired consciousness, including lethargy, drowsiness, coma or seizures with or without myoclonus. Brainstem encephalitis (rhombencephalitis) was defined as any combination of ataxia, nystagmus, oculomotor palsies and bulbar palsy, with or without myoclonus or an abnormal MRI. AFP was defined as the acute onset of flaccid muscle weakness and a lack of reflexes. AFP includes polio-like anterior horn cell involvement (anterior myelitis), Guillain-Barre syndrome (or peripheral nerve damage) and transverse myelitis2. To summarize all of the neurological complications, we defined mixed CNS involvement as any combination of the above four types of neurological complications. Definitions of ANS dysregulation, pulmonary oedema/haemorrhage and cardiorespiratory failure were accordant with the Guide14. Leucocytosis was defined as a white blood cell (WBC) count greater than 17,500 cells/μL on admission26, hyperglycaemia was defined as a blood glucose concentration greater than 8.3 mmol/L26 and intracranial hypertension was defined as a cerebrospinal fluid pressure greater than 180 mm H2O. The indicators for heart rate, respiration, blood pressure and lymphocyte subset abnormalities are listed in Supplementary Tables S1 and S2.
Definition of outcome
HFMD patients infected with EV-A71 were divided into cardiopulmonary failure group and group without cardiopulmonary failure. According to the Guide14, we defined cardiorespiratory failure as those with any of the following conditions: tachycardia, respiratory distress, pulmonary oedema, poor peripheral perfusion requiring inotropes, pulmonary congestion on chest radiography and reduced cardiac contractility on echocardiography. The dataset was randomly divided into two subsets: (1) the validation set (1,065 cases) and (2) the test set (60 cases). Patients were taken from the entire sample according to a conventional random number generation procedure and were then allocated to the two subsets with pre-determined sizes.
Follow-up
The children were reviewed to assess neurological sequelae by a neurological examination undertaken by a trained doctor 1 year after discharge. At review, a modified Rankin Scale27 score was obtained to quantify disability (0 is normal, 1 is mild symptoms and no disability, 2 is slight disability, 3 is moderate disability and ability to walk independently, 4 is moderate severe disability and ability to walk with assistance, 5 is severe disability and inability to walk and 6 is death).
Statistical analysis
The data were analysed using SPSS statistical software (IBM version 19.0, Chicago, Illinois, USA). The continuous variables were analysed using Student’s t test and the categorical variables were analysed using the χ2 test. When the expected values were less than 5, we used Fisher’s exact test for correction. All of the statistical tests were two-tailed and a P value less than 0.05 was considered significant. The validation subset was for the regression analysis. All of the variables except age were binary, whereas the age was considered a categorical variable (0–1.5, 1.5–2, 2–3 years and 3+ years) and was converted into a dummy variable. We used the 3+ years group as the reference group, X1 represented the 0–1.5 years group, X2 represented the 1.5–2 yeasr group and X3 represented the 2–3 years group. First, we used a univariate logistic regression analysis to screen out the possible risk factors for cardiopulmonary failure from possible variables and P values smaller than 0.2 were considered statistically significant. Second, a multiple logistic regression analysis was used to examine the multivariate-adjusted odds ratios for risk factors that were significant in the univariate analysis in which the backward stepwise elimination was used. Starting from the weakest predictor, variables were eliminated one by one from the full model until the change in R2 became statistically significant. P values smaller than 0.05 were considered statistically significant. Confounders were taken into consideration. Adjusted odds ratios (OR) and their 95% confidence intervals (95% CIs) were calculated. The Hosmer-Lemeshow test was used to examine the goodness-of-fit. Third, the regression model was built, the receiver operating characteristic curve (ROC curve) was plotted and the area under the curve (AUC) was calculated. We selected the P value as the cut-off when the Youden index was the maximum. Finally, the regression equation obtained was then applied to the test subset and the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy rate were calculated.
Results
Epidemiological information and clinical manifestations
The epidemiological data for the 1,125 patients are shown in Fig. 1. Most of the patients presented with fever (83.9% of the total number of patients), rashes (66.4%), oral ulcers (63.6%) and myoclonus (34.4%) upon disease onset. In addition, these patients also exhibited vomiting, headache, seizures, tachypnea, limb weakness or gait disturbance, irritability, drowsiness and coma during the course of the disease. The 1,125 cases included 95 cases (8.4% of the total patients) of simple HFMD, 1,017 cases (90.4%) associated with CNS involvement (including some with ANS involvement and severe disease), 247 cases (22.0%) with ANS involvement (including some severe cases) and 149 patients (13.2%) with severe disease. The most common neurological complication was myoclonus alone (559 cases, representing 55.0% of the total neurological complications). The other neurological complications observed included encephalitis(289, 28.4%, alone and mixed), meningitis (253, 24.9%), brainstem encephalitis(158, 15.5%) and AFP (50, 4.9%). Detailed numbers of cases showing each type of neurological complication are listed in Table 1. Apart from myoclonus alone, the most common CNS complications during the epidemic season were nearly the same in each month; encephalitis or meningitis. The detailed numbers of cases showing each type of neurological complication in every month are listed in Supplementary Table S3. The average age of the patients with cardiopulmonary failure was younger than that of the simple HFMD patients (p = 0.026) and the average hospital stay of the patients with cardiopulmonary failure was approximately 2.6 times longer than that of the simple HFMD patients (Table 2). Because most patients were discharged after improvement or recovery (1,103, 98.0% of total), the average hospital stay could indirectly reflect the disease duration (Table 2). The average time (±SD) from the onset to CNS involvement was 2.05 (±1.63) days, the average time from CNS involvement to ANS involvement was 2.59 (±1.77) days, the average time from CNS involvement to cardiopulmonary failure was 2.63 (±1.84) days and the average time from ANS involvement to progression to cardiopulmonary failure was 7.80 (±6.14) hours.

Number of Cases of EV-A71-related HFMD hospitalizations in the Children’s Hospital of Hunan province from January 1, 2010 to December 31, 2012.
Auxiliary examinations
A total of 411 patients underwent chest X-ray examination, of which 263 cases were abnormal and the main types of lesions included interstitial changes in both lungs, patchy shadows, pulmonary oedema and pulmonary haemorrhage. A total of 300 patients underwent magnetic resonance imaging (MRI) of the head or spinal cord within three days of entering the hospital (in the progressive stage of the symptoms, except for the patients who had been under endotracheal tubes since their arrival to the emergency unit and whose cardiac and pulmonary functions required closely monitoring) and 85 cases had abnormalities. The main manifestations were hyperintense signals on T2-phase images: 47 patients (accounting for 46.5% of the brainstem encephalitis patients who underwent MRI) demonstrated brainstem abnormalities (lesions involving the pontine tegmentum, medulla oblongata, midbrain and cerebellar dentate nuclei). Thirty-four cases (22.5%) showed brain abnormalities, with lesions involving the cortex, basal ganglia, globus pallidus, thalamus, hippocampus and corpus callosum and seven cases (58.3%) had spinal cord abnormalities, with lesions mainly involving the anterior horn of the cervical or thoracic spinal cord (Fig. 2). In addition, 280 patients underwent electroencephalography (EEG) examination, of which 110 cases presented nonspecific slowing of background activity. Among these patients, three demonstrated sharp waves in certain brain areas (frontal and central) and seizures and one of these patients had a history of epilepsy. Additionally, 40 patients had received electromyography (EMG), of which 21 cases showed neurogenic lesions.

Spin-Echo T2-weighted MRI scan of a 28-month-old boy with encephalitis, brainstem encephalitis and myelitis from EV-A71 infection.
The child had fever; rashes on the mouth, palms and soles of the feet; vomiting; myoclonus; tachypnea; and drowsiness, followed by coma. Physical examination revealed skin rashes, weakness in four limbs, hypermyotonia and positive reflex of Babinski’s sign. At the basal ganglia level (Panel A), there was an increased signal intensity of the bilateral globus pallidus (arrows). At the midbrain level (Panel B), there was an increased signal intensity of the bilateral cerebral peduncle (arrows). At the pons and medulla oblongata level (Panel C,D), lesions of high signal intensity were observed in the bilateral tegmentum (arrows). In the sagittal view (Panel E), there was a high signal intensity from the brain-stem to the anterior horn of the cervical spinal cord (arrows).
Relationships between various factors and cardiopulmonary failure
We selected 23 variables based on the literature and previous clinical experience (shown in Supplementary Table S4) to investigate the effects of these factors on the development of cardiopulmonary failure. We found that young age, fever duration ≥3days, tachypnea, tachycardia, hypertension, capillary refill time (CRT) >2 s, hyperglycaemia, leucocytosis, C-reactive protein (CRP) ≥40 mg/L, myoclonus, vomiting, coma, limb weakness, drowsiness and ANS involement were significant risk factors for cardiopulmonary failure.
We combined tachypnea, tachycardia, hypertension, capillary refill time (CRT) >2 s and hyperglycaemia into one variable, referred to as ANS involvement, because these variables were all clinical manifestations or laboratory results implicating the ANS involvement and appeared on a single patient nearly simultaneously. We did not put leucocytosis and C-reactive protein (CRP) ≥40 mg/L, into the following multivariable logistic regression because not every patient underwent CRP and blood testing.
We then introduced age, fever duration ≥3 days, ANS involvement, myoclonus, vomiting, coma, limb weakness and drowsiness into a multivariate logistic regression model. We found that the respective risk of developing severe disease in the 0–1.5,1.5–2 and 2–3 years age groups were 9.3, (adjusted odds ratio = 9.3[3.6–23.8], p = 0.000), 5.0 (adjusted OR = 5.0[1.9–13.3], p = 0.001) and 5.6 times (adjusted OR = 5.6[2.1–15.0], p = 0.001) greater compared with the age group 3+ years. Additionally, we found that fever duration ≥3 days (adjusted OR = 9.4[1.4–62.5], p = 0.020), coma (adjusted OR = 27.7[5.3–145.4], p = 0.000), limb weakness (adjusted OR = 5.0[2.6–9.6], p = 0.000), drowsinesss (adjusted OR = 4.1[2.5–6.9], p = 0.000) and ANS involvement (adjusted OR = 13.5[8.2–22.3], p = 0.000) were the most significant predictive factors associated with cardiopulmonary failure (Shown in Table 3). The Hosmer-Lemeshow statistics indicated a non-significant lack-of-fit (χ2 = 6.496, p = 0.483).
We drew the ROC curve, which showed an acceptable performance on the validation subset (AUC = 0.916; 95% CI, 0.890–0.941, p = 0.000; Fig. 3, Panel A).

ROC curve of the final model.
Panel (A) is the ROC of the first model, AUC = 0.916; 95% CI, 0.890–0.941, p = 0.000, Panel (B) is the ROC of the second model, AUC = 0.927; 95% CI, 0.903–0.952, p = 0.000, both panels indicate good internal validity.
We applied the model in the test subsets (60 cases) to predict the probability of cardiopulmonary failure in HFMD. It had a sensitivity of 75.0%, a specificity of 81.3%, a PPV of 50.0% and a NPV of 92.9% and it correctly classified 80.0% of cases.
Relationships between neurological complications and cardiopulmonary failure
We also investigated the effects of different neurological complications on disease severity. We collected data from 1,017 cases with neurological complications (excluding the simple HFMD cases in both the validation and test subsets). We found that myoclonus alone, encephalitis alone and meningitis alone were significant protective factors, suggesting that EV-A71-related HFMD patients with only myoclonus, encephalitis or meningitis were less likely to develop cardiopulmonary failure compared with those with other neurological complications. By contrast, brainstem encephalitis alone, some combination of neurological complications (brainstem encephalitis combined with encephalitis, brainstem encephalitis combined with meningitis, brainstem encephalitis combined with AFP, encephalitis combined with AFP and meningitis combined with AFP) and the number of CNS-involved regions were significant risk factors for cardiopulmonary failure. Young age might be a confounder (the detailed unadjusted OR is shown in Supplementary Table S5).
We then introduced these 10 screened significant factors and age into a multivariate logistic regression model. After the confounding factor (age) was adjusted, we found that brainstem encephalitis alone (adjusted OR = 9.4[4.3–22.1], p = 0.000), brainstem encephalitis combined with encephalitis (adjusted OR = 10.5[4.2–26.0], p = 0.000), brainstem encephalitis combined with meningitis (adjusted OR = 2.3[1.0–5.2], p = 0.056) and the number of CNS-involved regions (adjusted OR = 6.3[4.6–8.6], p = 0.000) were the most significant factors associated with cardiopulmonary failure (Shown in Table 3). The Hosmer-Lemeshow statistics indicated a non-significant lack-of-fit (χ2 = 4.420, p = 0.620). Although there were six cases of myoclonus alone that developed into cardiopulmonary failure, they all had symptoms of ANS involvement.
We drew the ROC curve, which showed an acceptable performance on the validation subset (AUC = 0.927; 95% CI, 0.903–0.952, p = 0.000; Fig. 3, Panel B).
We applied the P2 model in the test subsets (57 cases with neurological complications) to predict the probability of cardiopulmonary failure in HFMD. It had a sensitivity of 58.3%, a specificity of 88.9%, a PPV of 58.3% and a NPV of 88.9% and it correctly classified 82.5% of cases.
The detail and the usage of the model was in the supplement.
Treatment and prognosis
In the present study, 482 patients received gamma globulin treatment, 491 patients received high-dose methylprednisolone shock therapy, of which 387 patients combined methylprednisolone shock therapy with IVIG according to Chinese guideline for HFMD25,28,29,30, however, WHO guidelines do not recommend the use of corticosteroids in any severity of HFMD14. A total of nine patients died and one patient withdrew from treatment during hospitalization. During the one year follow-up period after discharge, five patients died (three patients who required ventilator-assisted breathing died several days after discharge, one patient who had difficulty swallowing died two months after discharge and one patient with limb weakness and mental retardation choked while eating and died of suffocation one year after discharge). The mean age (±SD) of the deceased patients was 1.59 (±1.03) years old. In total, 72 patients (6.8%) presented sequelae, their mean MRS(±SD) was 1.96 (±1.79), including 65 patients (5.5%) with abnormal gaits or limb weakness, four patients required long-term assistance of mechanical ventilation, two patients experienced seizures and one patient developed facial paralysis. The mean age (±SD) of the patients with sequelae was 1.78 (±0.98) years old. The sequelae and mortality rates were 7.1% and 1.5% for CNS involvement, respectively, whereas the sequelae and mortality rates were 33.6% and 9.4% for cardiopulmonary failure, respectively.
Discussion
From January 2010 to December 2012 in the Hunan province, the major peak incidence of HFMD occurred each year from May to July and a minor high peak occurred in November.
Among the viruses that cause HFMD, EV-A71 and CV-A16 were the most common and EV-A71 was more likely to cause neurological complications and cardiopulmonary failure31. We did not find that CV-A16 could easily cause neurological complications or cardiopulmonary failure. Our cases confirmed that EV-A71 infection can cause the following neurological complications: encephalitis, meningitis, brainstem encephalitis and AFP. The most common symptom associated with neurological complications was myoclonus; furthermore, encephalitis and meningitis were the most common neurological complications associated with EV-A71-related HFMD apart from simple myoclonus. MRI showed that the most frequently involved brainstem area was the pontine tegmentum and the most frequently involved spinal cord area was the anterior horn; these findings are consistent with previous reports17,20,32,33.
Chen et al. analysed the EV71 epidemiological characteristics in Taiwan during a period of eight years and concluded that children of approximately 0.5–1 years of age demonstrated the highest mortality34. Our study also found that young age was a risk factor for cardiopulmonary failure, particularly 0–1.5 years old. Chang et al.26 reported that hyperglycaemia, leucocytosis and limb weakness were the most significant risk factors for pulmonary oedema. Li et al.35 analysed the clinical characteristics of HFMD in China in a meta-analysis and concluded that blood glucose levels and WBC counts become elevated as the disease progresses. Fever duration, abnormal heart rate variability, vomiting and impaired consciousness have also been reported to be correlated with cardiopulmonary failure2,36,37,38. In 2014, a mata- analysis was conducted regarding the risk factors for severe HFMD: this study found that a duration of fever ≥3 days, lethargy, hyperglycaemia and young age were significantly related to the risk of severe HFMD39. Our data quantitatively confirmed the correlations between these risk factors and cardiopulmonary failure by univariate analysis. In addition, we found that tachypnea, hypertension, CRT >2 s and CRP ≥40 mg/L were also risk factors; and among the above factors, our results revealed that young age, fever duration ≥3 days, coma, limb weakness, drowsiness and ANS involvement were more significantly associated with cardiopulmonary failure. Apart from age and fever duration, the above risk factors mainly focused on the ANS symptoms (hyperglycaemia, abnormal heart rate, tachypnea, hypertension, CRT >2 s) and CNS symptoms (limb weakness, vomiting and impaired consciousness), ANS invovlement often develops into cardiopulmonary failure within several hours and interventions to prohibit disease progression become difficult once this occurs. Therefore, ANS-related risk factors are not helpful clinical predictors of cardiopulmonary failure. Our results revealed that the mean time from onset to CNS involvement was 2.05 ± 1.63 days and the mean time from CNS involvement to cardiopulmonary failure (2.63 ± 1.84 days) was generally more than 24 hours. The involvement of different part of the CNS invovled may lead to different outcomes; thus, in addition to observing CNS symptoms and signs, we should determine which regions of the CNS are affected by complications and which types of neurological complications have more predictive value to identify cardiopulmonary failure.
The Guide14 recommends that simple myoclonus and cerebrospinal fluid lymphocytosis may be considered to indicate brainstem encephalitis under limited conditions. Most of our patients demonstrated clinical manifestations of myoclonus (963 cases, accounting for 85.6% of the total cases), of which 559 cases showed myoclonus alone (49.7%). In addition, of the 305 patients with routine lumbar puncture, 196 cases (17.4%) showed cerebrospinal fluid (CSF) lymphocytosis. The majority of these cases had good prognoses and there was no significant correlation between myoclonus/CSF lymphocytosis and cardiopulmonary failure. By contrast, there were 158 cases (14.0%) of brainstem encephalitis of which 60.8% developed cardiopulmonary failure. Therefore, the misdiagnosis of myoclonus alone as brain stem encephalitis may interfere with determining patient prognosis. Because the present study was a retrospective analysis, subtle signs and symptoms were not recorded; therefore, we could not accurately estimate the myoclonic frequency, location and time, which should be improved in future clinical and research work. However, if HFMD paediatric patients present with myoclonus alone and do not exhibit other nervous system damage or manifestations of ANS dysfunction, these patients should have a good prognosis. This is particularly significant in China. With the rapid economic growth of China and improvements in the standard of living, increasing numbers of middle class families demand optimal care. Moreover, because of concerns of the poor health services of rural hospitals, most of the patients brought their children to an urban hospital, leading to the urban hospital overwhelmed. At the peak of the HFMD pandemic, there were insufficient hospital beds for all of the patients who required hospitalization. Hence, it is very important to rapidly predict the prognosis of patients and reserve beds for paediatric patients with cardiopulmonary failure.
The present study confirmed that brainstem encephalitis alone, particular neurological complications (brainstem encephalitis with encephalitis, brainstem encephalitis with meningitis) and the number of CNS-involved regions were significant risk factors for cardiopulmonary failure. The reticular activating system (RAS) originates in the upper brainstem reticular core; therefore, when the brainstem is affected, the RAS is damaged, leading to autonomic dysfunction and cardiopulmonary failure26. A greater number of CNS-involved regions indicates a more extensive range of viral invasion and more cardiopulmonary failure. Therefore, if paediatric patients present neurological symptoms and signs of damage to the brainstem and cerebellum, such as cranial nerve damage, crossed paralysis or crossed sensory disturbances, ataxia, nystagmus, or changes in brainstem MRI imaging, close monitoring should be conducted and interventions should be implemented as early as possible.
Encephalitis alone may not have been a risk factor because the Guide14 defines seizures as a symptom of encephalitis. However, the seizures are more likely to be simple febrile seizures2,40 and not a symptom of encephalitis if they occur in children 6 to 60 months old and are accompanied by fever (temperature ≥38.0 °C) and if the patient quickly regains consciousness. These patients have a good prognosis because only 1% of febrile seizures will lead to epilepsy41 and this type of seizure is often misdiagnosed as encephalitis and over-treated. Aseptic meningitis also had a good prognosis, which is consistent with previous reports42. In the present study, AFP alone (four cases) was not identified as a risk factor, which may be because the fact that the number of AFP cases in our study was small. Specifically, our study included 50 AFP cases of which 46 cases were combined with other neurological complications. Brainstem encephalitis combined with AFP, encephalitis combined with AFP and meningitis combined with AFP were risk factors for cardiopulmonary failure and the univariate logistic regression analysis of the relationship between AFP (simple and mixed) and cardiopulmonary failure showed that AFP remained a risk factor for cardiopulmonary failure (odds ratio 10.9[6.0–19.8], P = 0.000).
EV-A71-related severe HFMD presents high rates of mortality and sequelae because of the lack of specific antiviral drugs. If young HFMD paediatric patients with a fever duration ≥3 days present neurological symptoms, a neurological examination should be carefully conducted and the locations of the impaired regions of the nervous system should be quickly and accurately determined; if necessary, help from a neurologist may be required. For cases showing only myoclonus or only simple febrile seizures without other CNS or ANS symptoms, the patients can be followed at outpatient clinics or emergency rooms to avoid excessive medical treatment. If impaired consciousness or limb weakness occurs, if neurological symptoms and signs of brainstem and cerebellum involvement are present, or if multiple regions of the nervous system are affected, the patients should receive immediate intensive care and complete examinations, such as an ANS evaluation (respiration, heart rates, blood pressure, blood glucose monitoring and CRT) and CRP, blood testing, cardiopulmonary functional detection, MRI and lumbar puncture in a timely manner. Moreover, intervention should be conducted as early as possible to reduce the mortality and sequelae rates of EV-A71-related HFMD. However, the methods used in this study may not be the most optimal without high sensitivity and we should be cautious to apply it. In addition, the treatment for patients may be a confounder and should be considered in the future.
Additional Information
How to cite this article: Long, L. et al. Neurological complications and risk factors of cardiopulmonary failure of EV-A71-related hand, foot and mouth disease. Sci. Rep. 6, 23444; doi: 10.1038/srep23444 (2016).
References
Schmidt, N. J., Lennette, E. H. & Ho, H. H. An apparently new enterovirus isolated from patients with disease of the central nervous system. J Infect Dis 129, 304–309 (1974).
Ooi, M. H., Wong, S. C., Lewthwaite, P., Cardosa, M. J. & Solomon, T. Clinical features, diagnosis and management of enterovirus 71. Lancet Neurol 9, 1097–1105 (2010).
McMinn, P., Stratov, I., Nagarajan, L. & Davis, S. Neurological manifestations of enterovirus 71 infection in children during an outbreak of hand, foot and mouth disease in Western Australia. Clin Infect Dis 32, 236–242 (2001).
Chan, L. G. et al. Deaths of children during an outbreak of hand, foot and mouth disease in sarawak, malaysia: clinical and pathological characteristics of the disease. For the Outbreak Study Group. Clin Infect Dis 31, 678–683 (2000).
Chan, K. P. et al. Epidemic hand, foot and mouth disease caused by human enterovirus 71, Singapore. Emerg Infect Dis 9, 78–85 (2003).
Ho, M. et al. An epidemic of enterovirus 71 infection in Taiwan. Taiwan Enterovirus Epidemic Working Group. N Engl J Med 341, 929–935 (1999).
Yang, F. et al. Enterovirus 71 outbreak in the People’s Republic of China in 2008. J Clin Microbiol 47, 2351–2352 (2009).
National Bureau of Statistics of the People’s Republic of China. Statistical Yearbook of China 2008. (China Statistics Press, 2009).
National Bureau of Statistics of the People’s Republic of China. Statistical Yearbook of China 2012. (China Statistics Press, 2013).
Zhu, F. C. et al. Efficacy, safety and immunology of an inactivated alum-adjuvant enterovirus 71 vaccine in children in China: a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 381, 2024–2032 (2013).
Zhu, F. et al. Efficacy, safety and immunogenicity of an enterovirus 71 vaccine in China. N Engl J Med 370, 818–828 (2014).
Li R. et al. An Inactivated Enterovirus 71 Vaccine in Healthy Children. N Engl J Med 370, 829–837 (2014).
Liu, S. L. The Hunan Children’s Hospital accepted 500 children with hand, foot and mouth disease in a day. Xinhua Net.(2012) Available at: http://www.hn.xinhuanet.com/2012-05/20/c_111993309.htm (Accessed: 20th May 2012).
World Health Organization. Clinical Features and Case Management. In A guide to clinical management and public health response for hand, foot and mouth disease (HFMD) 35–39 (World Health Organization, 2011)
Ooi, M. H. et al. Identification and validation of clinical predictors for the risk of neurological involvement in children with hand, foot and mouth disease in Sarawak. BMC Infect Dis 9, 3(2009).
Yan, J. J., Wang, J.,. R., Liu, C. C., Yang, H. B. & Su, I. J. An outbreak of enterovirus 71 infection in Taiwan 1998: a comprehensive pathological, virological and molecular study on a case of fulminant encephalitis. J Clin Virol 17, 13–22 (2000).
Wang, S. M. et al. Clinical spectrum of enterovirus 71 infection in children in southern Taiwan, with an emphasis on neurological complications. Clin Infect Dis 29, 184–190 (1999).
Komatsu, H., Shimizu, Y., Takeuchi, Y., Ishiko, H. & Takada, H. Outbreak of severe neurologic involvement associated with Enterovirus 71 infection. Pediatr Neurol 20, 17–23 (1999).
Lum, L. C. et al. Fatal enterovirus 71 encephalomyelitis. J Pediatr 133, 795–798 (1998).
Huang, C. C. et al. Neurologic complications in children with enterovirus 71 infection. N Engl J Med 341, 936–942 (1999).
Lu, H. K. et al. Prognostic implications of myoclonic jerk in children with enterovirus infection. J Microbiol Immunol Infect 37, 82–87 (2004).
Lai, Y. Y. & Siegel, J. M. Brainstem-mediated locomotion and myoclonic jerks. I. Neural substrates. Brain Res 745, 257–264 (1997).
Viral Nucleic Acid Extraction Kit II. Available at: http://www.geneaid.com/sites/default/files/VR8_0.pdf (Accessed: 27th November 2014)
Xiao, X. L. et al. Simultaneous detection of human enterovirus 71 and coxsackievirus A16 in clinical specimens by multiplex real-time PCR with an internal amplification control. Arch Virol, 154, 121–125(2009).
The national health and family planning commission of the People’s Republic of China. A guide to clinical management of hand, foot and mouth disease (HFMD). (2010) Available at: http://www.nhfpc.gov.cn/yzygj/s3593g/201306/6d935c0f43cd4a1fb46f8f71acf8e245.shtml(Accessed: 20th April 2010)
Chang, L. Y. et al. Clinical features and risk factors of pulmonary oedema after enterovirus-71-related hand, foot and mouth disease. Lancet 354, 1682–1686 (1999).
van Swieten, J. C. et al. Interobserver agreement for the assessment of handicap in stroke patients. Stroke, 19, 604–607(1988).
Ye, N. et al. Cytokine responses and correlations thereof with clinical profiles in children with enterovirus 71 infections. BMC Infect Dis, 15, 225(2015).
Jiang, M. & Wang, X. C. Clinical research of early, enough methylprednisone combined with immunoglobulin in treatment of severe hand-foot-mouth disease. Zhonghua Shi Yan He Lin Chuang Bing Du Xue Za Zhi, 27, 363–365 (2013).
Teoh, H. L. et al. Clinical Characteristics and Functional Motor Outcomes of Enterovirus 71 Neurological Disease in Children. JAMA Neurol, 19, 1–8 (2016).
Chen, S. P. et al. Comparison of clinical features between coxsackievirus A2 and enterovirus 71 during the enterovirus outbreak in Taiwan, 2008: a children’s hospital experience. J Microbiol Immunol Infect 43, 99–104 (2010).
Zeng, H., Wen, F., Gan, Y. & Huang, W. MRI and associated clinical characteristics of EV71-induced brainstem encephalitis in children with hand-foot-mouth disease. Neuroradiology 54, 623–630 (2012).
Zimmerman, R. D. MR imaging findings of enteroviral encephalomyelitis: an outbreak in Taiwan. AJNR Am J Neuroradiol 20, 1775–1776 (1999).
Chen, S. C., Chang, H. L., Yan, T. R., Cheng, Y. T. & Chen, K. T. An eight-year study of epidemiologic features of enterovirus 71 infection in Taiwan. Am J Trop Med Hyg 77, 188–191 (2007).
Li, Y., Zhu, R., Qian, Y. & Deng, J. The characteristics of blood glucose and WBC counts in peripheral blood of cases of hand foot and mouth disease in China: a systematic review. PLoS One 7, e29003 (2012).
Lin, M. T. et al. Heart rate variability monitoring in the detection of central nervous system complications in children with enterovirus infection. J Crit Care 21, 280–286 (2006).
Yang, T., Xu, G., Dong, H., Ye, M. & He, T. A case-control study of risk factors for severe hand-foot-mouth disease among children in Ningbo, China, 2010–2011. Eur J Pediatr 171, 1359–1364 (2012).
Chong, C. Y. et al. Hand, foot and mouth disease in Singapore: a comparison of fatal and non-fatal cases. Acta Paediatrica 92, 1163–1169 (2003).
Fang, Y., et al. Risk factors of severe hand, foot and mouth disease: A meta-analysis. Scand J Infect Dis 46, 515–522 (2014).
Subcommittee on Febrile Seizures. & American Academy of Pediatrics. Neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics 127, 389–394 (2011).
Valman, H. B. ABC of one to seven. Febrile convulsions. BMJ 306, 1743–1745 (1993).
Michos, A. G. et al. Aseptic meningitis in children: analysis of 506 cases. PLoS One 8, e674 (2007).
Acknowledgements
We thank Zongwei Yue, Hui Li, Nan Lv, Yujiao Fu, Qihua Chen, Haiyue Zhang, Xuehui Qin, Hongjun Fang, Jinbiao Chen and Ying Fu for their assistance related to the study. We thank the language editing services “Nature Publishing Group Language Editing” for checking the spelling and grammar in the manuscript. This work was supported by the National Natural Science Foundation of China [Grant No. 81201001] and China Preventive Medicine Association [Grant No. 20101801].
Author information
Authors and Affiliations
Contributions
L.L. and L.X. were responsible for the study design, data collection, data analysis and the writing of the paper. B.X. was the coordinator, designed the study and revised the paper. Z.X., R.L., L.Y., Z.X. and X.S. were responsible for data collection. S.H. and K.L. contributed to data collection and viral confirmation. H.W. and X.L. were in charge of collection of imaging data. Y.S. helped to interpret the imaging data. L.Z., H.L., J.G., M.Z. and L.F. performed the work of collecting and interpreting the medical records. X.F. and X.Y. critically reviewed the paper. L.Z. gave advice on statistical analysis.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Long, L., Xu, L., Xiao, Z. et al. Neurological complications and risk factors of cardiopulmonary failure of EV-A71-related hand, foot and mouth disease. Sci Rep 6, 23444 (2016). https://doi.org/10.1038/srep23444
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep23444
This article is cited by
-
Changing serotypes of hand, foot and mouth disease in Shanghai, 2017–2019
Gut Pathogens (2022)
-
Co-infection and enterovirus B: post EV-A71 mass vaccination scenario in China
BMC Infectious Diseases (2022)
-
Neurotropic EV71 causes encephalitis by engaging intracellular TLR9 to elicit neurotoxic IL12-p40-iNOS signaling
Cell Death & Disease (2022)
-
Association of environmental factors and high HFMD occurrence in northern Thailand
BMC Public Health (2020)
-
Dysregulated autophagy contributes to the pathogenesis of enterovirus A71 infection
Cell & Bioscience (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
