
Abstract
This retrospective cohort study aimed to evaluate the prognostic value of the alpha-fetoprotein (AFP) response in advanced-stage hepatocellular carcinoma (HCC) patients treated with sorafenib combined with transarterial chemoembolization. From May 2008 to July 2012, 118 HCC patients with baseline AFP levels >20 ng/ml treated with combination therapy were enrolled. A receiver operating characteristic curve was used to generate a cutoff point for AFP changes for predicting survival. The AFP response was defined as an AFP decrease rate [ΔAFP(%)] greater than the cutoff point. The ΔAFP(%) was defined as the percentage of changes between the baseline and the nadir values within 2 months after therapy. The median follow-up time was 8.8 months (range 1.2–66.9). A level of 46% was chosen as the threshold value for ΔAFP (sensitivity = 53.7%, specificity = 83.3%). The median overall survival was significantly longer in the AFP response group than in the AFP non-response group (12.8 vs. 6.4 months, P = 0.001). Multivariate analysis showed that ECOG ≥ 1 (HR = 1.95; 95% CI 1.24–3.1, P = 0.004) and AFP nonresponse (HR = 1.71; 95% CI 1.15–2.55, P = 0.009) were associated with increased risk of death. In conclusion, AFP response could predict the survival of patients with advanced-stage HCC at an early time point after combination therapy.
Similar content being viewed by others

Introduction
Hepatocellular carcinoma (HCC) is the sixth most common cancer worldwide with more than 800,000 newly diagnosed cases per year1. It is the second most common cause of cancer-related death in the world2. A large proportion of HCC patients are diagnosed at an intermediate or advanced stage beyond curative treatments. Based on the Barcelona Clinic Liver Cancer (BCLC) staging system, transarterial chemoembolization (TACE) and sorafenib are the standard treatments for intermediate and advanced-stage HCC, respectively3,4. Because Sorafenib may improve the efficacy of TACE therapy by decreasing post-TACE angiogenesis, sorafenib combined with TACE has been considered to be a promising therapy5,6,7. Although the preliminary results of the first randomized controlled (SPACE) trial were disappointing as the time to progression (TTP) failed to show a significant difference, we consider that the reason for the failure may lie in the study design. The other trials in this field are still underway. The answer regarding the superiority of combination therapy will be provided by the results of these trials in the future.
Currently, radiological imaging evaluation is widely used for the prognostic assessment of HCC. The Response Evaluation Criteria in Solid Tumors (RECIST) focuses on whole-tumor shrinkage8. The modified RECIST (mRECIST) criteria measure the change of the tumor necrotic area. However, radiological imaging evaluation has several limitations9. First, it is challenging to measure tumor size when the tumor grows in a diffuse pattern. Second, radiological imaging evaluation is a relatively subjective assessment and lacks inter-observer reproducibility10. Third, our previous studies showed that RECIST and mRECIST criteria fail to predict survival at an early time point11. Therefore, alternative methods to estimate treatment efficacy are needed.
Alpha-fetoprotein (AFP) is a glycoprotein that is secreted in approximately 70% of HCC12. As the most common biomarker of HCC, AFP has confirmed its value in screening and diagnoses in multiple studies13. Recently, several studies unanimously suggested that the AFP response was associated with longer overall survival (OS) in HCC patients after locoregional treatment modalities or systematic chemotherapy14,15. However, the prognostic value of the AFP response in patients with advanced-stage HCC who are treated with sorafenib combined with TACE remains unclear.
The aim of this study was to evaluate the prognostic value of the AFP response in patients with advanced HCC who were undergoing treatment with sorafenib combined with TACE and to explore the correlation between the AFP response and a radiological evaluation from an early time point.
Materials and Methods
All HCC patients consecutively admitted to our department between May 2008 and June 2012 who were treated with a combination therapy of sorafenib and TACE were retrospectively considered in our study. The inclusion criteria were as follows: 1) an age ≥18 years old, 2) an interval between sorafenib and TACE of ≤60 days, 3) an Eastern Cooperative Oncology Group (ECOG) performance status score ≤2, 4) a Child-Pugh A or B (≤7) and 5) no other molecular target agents. The exclusion criteria were as follows: 1) main portal vein invasion,2) concurrent malignancy,3) an absence of a repeat AFP measurement within 2 months after treatment initiation,4) a baseline AFP < 20 ng/ml and 5) poor compliance. The diagnosis of HCC was based on the American Association for the Study of Liver Disease (AASLD) criteria16. Histology was needed only in case of diagnostic uncertainty. OS was measured from the beginning of combination therapy to the date of death or the last follow-up. The requirement to obtain informed consent was waived. The study protocol was approved by the ethics committees of Xijing Hospital. All the methods used in this study were carried out according to the approved guidelines.
Treatment and follow-up
The patients received sorafenib at an initial dose of 400 mg twice daily. Later, the dose of sorafenib was modified based on the degree of adverse events (AEs). AEs were assessed according to the National Cancer Institute Common Terminology Criteria for Adverse Events version 4.0. In our clinical practice, patients continue sorafenib treatment if the AEs can be safely controlled. TACE was performed using 10–50 mg doxorubicin mixed with 5–20 mg lipiodol. Gelatin foam was injected until the tumor-feeding vessels were completely obstructed. TACE procedures were repeated according to the radiological response5. Combined therapy was defined as an interval between sorafenib and TACE of less than 60 days, regardless of the order of the two treatments. Standard follow-up evaluations, including contrast-enhanced computer tomography (CT) scans and laboratory assessments, were performed during weeks 4 and 8 after the initiation of treatment and every 8 weeks thereafter. The end of the follow-up period was either death or December 31st 2014.
AFP evaluation
The serum AFP concentration was measured at baseline (before the initiation of combined therapy) and at every follow-up visit using an electro chemiluminescence immunoassay (ElecsysCobas e601, Roche). The AFP variation rate (ΔAFP) was defined as the percentage of change between the baseline and the nadir within 1–2 months after combination therapy.

The AFP response was defined as an ΔAFP(%) greater than the cutoff point (ΔAFP(%) > cutoff point), whereas AFP non-response was defined as an AFP decrease rate less than the AFP variation cutoff point (ΔAFP(%) < cutoff point). The researcher who extracted the AFP data was blinded to the survival outcome.
Radiological evaluation and definitions
Radiological imaging assessments were performed with contrast-enhanced spiral computed tomography (CT) at baseline (before the initiation of combined therapy) and at every follow-up visit after combined therapy. The RECIST and mRECIST criteria were used for radiological evaluation. The treatment responses were blindly assessed by three experienced clinicians (Yan Zhao, JiaJia and Wei Bai). In cases of discrepancies, the images were jointly reviewed by all of the clinicians and a consensus decision was reached. If the patients were evaluated as having a complete response (CR) or a partial response (PR) within 2 months after combination therapy, these individuals were considered to be responders. If the patients were evaluated as having stable disease (SD) or progressive disease (PD), these individuals were considered to be non-responders17.
Statistical analyses
Continuous variables were presented as median values with ranges and categorical variables were presented as frequencies with percentages. A receiver operating characteristic (ROC) curve was used to generate a cutoff point for AFP changes that predicted survival. For the area under the curve, a cutoff point with the highest sum of sensitivity and specificity was chosen as the most discriminative value of the AFP response for predicting survival. This statistic may range from 0 to 1 and cutoff points with a c-statistic >0.7 are generally considered useful18. A Mann-Whitney U test was used to compare continuous variables, whereas a Chi-squared test was used to compare categorical variables between the AFP response and non-response groups. The Κ coefficient was used to measure the inter-method concordance of the radiological response and the AFP response. OS time was assessed by Kaplan-Meier methods and the survival difference between groups was estimated by the log-rank test. Patients lost to follow-up or alive at the end-of-observation date were censored. Univariate and multivariate Cox regression analyses were used to test the prognostic factors of OS. Variables with a P value < 0.1 in the univariate analysis were included in the multivariate analysis. Statistical analyses were performed using SPSS version 16.0 (SPSS, Inc., Chicago, IL, USA). A two-sided P value < 0.05 was considered to be statistically significant.
Results
Patient characteristics and treatment
A total of 118 patients with unresectable HCC were included in our study (Fig. 1). The median age was 48 years (range, 23–75 years). Most patients were male (86.4%) and had hepatitis B virus infection (89%), Child-Pugh class A (90.7%), an ECOG performance status of 1–2 (74.6%) and BCLC stage C (83.9%). In total, 47 (66.9%) patients had branch portal vein tumor thrombosis (PVTT). Extrahepatic spread was observed in 45 (38.1%) patients, mainly in the abdominal lymph nodes (46.5%), the lungs (39.5%) and skeleton (16.3%) (Table 1). The median number of sessions of TACE was 2 (range, 1–12), the median time taking sorafenib was 6.6 months (range 0.3–66.9 months) and the median interval between sorafenib and TACE was 3 days (range 0–55 days). The interval was <7 days for 108 patients (91.5%), was <15 days for 8 patients and 15–55 days for 2 cases. The median baseline AFP level was 1821.5 ng/ml (range 20.7–121000 ng/ml), 25 (21.2%) patients had <200 ng/ml and 93 (78.8%) patients had ≥200 ng/ml.

Enrollment and outcomes.
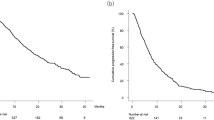
Survival analysis
The median follow-up time was 8.8 months (range, 1.2–66.9). By the end of follow-up, 111 out of 118 patients (94.1%) died and 7 (5.9%) survived. The overall median survival was 8.7 months (95% CI, 6.5–10.9) (Fig. 2A). The median OS was 11.3 months (95% CI, 6.9–15.8) in the patients with PVTT and 8.7 months (95% CI, 5.1–8.9) in the patients without PVTT (P = 0.011) (Fig. 2B). The median OS of the patients with ECOG 0 was longer than that of patients with ECOG ≥ 1 (13.7 months vs. 7.6 months, P = 0.002) (Fig. 2C). The difference in OS between patients with extrahepatic metastasis and those without metastasis was not significant (10.4 months vs. 7 months, P = 0.1) (Fig. 2D).

The Kaplan-Meier analysis of overall survival.
(A) Overall survival. (B) A comparison of survival according to portal vein thrombosis. (C) A comparison of survival according to the ECOG score. (D) A comparison of survival times according to extrahepatic metastasis.
A comparison between AFP response and non-response groups
The median time from the baseline treatment to AFP follow-up was 1.4 months (range 0.4–2.0). The area under the ROC curve (c-statistic) for predicting survival was 0.716 (Fig. 3). The most discriminative value of the ΔAFP(%) for predicting survival was 46%. This cutoff point had a sensitivity of 53.7% and a specificity of 83.3%.

The ROC curve for AFP values and survival.
In this study, 49 (41.5%) patients with ΔAFP(%) > 46% were classified into the AFP response group and 69 (58.5%) patients with ΔAFP(%) < 46% were classified into the non-response group. Most baseline clinical characteristics were similar between the AFP response and non-response groups, but the proportion of males was higher in the AFP response group than in the non-response group (Table 1). The median OS was significantly longer in the AFP response group (12.8 months, 95% CI 10.2–15.3) than in AFP non-response group (6.4 months, 95% CI4.7–8.1) (P = 0.001) (Fig. 4A). Multivariate analysis showed that ECOG ≥ 1 (HR = 1.95; 95% CI 1.24–3.1, P = 0.004) and AFP nonresponse (HR = 1.71; 95% CI 1.15–2.55, P = 0.009) were associated with increased risk of death (Table 2).

The Kaplan-Meier analysis of overall survival.
(A) A comparison between the AFP response and nonresponse groups in the entire cohort; (B) A comparison between RECIST response and nonresponse groups in 84 patients with radiological response; (C) A comparison between mRECIST response and nonresponse groups in 84 patients with radiological response; (D) A comparison between the AFP response and nonresponse groups in 34 patients without radiological evaluation.
The correlation between AFP response and radiological evaluation
Of the 118 patients, 84 (71.2%) were properly evaluated according to both RECIST and mRECIST criteria. Survival was of insufficient time to carry out contrast-enhanced CT scans in 1 patient, 3 patients did not have a complete imaging examination due to clinical deterioration, 10 patients had non-measurable diffused tumor lesions in the liver and 20 patients did not have completely preserved follow-up image data. The median time for assessing radiological imaging response was 1.2 months (range, 0.7–2.0 months). The rates of CR, PR, SD and PD were 0, 7 (8.3%), 66 (78.6%) and 11 (13.1%), respectively, according to the RECIST criteria and 24 (28.6%), 23 (27.4%), 30 (35.7%) and 7 (8.3%), respectively, according to the mRECIST criteria. The response rates (CR and PR) and nonresponse rate (SD and PD) were 8.3% and 91.7% according to the RECIST criteria and 56% and 44% according to the mRECIST criteria, respectively. With RECIST criteria, the median survival value of response group was not obtained because too few patients (n = 7) were classified into this group and 4 patients were censored. However, there was no difference between the response and nonresponse groups (P = 0.132) (Fig. 4B). With mRECIST criteria, the survival difference was not statistically significant between the response and nonresponse groups [14.8 months (95% CI 10.9–18.7) vs. 10.3 months (95% CI 6.8–13.8), P = 0.075] (Fig. 4C). Multivariate analysis showed that both the RECIST (HR = 2.2; 95% CI 0.9–5.6, P = 0.094) and mRECIST (HR = 2; 95% CI 0.9–2.2, P = 0.160) criteria were not independent predictors of overall survival. The outcomes of both the radiological assessment and AFP response are shown in Table 3. The patient evaluation in every response category was markedly different between the RECIST criteria and the AFP response (Κ = 0.077), whereas the majority of patients were classified into the same response categories when assessed using the mRECIST criteria and the AFP response. However, the agreement was still weak between the mRECIST criteria and the AFP response (Κ = 0.383).
Of the 34 patients without radiological evaluation, 8 and 26 patients were in the AFP response and AFP non-response groups, respectively. The median OS was significantly longer in the AFP response group than in the AFP non-response group (11.3 months vs. 3.9 months, P = 0.002) (Fig. 4D).
Discussion
Because AFP assessment is a simple and reproducible method to for the evaluation of the efficacy of combination treatment, our study demonstrates the feasibility of using the dynamic trend of AFP as an early biomarker for predicting survival outcomes after combination therapy in advanced HCC patients.
AFP is a well-established tumor marker for screening and diagnosing HCC and the AFP level appears to be associated with the prognosis of HCC patients19. Previous studies demonstrated that an elevated AFP level would decrease in HCC patients after hepatic resection and would rebound in cases of HCC recurrence20. Recently, the AFP response has been reported to be a significant prognostic factor in HCC patients treated with different locoregional modalities or systemic chemotherapy14,15,21. To our knowledge, the current analysis is the first exploration of the potential prognostic value of the AFP response in HCC patients treated with sorafenib combined with TACE. And our study population was mainly consisted of advanced stage HCC patients, which was different from previous report. The major findings of this study were as follows: 1) the adaptive AFP variation cutoff point to predict prognosis was a 46% reduction, 2) the AFP response (a decline of more than 46% from baseline within 2 months after the initiation of combination therapy) was associated with longer OS in patients with advanced-stage HCC who were treated with sorafenib in combination with TACE and 3) the AFP response could predict the overall survival at an earlier time point compared to radiological assessment, particularly in circumstances in which radiological evaluation could not be performed.
In previous studies, the AFP response was defined as an AFP level that decreased by more than 20%, 30% or 50%14,22,23. However, the definition of the AFP response mostly originated from personal clinical experiences or speculation but not from statistical analyses. In contrast, we used a ROC curve to generate an adaptive AFP variation cutoff point (an AFP reduction of 46%) for the AFP response. More importantly, by using this cutoff point the AFP response group had significantly longer survival than the AFP nonresponse group and it was an independent predictor for overall survival. Thus, the AFP level could be incorporated into the algorithm for assessing the prognosis of HCC patients. Additionally, it should be noted that patient selection in previous studies was different from ours. In previous studies, patients with baseline AFP < 100 ng/ml or <200 ng/ml were excluded to differentiate from other benign liver diseases14,21. Thus, the conclusions of these studies were suitable only for patients with a relatively high baseline AFP level. In contrast, our inclusion criteria were relatively wider, only patients with a baseline AFP < 20 ng/ml were excluded from our study because not all HCC patients have an elevated AFP level.
Radiological evaluations, such as those based on RECIST and mRECIST criteria responses, have been widely used in the prognostic assessment of HCC17,24. Radiological response has also been established to correlate with the pathological response25,26. However, in the current study, both the RECIST and mRECIST assessment within 2 months after treatment were not independent predictors of overall survival. Additionally, the agreement between radiological assessment and the AFP response was weak regardless of whether the RECIST or mRECIST criteria were used, though a majority of patients were classified into the same response categories when assessed using the mRECIST criteria and the AFP response. These results were consisted with our previous study that showed that the earliest time to evaluate the response to combination therapy was 3 months11. This result could be explained by the reality that the baseline tumor burden in Chinese patients is higher than those reported in western countries. Only one TACE session may not be efficient enough to achieve complete tumor response. Moreover, the study by Georgiades et al. showed that initial nonresponders after the first TACE session could obtain prolonged survival from further treatment27. Therefore, under these circumstances, radiological assessment could not be used as an early predictor of overall survival. Additionally, our study demonstrated that the AFP response could predict the prognosis of these patients in the absence of a radiological evaluation, especially in patients with diffuse malignant tumors that could not be evaluated by radiological criteria. Hypovascular or diffusely infiltrative tumor patterns are often present in real-world clinical settings22. Establishing a correlation between AFP and treatment efficacy has the potential to help assess treatment response in clinical practice when the standard imaging findings are equivocal. Another potential advantage of the AFP assessment would be reducing the cost burden of repeat radiological scans.
Several limitations of this study should be recognized. First, this was a retrospective study with a relatively small number of patients. A potential bias may exist because not all the patients had follow-up AFP assessments within 2 months after treatment and consequently only the patients with complete follow-up information were included in the analysis. Further well-design prospective studies with large sample sizes are needed to confirm the prognostic value of the AFP response. Second, the serum AFP concentration might be influenced by hepatitis, cirrhosis and liver cell necrosis. Not all HCC patients have a significantly elevated AFP level at baseline and patients with viral hepatitis and other benign liver diseases incidentally do have an elevated AFP level28,29. An AFP reduction might also be induced not only by treatment for HCC but also by antiviral or anti-fibrosis therapy. Unfortunately, the related data were lacking because we did not collect follow-up information about these types of therapies. Third, the 46% cut-off point was based on this study cohort that mainly consisted of advanced stage HCC patients. Its application in patients with intermediate stage HCC requires further validation.
In conclusion, our study suggested that the AFP response could predict overall survival in advanced-stage HCC patients at an early time point after the treatment of sorafenib combined with TACE. Further prospective studies are necessary to validate the prognostic effect of a decline of 46% as an accurate AFP variation cutoff point.
Additional Information
How to cite this article: Liu, L. et al. The Prognostic Value of Alpha-Fetoprotein Response for Advanced-Stage Hepatocellular Carcinoma Treated with Sorafenib Combined with Transarterial Chemoembolization. Sci. Rep. 6, 19851; doi: 10.1038/srep19851 (2016).
References
de Lope, C. R., Tremosini, S., Forner, A., Reig, M. & Bruix, J. Management of HCC. J Hepatol 56 Suppl 1, S75–87 (2012).
Global battle against cancer won’t be won with treatment alone–effective prevention measures urgently needed to prevent cancer crisis. Cent Eur J Public Health 22, 23–28 (2014).
EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 56, 908–943 (2012).
Llovet, J. M. et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 359, 378–390 (2008).
Zhao, Y. et al. Sorafenib combined with transarterial chemoembolization for the treatment of advanced hepatocellular carcinoma: a large-scale multicenter study of 222 patients. Ann Oncol 24, 1786–1792 (2013).
Pawlik, T. M. et al. Phase II trial of sorafenib combined with concurrent transarterial chemoembolization with drug-eluting beads for hepatocellular carcinoma. J Clin Oncol 29, 3960–3967 (2011).
Park, J. W. et al. Phase II study of concurrent transarterial chemoembolization and sorafenib in patients with unresectable hepatocellular carcinoma. J Hepatol 56, 1336–1342 (2012).
Therasse, P. et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 92, 205–216 (2000).
Lencioni, R. & Llovet, J. M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis 30, 52–60 (2010).
Salem, R., Miller, F. H., Yaghmai, V. & Lewandowski, R. J. Response assessment methodologies in hepatocellular carcinoma: complexities in the era of local and systemic treatments. J Hepatol 58, 1260–1262 (2013).
Liu, L. et al. EASL- and mRECIST-evaluated responses to combination therapy of sorafenib with transarterial chemoembolization predict survival in patients with hepatocellular carcinoma. Clin Cancer Res 20, 1623–1631 (2014).
Nomura, F., Ohnishi, K. & Tanabe, Y. Clinical features and prognosis of hepatocellular carcinoma with reference to serum alpha-fetoprotein levels. Analysis of 606 patients. Cancer 64, 1700–1707 (1989).
Daniele, B., Bencivenga, A., Megna, A. S. & Tinessa, V. Alpha-fetoprotein and ultrasonography screening for hepatocellular carcinoma. Gastroenterology 127, S108–112 (2004).
Riaz, A. et al. Alpha-fetoprotein response after locoregional therapy for hepatocellular carcinoma: oncologic marker of radiologic response, progression and survival. J Clin Oncol 27, 5734–5742 (2009).
Chan, S. L. et al. New utility of an old marker: serial alpha-fetoprotein measurement in predicting radiologic response and survival of patients with hepatocellular carcinoma undergoing systemic chemotherapy. J Clin Oncol 27, 446–452 (2009).
Bruix, J. & Sherman, M. Management of hepatocellular carcinoma: an update. Hepatology 53, 1020–1022 (2011).
Gillmore, R. et al. EASL and mRECIST responses are independent prognostic factors for survival in hepatocellular cancer patients treated with transarterial embolization. J Hepatol 55, 1309–1316 (2011).
Kamath, P. S. et al. A model to predict survival in patients with end-stage liver disease. Hepatology 33, 464–470 (2001).
Kohles, N. et al. Prognostic relevance of oncological serum biomarkers in liver cancer patients undergoing transarterial chemoembolization therapy. Tumour Biol 33, 33–40 (2012).
McIntire, K. R., Vogel, C. L., Primack, A., Waldmann, T. A. & Kyalwazi, S. K. Effect of surgical and chemotherapeutic treatment on alpha-fetoprotein levels in patients with hepatocellular carcinoma. Cancer 37, 677–683 (1976).
Tsai, M. C. et al. Favorable alpha-fetoprotein decrease as a prognostic surrogate in patients with hepatocellular carcinoma after radiofrequency ablation. J Gastroenterol hepatol 25, 605–612 (2010).
Personeni, N. et al. Usefulness of alpha-fetoprotein response in patients treated with sorafenib for advanced hepatocellular carcinoma. J Hepatol 57, 101–107 (2012).
Xu, X. S. et al. Highlights for alpha-fetoprotein in determining prognosis and treatment monitoring for hepatocellular carcinoma. World journal of gastroenterology: WJG 18, 7242–7250 (2012).
Shim, J. H. et al. Which response criteria best help predict survival of patients with hepatocellular carcinoma following chemoembolization? A validation study of old and new models. Radiology 262, 708–718 (2012).
Riaz, A. et al. Radiologic-pathologic correlation of hepatocellular carcinoma treated with internal radiation using yttrium-90 microspheres. Hepatology 49, 1185–1193 (2009).
Riaz, A. et al. Radiologic-pathologic correlation of hepatocellular carcinoma treated with chemoembolization. Cardiovasc Intervent Radiol 33, 1143–1152 (2010).
Georgiades, C. et al. Lack of response after initial chemoembolization for hepatocellular carcinoma: does it predict failure of subsequent treatment? Radiology 265, 115–123 (2012).
Bloomer, J. R., Waldmann, T. A., McIntire, K. R. & Klatskin, G. alpha-fetoprotein in noneoplastic hepatic disorders. JAMA 233, 38–41 (1975).
Chen, C. H. et al. Hepatitis B- and C-related hepatocellular carcinomas yield different clinical features and prognosis. Eur J Cancer 42, 2524–2529 (2006).
Acknowledgements
This study was supported by grants from the National Natural Science Foundation of China 81172145 and 81420108020.
Author information
Authors and Affiliations
Contributions
Conceived and designed the study: Y.Z., J.J. and G.H.; collection and analysis of data: L.L., Y.Z., J.J., H.C., W.B., M.Y., J.X. and H.C.; manuscript writing: L.L., Y.Z., J.J., H.C., W.B., M.Y., Z.Y., C.H., L.Z., W.G., J.N., J.Y., H.C. and J.X.; revision of the manuscript: Y.Z., G.H. and D.F.; L.L., Y.Z., J.J., H.C., W.B., M.Y., Z.Y., C.H., L.Z., W.G., J.N., J.Y., H.C., J.X., D.F. and G.H.H. approved the final manuscript submitted.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Liu, L., Zhao, Y., Jia, J. et al. The Prognostic Value of Alpha-Fetoprotein Response for Advanced-Stage Hepatocellular Carcinoma Treated with Sorafenib Combined with Transarterial Chemoembolization. Sci Rep 6, 19851 (2016). https://doi.org/10.1038/srep19851
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep19851
This article is cited by
-
An Insight Into the Role of Alpha-Fetoprotein (AFP) in the Development and Progression of Hepatocellular Carcinoma
Molecular Biotechnology (2023)
-
Prognostic role of alpha-fetoprotein in patients with hepatocellular carcinoma treated with repeat transarterial chemoembolisation
BMC Cancer (2020)
-
Alpha-fetoprotein assessment for hepatocellular carcinoma after transarterial chemoembolization
Abdominal Radiology (2019)
-
Alpha-fetoprotein kinetics in patients with hepatocellular carcinoma receiving ramucirumab or placebo: an analysis of the phase 3 REACH study
British Journal of Cancer (2018)
-
Evaluation on the diagnostic and prognostic values of long non-coding RNA BLACAT1 in common types of human cancer
Molecular Cancer (2017)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
