
Abstract
Human population movements currently challenge malaria elimination in low transmission foci in the Greater Mekong Subregion. Using a mixed-methods design, combining ethnography (n = 410 interviews), malariometric data (n = 4996) and population surveys (n = 824 indigenous populations; n = 704 Khmer migrants) malaria vulnerability among different types of mobile populations was researched in the remote province of Ratanakiri, Cambodia. Different structural types of human mobility were identified, showing differential risk and vulnerability. Among local indigenous populations, access to malaria testing and treatment through the VMW-system and LLIN coverage was high but control strategies failed to account for forest farmers’ prolonged stays at forest farms/fields (61% during rainy season), increasing their exposure (p = 0.002). The Khmer migrants, with low acquired immunity, active on plantations and mines, represented a fundamentally different group not reached by LLIN-distribution campaigns since they were largely unregistered (79%) and unaware of the local VMW-system (95%) due to poor social integration. Khmer migrants therefore require control strategies including active detection, registration and immediate access to malaria prevention and control tools from which they are currently excluded. In conclusion, different types of mobility require different malaria elimination strategies. Targeting mobility without an in-depth understanding of malaria risk in each group challenges further progress towards elimination.
Similar content being viewed by others

Introduction
Despite increasing understanding of the importance of ‘hot spots’ for malaria control and elimination1, comparatively less attention is being given to populations subgroups (‘hot pops’) that are vulnerable to malaria but cannot be easily located in a geographically confined area due to their mobility2. While human mobility has been addressed more extensively in relation to neglected tropical disease elimination3, immunization campaigns4 and HIV prevention5, it has, until recently, been largely neglected in malaria control and elimination3,6,7. Nevertheless, human mobility affects malaria transmission in several ways. Population movements expose individuals to a variety of health hazards to which sedentary populations are not exposed8 and it is often harder for those individuals to cope with the consequences of disease due, for instance, to language difficulties or a lack of familiarity with local health care. Moreover, the type of work highly mobile populations perform and the generally poorer working conditions can result in higher exposure to malaria vectors6,9,10, as has been reported on rubber plantations or in slash-and burn-agriculture11,12. Population movements may also result in non-immune individuals arriving in endemic areas or infected individuals seeking care in malaria-free regions, increasing difficulties in diagnostics and treatment13,14,15,16,17,18.
The importance of human mobility for malaria elimination was evident in previous elimination attempts where malaria re-emerged due to surveillance systems that failed to account for the movements of human populations16,19. Standard malaria control interventions implicitly operate on the assumption that individuals and subpopulations are registered and therefore easy to access. Current malaria control efforts typically target geographically stable groups: village malaria workers are assigned to highly endemic villages based on the administrative unit of the village/community; the distribution of long lasting insecticidal nets (LLIN) relies on intermittently updated census data and also indoor residual spraying (IRS) focuses on stable administrative villages; all of which consequently fail to account for mobile populations10,17,20,21. Moreover, in biomedical and clinical research, mobile individuals and mobile ethnic groups (such as e.g. nomadic Fula herders in SSA) are often purposefully excluded so as to minimize poor compliance to treatment or losses to follow-up. As a result, little is known about the effectiveness of standard interventions among these mobile populations. In the context of current malaria elimination targets, human mobility represents a major challenge for national control programs to further decrease malaria transmission9,10,19. Given the large sociocultural differences between various types of mobile populations, it can be expected that there is no standard way to address mobility in malaria control. In this sense, targeting pastoral nomads (i.e. pastoral herders in SSA) will require a radically different approach as compared to targeting national or international migrants, or commercial itinerant workers (i.e. street vendors and traders in border regions).
Several countries in the Greater Mekong Subregion are aiming to achieve malaria elimination within the next few decades22. However, residual transmission foci persist in forested areas such as the North-Eastern Cambodian province of Ratanakiri, that are largely populated by ethnic minority communities, often located at international borders and on the fringes of society, with increasing rural to rural migration to exploit new economic opportunities such as rubber plantations, gem mining and agriculture23. The aim of this study was therefore to characterize the different mobile groups in one such context and related those to vulnerability to malaria.
Methods
Study site and population
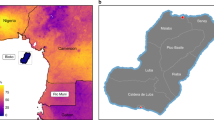
The study was conducted in the Cambodian province of Ratanakiri, traditionally populated by indigenous groups such as the Jarai, Kreung and Tompuon, also referred to as ‘ethnic minorities’, in contrast to the majority Khmer population that populates the rest of Cambodia. Indigenous subsistence strategies usually combine slash-and-burn agriculture with hunting, fishing, gathering forest products and small-scale trade. As distances between forest farms, rice fields and villages can be substantial (i.e. at several hours walking distance), most families maintain residences at each location and rotate from one place to another according to the agricultural cycle24. In addition to the indigenous populations, the rich resources of the province (forest, farmland, gems, etc.) have recently attracted many national and international investors mainly for large-scale rubber plantations. The latter require a large work force of mainly migrant workers from Cambodia’s rural and impoverished lowland provinces. In addition to plantation work, these rural-to-rural migrant Khmer farmers also seek irregular job opportunities on private farms or in construction and gem or gold mining in the area.
Malaria incidence in Ratanakiri is currently decreasing following intensified control measures, improved access to health care, socio-economic development and changes in the landscape, characterized by the replacement of the primary forests with rubber plantations, potentially impacting on vector populations25. Malaria transmission in Ratanakiri is perennial with two peaks, June-July and October-November and the main vector is Anopheles dirus25,26.
In the public sector, malaria control measures (LLIN distribution, early diagnosis with RDT and treatment) are implemented through village malaria workers (VMWs) at community level. At the time of the study (2008–2012), the first line treatment was mefloquine-artesunate (A + M) for Plasmodium falciparum and chloroquine for P. vivax. In the private sector, Malarine™ branded blisterpacks of mefloquine-artesunate were sold alongside various drug cocktails (small plastic bags containing a variety of drugs such as antimalarials and antibiotics) and artemether injections27. Local indigenous groups traditionally consult diviners (traditional healers) to identify the cause of an illness, often in combination with various treatments from the public or private sectors27.
Research strategy
A parallel mixed-methods study design was chosen, using qualitative ethnographic research and quantitative survey research methods for complementarity (in standard annotation [qual + quan]28). Qualitative ethnographic data were collected in local communities and selected plantations to acquire an in-depth understanding of mobility patterns, living and working conditions, access to and use of malaria preventive measures and health care services of (i) Khmer migrant plantation workers and gem miners and (ii) local indigenous populations. Three additional surveys were aimed at quantifying the ethnographically assessed variables among these different populations. The ethnographic study and three surveys are described below and summarized in Table 1 and Fig. 1.

Flowchart of research strategy.
Qualitative ethnographic study
The qualitative study was carried out in two phases: (i) A first exploratory qualitative phase was carried out between 2008 and 2010 in the villages of Phi and Lom (Oyado district), inhabited by the indigenous Jarai and in three adjacent rubber plantations; (ii) In 2012, in-depth qualitative research was conducted in three villages included in a larger cluster randomized trial on the effectiveness of topical repellents as an added control measure to long-lasting insecticidal nets25 (NCT01663831, hereafter “MalaResT”). The Tompuon villages of Kachon Kraom (Voen Sai district) and Sayos (Lumphat district) and the Jarai village of Lom (Oyadao district) were selected. In addition, in Borkeo, Oyadao and Andong Meas districts, all identifiable plantations and gem mining sites were visited.
Data collection
Participant observation and in-depth interviewing were carried out. The former consisted of observations and reiterated informal conversations. Participant observation was primarily used as respondent-independent data collection tool to detect unforeseen variables and to contrast stated opinions with actual behavior.
Sampling
Multiple purposive sampling techniques were used. Following the principle of gradual selection, informants were theoretically selected (in accordance with emerging results/theory) and categorized in relation to relevant criteria (such as gender, age, locality, forest activities, previous experience with malaria, use of preventive measures, etc)29. In order to increase confidentiality with respondents and consequent reliability of the data, snowball sampling techniques (i.e. sampling using participants to identify additional cases) were used.
Data analysis
Qualitative data collection and analysis were performed concurrently and data analysis was an iterative process. Preliminary data were intermittently analyzed in the field and preliminary results were then translated into the question guides for follow-up interviews. Analytic induction involved the iterative testing of theoretical ideas, which was used to refine and categorize themes grounded in the data29. This resulted in an analytical framework that was then systematically applied in the data analysis. Data were entered, managed and analyzed in NVivo 9 Qualitative Data Analysis software (QSR International Pty Ltd. Cardigan UK).
Khmer Migrant Survey
Three different risk groups –identified in the ethnographic study- were targeted: (i) rural to rural migrants working on rubber plantations; (ii) rural to rural migrants working in self-exploited (gold/gem) mines; and (iii) migrants having initially worked in plantations, but currently working in other informal jobs within the same general location (i.e. working on fields, etc). All work sites with migrant mobile populations in the districts of Oyadao, Andong Meas and Borkeo were identified and included in the study.
Data collection and sampling
In each study site, all Khmer working households (HH) that could be located on the plantation were invited to participate in the survey. After oral consent, first all participating household leaders were asked questions about their expected duration of residence, land ownership, administrative registration, income and use and access to malaria prevention tools. Secondly, the sleeping arrangements (use, type and condition of bed net or hammock net, sleeping surface) of all members of each household were observed and recorded.
Data analysis
Data was entered in Epi Info 7 (CDC, Atlanta, GA, USA) and analysed in SPSS (IBM SPSS Statistics 19). Frequency tables for the main descriptive variables were produced.
Indigenous Population Survey
Data collection and sampling
A random sample of 900 individuals from different households were selected from the population census of the 113 villages included in the MalaResT study in 2012 and invited to participate in the survey. After oral consent, all participants were interviewed on the number of different settlements accessed by the individual’s household (village homes, homes on slash and burn farms, homes on rice fields), the time spent in each location by household members and their use of malaria prevention measures.
Data analysis
Data was entered in Epi Info 7 (CDC, Atlanta, GA, USA) and analyzed in SPSS (IBM SPSS Statistics 19). Descriptive statistics were performed for the main outcome variables.
Indigenous Malariometric Survey
Data collection and sampling
In addition to the Indigenous Population Survey, a malariometric survey was conducted during the MalaResT study in October 2012 to determine malaria prevalence and related risk factors. A total of 6,640 individuals across the 113 study villages were randomly selected from the census file and invited to participate in the survey. Participants were interviewed on use of preventive measures and overnight stays at the farm plot hut, clinically examined and blood sampled for microscopy and molecular detection of malaria parasites25,26.
Data analysis
Data was entered in MS Access and analyzed in SPSS (IBM SPSS Statistics 19) and R (R version 3.1.1, The R Foundation for Statistical Computing). Frequency tables for the main outcome variables were produced. Two-level logistic regression with a random intercept fitted to adjust for clustering at village level was used to calculate the odds ratio for the association between spending nights in the forest in the past month and malaria infection, adjusted for age and sex.
Ethical considerations
The study protocol was approved by the Institutional Review Board of the Institute of Tropical Medicine in Antwerp (ITM) and the Ministry of Health, Cambodia. The interviewers followed the Code of Ethics of the American Anthropological Association (AAA). All interviewees were informed before the start of the interview about project goals, the topic and type of questions, the intended use of results for scientific publications as well as their right to refuse being interviewed, interrupt the conversation at any time or withdraw any given information during or after the interview. Anonymity was guaranteed and confidentiality of interviewees assured by assigning a unique code number to each informant. The interviewers sought oral consent from all interviewees. Oral consent was preferred because the act of signing one’s name when providing certain information can generate mistrust. The quantitative and malariometric surveys obtained additional ethical clearance from ethical committee of the University Hospital of Antwerp and the National Ethics Committee for Health Research in Cambodia. For the surveys, the study objectives and methodology were first explained to each family in Khmer and individual written informed consent was given by each participant, or by parents/guardians of children below 18 years of age. All methods were carried out in accordance with the approved guidelines
Results
Study participants
Qualitative study
In total, 410 interviews, including formal and informal conversations, were recorded and transcribed.
Indigenous Population Survey
Among the 900 randomly sampled individuals, 824 (91.6%) were reached and interviewed, among which 55 individuals were Khmer (6.7%) that had migrated to a local village. All other respondents were indigenous people, including the ethnicities Jarai, Kreung, Tompuon, Kachok, Kavet, Lao, Lon and Prov.
Khmer Migrant Survey
Among the 67 plantations and 2 gem-mining sites included in the survey, 186 Khmer household leaders were interviewed. Of these 186 households, 704 household members’ sleeping arrangements were recorded.
Indigenous Malariometric Survey
Among the 6,640 individuals selected from the census file, 4,996 (75%) participants were reached.
Types of mobility
During the first phase of the ethnographic study, the following types of mobile groups were identified (Table 1): first, Khmer rural-to-rural migrants, including (i) Permanent national rural to rural migration, which describes Khmer farmers leaving their rural communities in lowland provinces of Cambodia to settle permanently in highland Ratanakiri and work on large-scale plantations or smaller farms; and (ii) Seasonal/temporal national rural to rural migration, referring to Khmer farmers temporarily working on plantations in Ratanakiri and then returning to their villages at the end of their contract. Secondly, indigenous population movements were identified that included mobility due to (iii) indigenous multiple residence systems. This translates into local indigenous population movements driven by subsistence requirements (e.g. sleeping at farms in the forest) and economic activities (e.g. spending nights in the forest for hunting). Indigenous population movement also included (iv) cross-border mobility, meaning movement of indigenous people across the Cambodian/Vietnamese border for economic (buying or selling products across the border) and/or social (visiting relatives) reasons.
Vulnerability of Khmer rural to rural migrants to malaria infection
Mobility
More than half (56.5%) of the Khmer households working on plantations, all households working in gem-mining sites and most households (70.6%) headed by independently working Khmer migrants were categorized as “permanent rural to rural migration”, reportedly having come to Ratanakiri to work for an indefinite period of time (Table 2). Among the Khmer plantation workers, 43.5% could be categorized as seasonal rural to rural migrants, with a median working time of 5 months (IQR 16, range 1 to 108 months); a figure that went up to 48 months among miners (IQR 54, range 1 to 240 months). Traditionally, the Khmer New Year (April) marked the time point at which the Khmer migrant plantation workers returned home and new migrants came to replace them.
Socio-economic vulnerability
Overall, only 7.0% of all Khmer migrant households owned some land for small subsistence farming in Ratanakiri, while the majority did not own land at all (53.2%), especially among the miners (83.8%). Miners also seldom owned land in their home province (8.1%) compared to plantation or other workers (respectively, 52.2% and 38.2%; Table 2). On plantations, the majority of Khmer workers (79.1%) were not officially registered in Ratanakiri; though most of them (84.6%) reported being registered in their home villages. Local official registration was higher among Khmer migrants working independently on private farms (55.9%) and on mining sites (67.6%). The Khmer migrant households’ monthly income ranged between 0 and 800.000 riel (200 USD) with a median of 250.000 riel (62.5 USD) (Table 2). and half of households reported not being able to save any of this money.
Access to health care and malaria prevention
Only 5.4% of Khmer migrant respondents knew about the existence of VMW’s in the nearby indigenous villages, (Table 2); and only 2.7% knew the actual VMW of the village where their plantation/mine was located. The lack of administrative registration among the majority of Khmer migrants resulted in the majority of households never having received a bed net from the NMCP in Ratanakiri (66.7%), especially those households working on plantations (91.3%). Moreover, a majority (76.3%) of Khmer migrants reported never having received a bed net from the NMCP in their home province. Nevertheless, the majority of the households did bring bed nets (both treated and non-treated) to their new work locations (89.2%) and most of them considered the number of bed nets they brought themselves sufficient to protect all household members (71.7%) (Table 2).
When considering individual malaria prevention among household members of the migrant households, almost all (91.1%) respondents reported to use a bed net, usually while sleeping on mats, or on rare occasions, in hammocks (Table 3). Bednets were usually non-treated and bought from the market (74.7%) and over half of the respondents were sleeping under nets that were observed to be torn (i.e. defined as nets with rips and tears).
Indigenous population in-country mobility
Mobility
Mobility among the indigenous population is linked to the tradition of slash-and-burn agriculture. According to the ethnographic study, indigenous families combine sleeping in village homes (traditionally longhouses) with one or several homes at their farms or rice fields in the forest. According to the Indigenous Population Survey (Table 4), most respondents (93.2%) had one or more forest farms, as well as a house on the farm(s) (82.5%). The rainy season, especially during the harvest months, is the most work intensive season for indigenous farmers, often requiring them to sleep in plot huts at their farms in the forest. Indeed, 61.2% reported sleeping at their farms during the malaria season (rainy season which extends into harvest months). In addition to forest farms, 44.1% of respondents reported having a wet rice field and of those, the majority (67.5%) had built a house on that rice field where they would also be sleeping during the malaria season (53.2%).
The village home is mostly used during the dry season when the most labor-intensive work at the field is over and when farmers rest and have their annual ceremonies and celebrations in the village home. Accordingly, only 33.1% of all respondents reported always sleeping in the village during the rainy season, as opposed to the 72.5% that always sleep in the village during the dry season.
Forest farms are usually reached by foot and can be located as far as 10 kilometers from the village, making it difficult to transport the necessary materials, such as food, water, mats and bed nets, back and forth between village and farm (Table 4). The majority (74.8%) of respondents reported moving between farms and fields without stopping over in the village, making it even more difficult to carry around sufficient bed nets or hammock nets to protect all family members who go on the journey. However, due to the recent national malaria control policy (since 2011) of distributing one bed net per person, the largely officially registered indigenous families seem to have sufficient bed nets from the NMCP in combination with non-impregnated nets bought from the market to spread them out over several locations, as multiple family members sleep under one net at different sleeping places. Over half of respondents therefore report to permanently keep some bed nets at their farms (58.1%) and rice fields (50.6%) and the majority reports to usually have a bed net to use at farms (73.3%) and rice fields (77.6%) (Table 4).
Deep forest activities
67.2% of the indigenous population engaged in deep forest activities. These consist of hunting, gathering forest products such as bamboo or wood and other activities in the uncleared forest where people potentially sleep in an improvised way (e.g. in hammocks). 23.6% reported spending nights in the deep forest (Table 4). The malariometric survey indicated a significant relationship between spending nights at the plot hut on the forest farm in the last month and increased odds of malaria infection (OR 1.66, 95% CI 1.20-2.28, p = 0.002). There was a trend towards increased odds of malaria associated with spending nights in the deep forest in the last month, though there was only weak statistical evidence for this association (OR 1.35, 95% CI 0.94-1.98, p = 0.10) (Table 5).
Access to health care and malaria prevention
Unlike the Khmer migrants, most local indigenous villagers knew the local VMW since he/she was chosen from the indigenous community; only 22.8% of indigenous respondents had never visited the VMW (Table 4). Of those who had visited the VMW for a RDT, 71.5% reported the test to have been positive for malaria and most of those positive cases (81.6%) received treatment from the VMW.
Indigenous population cross-border mobility
Mobility
According to the ethnographic study, in the three Jarai villages at the border area, the indigenous territory consists of communities spread over both sides of the border. Short-term cross-border human population movements occurred frequently as the Vietnamese and Cambodian Jarai living within the border communes are allowed to cross the border without permits for one-day stays. It was primarily Cambodian Jarai that crossed the border into Vietnam to pursue economic activities, namely to sell agricultural products and/or to buy products at local Vietnamese stores and markets to take back to Cambodia for resale in small privately owned shops. Longer stays, for which community-level permits and justifications are needed, were generally driven by wanting to seek care in Vietnamese health centers (also for malaria treatment), to visit relatives and to attend ceremonies. Given the greater economic growth in Vietnam, few Vietnamese Jarai venture into Cambodia for business, but do cross the border for celebrations and other family obligations, as well as to cultivate land in the forest for slash and burn agriculture unavailable in Vietnam.
Malaria prevention
When visiting relatives or other relations across the border, it is not usual to take bed nets when spending nights at hosts’ houses across the border. The host family often do not have enough nets to share and rules of hospitality do not require the host to provide bed nets to visitors. However, families that visit once or twice a year and only for ceremonies do so mostly during the dry season.
Discussion
Our study characterized the different structural types of human mobility in Ratanakiri and their differential risk and vulnerability towards malaria exposure, clearly showing the need for different and adapted malaria prevention and control measures among the groups that are, nevertheless, usually jointly categorized under “mobile populations”. Among the local indigenous population, in contrast to the Khmer migrants, LLIN coverage was very high. However, this LLIN distribution was based solely on the administrative village setting, thereby failing to take into account local forest farmers’ multiple residence system which entails prolonged stays in the forest farms/fields and increases their exposure to the known early outdoor biting behavior of sylvatic An. dirus12,21. Control measures targeting the forest farms, such as additional LLINs and/or other innovative tools, such as spatial repellents or toxic sugar bait traps, can be expected to have a further impact on malaria30,31. Types of human population movements, taking place on a relatively local level, easily go undetected, as illustrated by the multiple residence system among the indigenous Jarai. They could, however, be key to malaria elimination due to the mentioned exposure and in relation to difficulties with uptake of elimination strategies such as MDA, where these populations may easily be missed. More irregular and individual mobility related to the family visits, trade, the exploitation of forest products, including logging, require different tools and strategies, examples of which could be long-lasting insecticidal hammocks32,33,34,35,36, topical repellents or insecticide treated clothing37,38.
With regard to cross-border mobility, while the current borders of the nation-states divide traditional indigenous territory, their social and economic networks require cross-border movements. These cross-border movements can increase local populations’ vulnerability to malaria as no bed nets are transported during these visits and hosts generally do not offer them to their guests. In addition, the differential application, in method and intensity, of malaria control activities on either side of nations’ borders has been shown to potentially lead to the maintenance of the parasite reservoir by a constant supply of new strains39.
Additional difficulties for malaria control among indigenous populations include language barriers, historically complicated inter-ethnic relations, the power imbalance observed between local communities and large companies that are currently converting traditional territories into plantations. All of these factors can be hypothesized to compel the most vulnerable groups among indigenous populations, in terms of socio-economic status and social integration, to retreat deeper into remote forested areas, further increasing their exposure/risk and decreasing their accessibility to health services.
The Khmer rural-to-rural migrant group, mostly active on rubber plantations and in mines, represents a fundamentally different social group that increasingly develops as a parallel “social territory” to that of the indigenous populations. The continuous influx of these lowland Khmer constitutes a new potential risk group for malaria. These migrants are often moving from lowland non-endemic provinces and are therefore more vulnerable to malaria infection due to their limited awareness of malaria prevention and treatment as well as low acquired immunity, in contrast to the indigenous populations, that have good access to malaria diagnostic and treatment through the VMW system and have a higher level of immunity. Khmer migrants were seldom reached by LLIN-distribution campaigns since they remained largely unregistered and were also unaware of the local VMW-system due to poor social integration locally. Moreover, most plantation workers and miners purchased non-treated nets, the majority of which were already damaged at the time of study, providing less protection against mosquito bites.
The temporal migration from high to low-endemic areas, as large numbers of Khmer migrants return to their home provinces after their work has ended, can result in imported infections16 or re-introduce malaria where transmission had ceased, which is especially the case in areas of high receptivity (i.e. the historical potential for vector transmission that determines the severity of local onward transmission)16. Khmer temporal migrants therefore require different malaria control strategies than local indigenous populations, such as the active detection and registration of those workers and immediate access to malaria prevention and control tools from which they are currently excluded.
The strength of this study lies in its mixed-methods design that allowed the integration of qualitative and quantitative data, producing consistent and complementary findings across different datasets. The triangulation design reduced the risk of bias as it allows the validation of different findings observed across different methods. An additional strength was the interdisciplinarity, which enabled linking different types of local mobility patterns to malaria risk as measured by malariometric data. The ethnographic data collection provided richer contextual data than would have been possible to obtain through standard questionnaires during malariometric surveys. Furthermore, the ethnographic component explicitly informed the development of the malariometric survey by a prior identification of all possible local risk factors/behaviors. The main limitation of the study was the lack of malariometric data on migrant workers in rubber plantations and gem mines that could have assessed the relevance of their exposure in relation to malaria risk. This should be further assessed in population-based studies including the different groups at risk. In addition, due to the rapid economic changes in the region and the continuous exploitation of new plantations, some plantations may have been missed. We do not expect, however, that including additional plantations would have changed the presented results.
Conclusion
Different types of mobility require different malaria control and, ultimately, elimination strategies (Fig. 2). In addition, targeting mobility without an in-depth understanding of malaria risk in each group can lead to wasted efforts and resources. Further studies should be systematically embedded into national malaria control and elimination programs in order to identify the different type(s) of mobile populations at stake and enable the development of a theoretical framework for optimizing the delivery of effective malaria control measures to those most in need.

Malaria vulnerability by types of mobility.
Additional Information
How to cite this article: Peeters Grietens, K. et al. Characterizing Types of Human Mobility to Inform Differential and Targeted Malaria Elimination Strategies in Northeast Cambodia. Sci. Rep. 5, 16837; doi: 10.1038/srep16837 (2015).
References
Bousema, T. et al. Hitting hotspots: spatial targeting of malaria for control and elimination. PLoS Med. 9, e1001165, 10.1371/journal.pmed (2012).
Cotter, C. et al. The changing epidemiology of malaria elimination: new strategies for new challenges. The Lancet 382, 900–911, 10.1016/S0140-6736(13)60310-4 (2013).
Stoddard, S. T. et al. The role of human movement in the transmission of vector-borne pathogens. PLoS NTDs 3, e481, 10.1371/journal.pntd.0000481 (2009).
Schelling, E. et al. Human and animal vaccination delivery to remote nomadic families, Chad. Emerging infectious diseases 13, 373 (2007).
Todrys, K. W. & Amon, J. J. Within but without: human rights and access to HIV prevention and treatment for internal migrants. Globalization and health 5, 17, 10.1186/1744-8603-5-17 (2009).
Prothero, R. M. Population mobility and trypanosomiasis in Africa. Bulletin of the World Health Organization 28, 615 (1963).
Smith, C. & Whittaker, M. Beyond mobile populations: a critical review of the literature on malaria and population mobility and suggestions for future directions. Malar. J. 13, 10.1186, 10.1186/1475-2875-13-307 (2014).
Prothero, R. M. Disease and mobility: a neglected factor in epidemiology. International journal of epidemiology 6, 259–267 (1977).
Heggenhougen, H., Hackethal, V. & Vivek, P. The behavioural and social aspects of malaria and its control: An introduction and annotated bibliography. (UNDP/World Bank/WHO/TDR, 2007).
Carpenter, C. C., Pearson, G. W., Mitchell, V. S. & Oaks Jr, S. C. Malaria: Obstacles and Opportunities (National Academies Press, 1991).
Peeters Grietens, K. et al. Low perception of malaria risk among the Ra-glai ethnic minority in south-central Vietnam: implications for forest malaria control. Malar. J. 9, 1–9, 10.1186/1475-2875-9-23 (2010).
Erhart, A. et al. Forest malaria in Vietnam: a challenge for control. Am. J. Trop. Med. Hyg. 70, 110–118 (2004).
Deressa, W., Ali, A. & Berhane, Y. Review of the interplay between population dynamics and malaria transmission in Ethiopia. Ethiopian Journal of Health Development 20 (2006).
Hu, H. et al. Factors influencing malaria endemicity in Yunnan Province, PR China (analysis of spatial pattern by GIS). Southeast Asian J. Trop. Med. Public Health 29, 191–200 (1998).
Jianwei, X. & Hui, L. Border malaria in Yunnan, China. Southeast Asian Journal of Trop. Med. & Public Health 28, 456–459 (1997).
Pindolia, D. K. et al. The demographics of human and malaria movement and migration patterns in East Africa. Malar. J. 12, 10.1186, 10.1186/1475-2875-12-397 (2013).
Wessen, A. F. Human ecology and malaria. Am. J. Trop. Med. Hyg. 21, 658–662 (1972).
Wesolowski, A. et al. Quantifying the impact of human mobility on malaria. Science 338, 267–270 (2012).
Martens, P. & Hall, L. Malaria on the move: human population movement and malaria transmission. Emerg. infect. dis. 6, 103 (2000).
Wangroongsarb, P. et al. Respondent-driven sampling on the Thailand-Cambodia border. II. Knowledge, perception, practice and treatment-seeking behaviour of migrants in malaria endemic zones. Malar. J. 10, 10.1186, 10.1186/1475-2875-10-117 (2011).
Peeters Grietens, K. et al. Social Determinants of Long Lasting Insecticidal Hammock-Use Among the Ra-Glai Ethnic Minority in Vietnam: Implications for Forest Malaria Control. PloS ONE 7, e29991, 10.1371/journal.pone.0029991 (2012).
Cui, L. et al. Challenges and prospects for malaria elimination in the Greater Mekong Subregion. Acta Tropica 121, 240–245 (2012).
Cui, L. et al. Malaria in the Greater Mekong Subregion: Heterogeneity and complexity. Acta Tropica 121, 227–239 (2012).
Gryseels, C. et al. Re-imagining Malaria: Heterogeneity of Human and Mosquito Behavior in Relation to Residual Malaria Transmission in Cambodia. Malar. J. 14, 165, 10.1186/s12936-015-0689-0 (2015).
Sluydts, V. et al. Spatial clustering and risk factors of malaria infections in Ratanakiri Province, Cambodia. Malar. J. 13, 387, 10.1186/1475-2875-13-387 (2014).
Canier, L. et al. An innovative tool for moving malaria PCR detection of parasite reservoir into the field. Malar. J. 12, 405, 10.1186/1475-2875-12-405 (2013).
Gryseels, C. et al. Injections, cocktails and diviners: therapeutic flexibility in the context of malaria elimination and drug resistance in Northeast Cambodia. PloS ONE 8, e80343. 10.1371/journal.pone.0080343 (2013).
Teddlie, C. & Tashakkori, A. Foundations of mixed methods research: Integrating quantitative and qualitative approaches in the social and behavioral sciences (Sage, 2009).
Bernard, H. R. Research methods in anthropology: Qualitative and quantitative approaches (Rowman, 2011).
Durnez, L. & Coosemans, M. Residual transmission of malaria: an old issue for new approaches in Anopheles mosquitoes–New insights into malaria vectors (ed. Manguin S. ) 671–704 (2013).
Durnez, L. et al. Outdoor malaria transmission in forested villages of Cambodia. Malar. J. 12, 329, 10.1186/1475-2875-12-329 (2013). 10.5772/55925.
Hill, N., Lenglet, A., Arnez, A. & Carneiro, I. Plant based insect repellent and insecticide treated bed nets to protect against malaria in areas of early evening biting vectors: double blind randomised placebo controlled clinical trial in the Bolivian Amazon. BMJ 335, 1023 (2007).
Syafruddin, D. et al. Impact of a Spatial Repellent on Malaria Incidence in Two Villages in Sumba, Indonesia. Am. J. Trop. Med. Hyg. 91, 1079–1087 (2014).
Muller, G. et al. Successful field trial of attractive toxic sugar bait (ATSB) plant-spraying methods against malaria vectors in the Anopheles gambiae complex in Mali, West Africa. Malar. J. 9, 210, 10.1186/1475-2875-9-210 (2010).
Kimani, E. W., Vulule, J. M., Kuria, I. W. & Mugisha, F. Use of insecticide-treated clothes for personal protection against malaria: a community trial. Malar. J 5, 63, 10.1186/1475-2875-5-63 (2006).
Thang, N. D. et al. Long-lasting insecticidal hammocks for controlling forest malaria: a community-based trial in a rural area of central Vietnam. PLoS ONE 4, e7369. 10.1371/journal.pone.0007369 (2009).
Killeen, G. et al. Made-to-measure malaria vector control strategies: rational design based on insecticide properties and coverage of blood resources for mosquitoes. Malar. J, 13, 146, 10.1186/1475-2875-13-146 (2014).
Wilson, A. L., Chen-Hussey, V., Logan, J. G. & Lindsay, S. W. Are topical insect repellents effective against malaria in endemic populations? A systematic review and meta-analysis. Malar. J. 13, 446, 10.1186/1475-2875-13-446 (2014).
Pongvongsa, T. et al. Joint malaria surveys lead towards improved cross-border cooperation between Savannakhet province, Laos and Quang Tri province Vietnam. Malar. J. 11, 262, 10.1186/1475-2875-11-262 (2012).
Acknowledgements
We are most grateful to all community members in the study region for their time and their confidence in our research. We also sincerely thank the staff of the provincial health department in Ratanakiri. This work was partly funded by the Bill and Melinda Gates foundation under the Global Health Grant number OPP1032354 and the Belgian Cooperation within the Framework Agreement III between the Institute of Tropical Medicine (ITM), Antwerp, Belgium and the National Center for Parasitology, Entomology and Malaria Control (CNM), Phnom Penh, Cambodia.
Author information
Authors and Affiliations
Contributions
K.P.G., A.E., U.D.A. and M.C. conceived of the study. K.P.G. and C.G. designed the experiments. K.P.G., C.G., S.U., P.P., S.S. and S.R.S. performed the anthropological fieldwork. V.S. performed and supervised the malariometric survey. K.P.G. and C.G. performed the qualitative data analysis. C.G., S.D. and V.S. did the quantitative analysis. K.P.G. and C.G. wrote the manuscript. A.E., M.C., U.D.A., S.H.M., R.G., J.M., M.B.T., S.H., S.D., S.T., S.U., P.P., S.S., S.R.S, L.D., V.S. and T.S. edited and reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Peeters Grietens, K., Gryseels, C., Dierickx, S. et al. Characterizing Types of Human Mobility to Inform Differential and Targeted Malaria Elimination Strategies in Northeast Cambodia. Sci Rep 5, 16837 (2015). https://doi.org/10.1038/srep16837
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep16837
This article is cited by
-
Comparing malaria risk exposure in rural Cambodia population using GPS tracking and questionnaires
Malaria Journal (2024)
-
Applying the COM-B behaviour change model to a pilot study delivering volatile pyrethroid spatial repellents and insecticide-treated clothing to forest-exposed populations in Mondulkiri Province, Cambodia
Malaria Journal (2023)
-
Forest malaria and prospects for anti-malarial chemoprophylaxis among forest goers: findings from a qualitative study in Thailand
Malaria Journal (2022)
-
Why using bed nets is a challenge among minority populations in Central Vietnam
Malaria Journal (2022)
-
Imported malaria definition and minimum data for surveillance
Scientific Reports (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
