
Abstract
The study aimed to examine the association between ideal cardiovascular health (CVH) metrics and depression. We conducted a population-based, cross-sectional study of 6,851 participants aged 20 years or older (3,525 men and 3,326 women) living in Tangshan City, China. Information on the seven CVH metrics (including smoking, body mass index, dietary intake, physical activity, blood pressure, total cholesterol and fasting blood glucose) was collected via questionnaires, physical examination and laboratory test. Depression status was assessed using the Epidemiologic Studies Depression Scale (CES-D) and a score of 16 or above was considered depression. The relationship between CVH metrics and depression was analyzed using logistic regression. Of the 6,851 participants, 525 (7.7%) were in depression status. After adjustment for potential confounders, men in the highest quartile of ideal CVH metric summary score had a reduced likelihood of having depression compared to those in the lowest quartile (adjusted odds ratio (AOR): 0.46, 95% confidence interval (CI): 0.28–0.75, p = 0.002). A similar trend was found among women, even though the association was not significant (AOR = 0.74, 95%CI: 0.46–1.18, p = 0.211). This study suggested that better CVH status is associated with a lower risk of depression especially in Chinese male and young population.
Similar content being viewed by others

Introduction
Depression is a significant contributor to the global burden of diseases, currently affecting an estimated 350 million people worldwide. Depression is more prevalent in developing countries than developed countries. Unipolar major depression is the second largest contributor to the burden of disease in mainland China, accounting for 6.2% of the total disease burden1. Moderate to severe depression is a serious condition and can lead to severe consequence including suicide2.
Depression is a physical and psychological illness. The disease if untreated can lead to fatal consequences such as heart attacks and cerebral vascular events3,4,5,6. The best strategy to control the depression is to understand the condition and apply lifestyle modifications7.
American Heart Association (AHA) proposed the concept of “ideal cardiovascular health” in 2010. This refers to the simultaneous existence of three health behaviors (non-smoking, being physically active and healthy dietary intake) and four health biomarkers (body mass index <25 kg/m2, untreated total cholesterol <200 mg/dl, untreated systolic/diastolic blood pressure <120/80 mmHg and fasting plasma glucose <100 mg/dl)8. The “zero-level prevention” concept emphasizes the importance of healthy behaviors on preventing cardiovascular diseases.
España-Romero et al. reported that ideal cardiovascular factors had protective effects on depression in Caucasian populations9. However, within Chinese population, the prevalence of ideal cardiovascular health indicators remains unclear and their relationships with depression have not been reported. We, therefore, conducted a cross-sectional study to explore the relationship between ideal cardiovascular metrics and depression in Chinese population.
Results
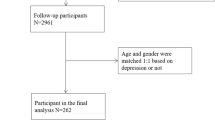
After excluding 13 participants aged less than 20 years and 246 persons with missing information on study exposures, outcomes or important confounders, the final analyses included 6,851 persons (3,525 men and 3,326 women). Overall, 525 (7.7%) participants had depressive symptoms. Table 1 shows the characteristics of participants with or without depression. The prevalence of depression among men was comparable to that among women (8.2% vs. 7.1%, p = 0.086). On average, participants with depression were younger and had lower income. Regarding CVH metrics, participants with non-ideal smoking status (9.6%), physically inactive (9.8%) and having unhealthy diet (12.3%) were more likely to be depressed. There was no correlation between body mass index (BMI), total cholesterol and depression.
Table 2 shows the association between depression and cardiovascular health metric. After adjusting for age, gender, marital status, alcohol use, income level, education, history of myocardial infarction, history of stroke and cancer and other six ideal cardiovascular metrics, we found that ideal smoking status, ideal physical activity and ideal diet intake significantly correlated with the a lower prevalence of depression (AOR = 0.78, 95%, CI: 0.61–0.99, P = 0.041; AOR = 0.67, 95% CI: 0.55–0.82, P < 0.001; and AOR = 0.43, 95% CI: 0.32–0.58, P < 0.001, respectively). In contrast, ideal blood pressure was associated with a higher prevalence of depression compared to those with a poor blood pressure (OR = 1.79, 95%, CI: 1.24–2.59, P = 0.001), but we found no significant association between BMI, total cholesterol, fasting blood glucose and depression.
Stratified analyses showed that the negative correlation of depression with ideal dietary intake and positive correlation with ideal blood pressure were consistent in men and women across different age groups. However, the negative association of depression with ideal smoking status and physical activity appeared to be more associated with men than women.
Table 3 shows the associations between depression and the summary score of ideal CVH metrics. After adjusting for potential confounders, we found that participants in the highest quartile of ideal CVH metrics summary score had a lower risk of getting depression than those in the lowest quartile of the summary score (AOR = 0.58, 95%CI: 0.43–0.78, p < 0.001). Stratified analyses showed that such negative association was more profound in men those whose age were below 40 years.
Discussion
Based on this large population-based sample, the study found that participants with better CVH metric measures had a lower risk of having depression. Those in the highest quartile of the ideal CVH metric summary score had a 42% reduced odds of having depression compared to those in the lowest quartile. This negative association was stronger in men and in participants younger than 40 years.
Our research showed that ideal metrics of smoking, physical activity and dietary intake had a negative association with depression. Other studies done outside China have also come to a similar conclusion9,10. A prospective study of 5,110 Americans found that the ideal cardiovascular health components, especially healthy behaviors, were negatively correlated with depressive symptoms9. Likewise, a study by Ia M.K et al. on 30,239 participants from the United States found that depression was associated with poor metrics of CVH10. Health behaviors may be crucial to prevent depression and can reduce the risk of developing cardiovascular diseases. The cardiovascular health behaviors including ideal diet intake, being physically active and non-smoking are associated with a reduced likelihood of having depression11,12,13. Our study confirmed the findings from previous studies that ideal diet intake is associated with a lower prevalence of depression. Several studies reported that being physically inactive is associated with depression, whereas regular physical exercise can be useful to relieve insomnia and depression and improve psychological health14,15,16. Our study confirmed this association, even though the association appeared stronger in men. In addition, studies showed that cigarette smoking might compromise the effectiveness of treatments for depression and increase the risk of developing depression17,18,19. Similar conclusion was found in our study, even though the association seems only present among men but not women (P > 0.05).
We analyzed the relationships between depression and the biomarkers indicative of ideal cardiovascular health. Previous research showed that there were negative correlation between the total cholesterol and depression20; however, our study disagreed with this finding. A prospective study of 5,110 Caucasian also found no significant correlation between total cholesterol and depression9. We did not find a correlation between fasting plasma glucose and depression, which was contrary to some previous studies4. There may be two possible explanations for this discrepancy. Firstly, our study may have failed to detect the association because too few participants had a poor measure of fasting blood glucose, with a proportion of 2.6% and 4.7% in participants with or without depression, respectively. Secondly, the difference may be due to ethnic difference among the participants. Participants in this study are Han-ethnic Chinese, probably having different physique and lifestyles compared with other ethnic populations.
In our study, participants with ideal blood pressure had a 79% increase in the odds of having depression compared to those with poor blood pressure. Earlier research considered low blood pressure ideal for health21, but more recent studies showed that low blood pressure was associated with various somatic and psychological symptoms22,23. A cross-sectional study of 60,799 participants showed that low blood pressure was associated with anxiety and depression24. In their study, hypotension was defined as the systolic/diastolic blood pressure less than 120/75 mmHg, which is close to the “ideal blood pressure level”. In this study, we found similar results especially in the male and young population. A study reported that neurons which controlled blood pressure by releasing neuropeptide Y may play a role in lowering blood pressure and inducing anxiety25.
Although our study included a large sample size and adjusted for a variety of potential confounders, several limitations should be noted. Firstly, dietary intake is defined based on questionnaire survey modified from the established food frequency questionnaire. Secondly, despite that the Center for Epidemiologic Studies Depression Scale is a validated scale and widely used for measuring depression in epidemiologic studies, the scale is not a tool for clinical diagnosis of depression. Thirdly, we do not have sufficient information on use of antidepressant medication and other treatments and thus are unable to adjust for them in the model. Fourthly, all participants in this study are from the Jidong community with relatively higher income status and attained higher education compared to the general Chinese population. Therefore, we cannot generalize our results for the entire Chinese population. Finally, this study is a cross-sectional study, which limits our ability to conclude a cause–effect relationship between ideal cardiovascular metrics and depression.
In conclusion, higher ideal cardiovascular metrics are associated with a lower prevalence of depression. Maintaining ideal cardiovascular health, i.e., non-smoking, physically active and healthy dietary intake may be of great value to prevent depression in the general population, especially among male and young Chinese population.
Methods
Ethics Statement
The study was conducted according to the guidelines of Helsinki Declaration and was approved by the Ethics Committee of Jidong Oilfield Inc. Medical Centers. Written informed consent was obtained from all participants.
Study Design and Population
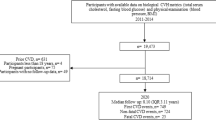
From July to November 2013, all residents aged 20 years and above from Jidong community were invited to participate in this study. The community is geographically located in Tangshan City, northern China and is mainly comprised of employees of the Jidong Oilfield Inc. and their family members. 7,110 residents (out of all the 9,500 residents) were willing to participate in the study and provided informed consent. Among the participants, 6,851 who had complete information on CVH metrics, depression and potential confounders were included in the analyses. At baseline, physical examinations and surveys were conducted by trained medical professionals from Medical Centers of the Jidong Oil field Inc.
Assessment of Cardiovascular Health Metrics
Dietary intake was assessed via a brief semi-quantitative food frequency questionnaire26,27. All participants were asked the amount and frequency of the consumption of ten major food groups/items during past 12 months: vegetable, fruits, fiber-rich whole grains, eggs, red meat (beef/lamb/pork), fish/sea food, milk and dairy products, soybean products, nuts, sugar-sweetened beverage and tea. Salt intake (gram per day) was based on self-report. Healthy dietary-intake components were defined as follows: 4.5 or more servings per day of fruits and vegetables; 2 or more servings per week of fish or shellfish; 3 or more servings per day of fiber-rich whole grains; sugary drinks once a week or less; and less than 6 gram per day of salt intake.
Body mass indexes (BMI) were defined based on measured heights (accurate to 0.1 cm) and weights (accurate to 0.1 kg) and calculated as the body weight (kg) divided by the square of height (m2). Blood pressure was measured using a mercury sphygmomanometer. Two readings of systolic blood pressure (SBP) and diastolic blood pressure (DBP) were taken at a five-minute interval with the participants resting in a chair during the interval. The average of the two readings was used for current analyses. If the two measurements differed by more than 5 mmHg, an additional reading was taken and the average of the three readings was used.
Blood samples were drawn by trained phlebotomists from the participants after overnight fasting. The venous blood samples in tubes containing trisodium ethylenediaminetetraacetic acid were immediately placed on ice after antecubital venipuncture. Blood samples were then centrifuged for 10 minutes at 3,000 rotations per minute at 25 °C. After separation, plasma samples were used within four hours. Biochemical variables including total cholesterol and fasting blood glucose were measured using an autoanalyzer (Olympus, AU400, Japan) at the central laboratory in Jidong Oilfield Hospital.
According to the guidelines by America Heart Association (AHA), we defined the seven CVH metrics in three levels: “ideal”, “intermediate” and “poor”8. Based on the number of healthy-diet behaviors, the dietary intake metric was classified as ideal (4–5 components), intermediate (2–3 components) or poor (0–1 component). Smoking metric was classified as ideal (never or quit-smoking >12 months); intermediate (former-smoking ≤12 months) or poor (current smoking); physical activity was classified as ideal (≥150 min/week of moderate intensity or ≥75 min/week of vigorous intensity), intermediate (1–149 min/week of moderate intensity or 1–74 min/week of vigorous intensity), or poor (none). BMI was classified as ideal (<25 kg/m2), intermediate (25–29.9 kg/m2) or poor (≥30 kg/m2); blood pressure was classified as ideal (SBP<120 mmHg and DBP <80 mmHg and untreated), intermediate (SBP 120–139 mmHg or DBP≥80–89 mmHg or treated to goal), or poor (SBP≥140 mmHg or DBP≥90 mmHg); fasting blood glucose was classified as ideal (<100 mg/dL and untreated), intermediate (100–125 mg/dL or treated to goal), or poor (≥126 mg/dL); and total cholesterol status was classified as ideal (<200 mg/dL and untreated), intermediate (200 to 239 mg/dL or treated to goal), or poor (≥240 mg/dL).
Assessment of depression
Depression was assessed using the Center for Epidemiologic Studies Depression Scale (CES-D). The CES-D contains 20 items and measures six components including depressed mood, feelings of guilt and worthlessness, feelings of helplessness and hopelessness, psychomotor retardation, loss of appetite and sleep disturbance. Respondents indicated how often they experienced the symptoms in last week. Their answers could be: “rarely or none of the time” (score 0), “some or little of the time” (score 1), “occasionally or a moderate amount of time” (score 2) and “most or all of the time” (score 3). Scores for the 20 items were summed to yield a total score ranging from 0 to 60, with higher scores indicating greater severity in depressive symptoms. Scores of 16 and above are considered indicative of having depressive symptoms28,29.
Assessment of Potential Covariates
Information on demographic and clinical characteristics (age, sex, marital status, heavy alcohol consumption, personal monthly income, education and history of diseases) was collected via questionnaires. Age was classified into three categories: <40 years, 40–59 years and ≥60 years. Marital status was divided into being married and unmarried (including single, divorced or widowed). Heavy alcohol consumption was defined as a daily intake of at least 100 ml of liquor (equivalent to 240 ml of wine or 720 ml of beer) for more than a year. Previous history of disease, including myocardial infarction, stroke and cancer, was based on self-report. The average monthly income was categorized as “<¥3,000”, “¥3,000–4,999” and “≥¥5,000”. The educational attainment was categorized as “illiteracy or primary”, “middle/high school” and “college graduate or above”.
Statistical Analyses
Continuous variables were described with mean (standard deviation, SD) and compared using ANOVA analysis. Categorical variables were described with percentages and compared using Chi-square test. Logistic regression was used to analyze the association between each CVH metric and presence of depressive symptoms by calculating the odds ratios (ORs) and 95% confidence interval (CI). We adjusted for age, gender, marital status, heavy alcohol consumption, income level, education level and history of myocardial infarction, stroke and cancer in the models because they were known as possible risk factors for depression5,6,30,31.
To assess the collective impact of ideal CVH metrics on depression, we calculated a summary score of ideal CVH metrics. Each CVH metric was assigned a score as follows: “poor” was coded as “0”, the “intermediate” was coded as “1” and “ideal” was coded as “2”. The summary score of ideal CVH metrics for each individual was the sum of the scores of his/her seven CVH metrics. In the logistic regression models estimating the relationship between the summary score and depression, the summary was entered in the models as quartiles (with the lowest quartile as the reference).
As sensitivity analyses, we estimated the association between CVH metrics and depression stratified by sex and age groups. All statistical tests were 2-sided with the significance level set at P ≤ 0.05. All analyses were performed using SAS 9.3 (SAS Institute, Cary, North Carolina, USA).
Additional Information
How to cite this article: Li, Z. et al. Association between Ideal Cardiovascular Health Metrics and Depression in Chinese Population: A Cross-sectional Study. Sci. Rep. 5, 11564; doi: 10.1038/srep11564 (2015).
References
Parker, G., Gladstone, G. & Chee, K. T. Depression in the planet’s largest ethnicgroup: the Chinese. Am J Psychiatry 158, 857–64 (2001).
World Health Organization, World suicide prevention day 2012. Available from: http://www.who.int/mediacentre/events/annual/world_suicide_prevention_day/en/Accessed 16, 6 (2012).
Bunker, S. J. et al. “Stress” and coronary heart disease: psychosocial risk factors. Med J Aust 178, 272–6 (2003).
Marano, C. M. et al. The relationship between fasting serum glucose and cerebral glucose metabolism in late-life depression and normal aging. Psychiatry Res 222, 84–90 (2014).
Denollet, J., Freedland, K. E., Carney, R. M., de Jonge, P. & Roest, A. M. Cognitive-affective symptoms of depression after myocardial infarction: different prognostic importance across age groups. Psychosom Med 75, 701–8 (2013).
Thomson, W. Rate of Stroke Death after Depression: A 40-year Longitudinal Study Extension of Chichester/Salisbury Catchment Area Study. J Stroke Cerebrovasc Dis 23, 1837–42 (2014).
Khalaila, R. & Litwin, H. Changes in health behaviors and their associations with depressive symptoms among Israelis aged 50+. J Aging Health 26, 401–21 (2014).
Lloyd-Jones, D. M. et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation 121, 586–613 (2010).
Espana-Romero, V. et al. A prospective study of ideal cardiovascular health and depressive symptoms. Psychosomatics 54, 525–35 (2013).
Kronish, I. M., Carson, A. P., Davidson, K. W., Muntner, P. & Safford, M. M. Depressive symptoms and cardiovascular health by the American Heart Association’s definition in the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study. PLoS One 7, e52771 (2012).
Sanchez-Villegas, A. et al. Dietary fat intake and the risk of depression: the SUN Project. PLoS One 6, e16268 (2011).
Weng, T. et al. Is there any relationship between dietary patterns and depression and anxiety in Chinese adolescents? Public Health Nutrition 15, 673–82 (2012).
Seppala, J., Kauppinen, A., Kautiainen, H., Vanhala, M. & Koponen, H. [Depression and diet ]. Duodecim 130 902–9 (2014).
Scarapicchia, T. M. et al. Physical activity motivation mediates the association between depression symptoms and moderate-to-vigorous physical activity. Prev Med. 66, 45–8 (2014).
Rothenbacher, D. et al. Prognostic value of one-year course of symptoms of anxiety and depression in patients with coronary heart disease: Role of physical activity and unmet medical need. Eur J Prev Cardiol 00, 1–10, 10.1177/2047487314545317 (2014).
Zhang, M. et al. Relation between anxiety, depression and physical activity and performance in maintenance hemodialysis patients. J Ren Nutr. 24, 252–60 (2014).
Melin, E. O., Thunander, M., Landin-Olsson, M., Hillman, M. & Thulesius, H. O. Depression, smoking, physical inactivity and season independently associated with midnight salivary cortisol in type 1 diabetes. BMC Endocr Disord 14, 75 (2014).
Choi, N. G. & DiNitto, D. M. Role of New Diagnosis, Social Isolation and Depression in Older Adults’ Smoking Cessation. Gerontologist 00, 1–9, 10.1093/geront/gnu 049 (2014).
Bland, P. Smoking cessation improves anxiety depression. Practitioner 258, 5 (2014).
Shin, J. Y., Suls, J. & Martin, R. Are cholesterol and depression inversely related? A meta-analysis of the association between two cardiac risk factors. Ann Behav Med. 36, 33–43 (2008).
Robbins, J. M., Korda, H. & Shapiro, M. F. Treatment for a nondisease: the case of low blood pressure. Soc Sci Med 16, 27–33 (1982).
Donner-Banzhoff, N., Chan, Y., Szalai, J. P. & Hilditch, J. R. Low blood pressure associated with low mood: a red herring? J Clin Epidemiol 50, 1175–81 (1997).
Pilgrim, J. A. Low blood pressure, low mood? BMJ 304, 75–8 (1992).
Hildrum, B. et al. Association of low blood pressure with anxiety and depression: the Nord-Trondelag Health Study. J Epidemiol Community Health 61, 53–8 (2007).
Michalkiewicz, M., Knestaut, K. M., Bytchkova, E. Y. & Michalkiewicz, T. Hypotension and reduced catecholamines in neuropeptide Y transgenic rats. Hypertension 41, 1056–62 (2003).
Li, L. M. et al. A description on the Chinese national nutrition and health survey in 2002. Zhonghua Liu Xing Bing Xue Za Zhi 26, 478–84 (2005).
Zhuang, M. et al. Reproducibility and relative validity of a food frequency questionnaire developed for adults in Taizhou, China. PLoS One 7, e48341 (2012).
Poulin, C., Hand, D. & Boudreau, B. Validity of a 12-item version of the CES-D used in the National Longitudinal Study of Children and Youth. Chronic Dis Can 26, 65–72 (2005).
Surkan, P. J. et al. Early maternal depressive symptoms and child growth trajectories: a longitudinal analysis of a nationally representative US birth cohort. BMC Pediatr 14, 185 (2014).
Vroege, E. M., Zuidersma, M. & de Jonge, P. Vital exhaustion and somatic depression: the same underlying construct in patients with myocardial infarction? Psychosom Med. 74, 446–51 (2012).
Weiss, W. T. et al. The relationship between age, anxiety and depression in older adults with cancer. Psychooncology 10.1002/pon.3638 (2014).
Acknowledgements
We appreciate the participation of the residents and members of the survey teams from the Jidong community and the staff assistance of Recovery Medical Technology Development Co., Ltd. This study was supported by the research grants of the National 12th Five-Year Major Projects of China (2012BAI37B03) and Edith Cowan University Industry Collaboration Scheme 2013 (G1001368). WW were supported by the Importation and Development of High-Calibre Talents Project of Beijing Municipal Institutions.
Author information
Authors and Affiliations
Contributions
Z.L., X.Y., X.W., Q.S. and W.W. conceived and designed this study, Z.L., A.W. and J.Q. directed data analysis, Z.L. and X.Y. writing the paper. Z.L., A.W. and J.Q. prepared the database and reviewed the paper. X.W., Q.S. and W.W. conducted the quality assurance, reviewed and edited the paper. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Li, Z., Yang, X., Wang, A. et al. Association between Ideal Cardiovascular Health Metrics and Depression in Chinese Population: A Cross-sectional Study. Sci Rep 5, 11564 (2015). https://doi.org/10.1038/srep11564
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep11564
This article is cited by
-
Improving mental health in black men through a 24-week community-based lifestyle change intervention: the black impact program
BMC Psychiatry (2024)
-
Identifying factors associated with depression among men living with HIV/AIDS and undergoing antiretroviral therapy: a cross-sectional study in Heilongjiang, China
Health and Quality of Life Outcomes (2018)
-
Achieving Optimal Cardiovascular Health: a Social Epidemiological Approach
Current Epidemiology Reports (2018)
-
Association between Insomnia and Metabolic Syndrome in a Chinese Han Population: A Cross-sectional Study
Scientific Reports (2017)
-
Integration of suboptimal health status and endothelial dysfunction as a new aspect for risk evaluation of cardiovascular disease
EPMA Journal (2016)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
