
Abstract
High serum free fatty acid (FFA) levels are associated with metabolic syndrome (MS). This study aimed to assess the association of fasting serum FFAs with nonalcoholic fatty liver disease (NAFLD) in a Chinese population. A total of 840 subjects fulfilled the diagnostic criteria of NAFLD and 331 healthy control participants were enrolled in this cross-sectional study. Fasting serum FFA levels and other clinical and laboratory parameters were measured. NAFLD patients had significantly higher serum FFA levels than controls (P < 0.001). Serum FFA levels were significantly and positively correlated with parameters of MS, inflammation indexes and markers of hepatocellular damage. Elevated serum FFA levels were found in NAFLD subjects with individual components of MS (obesity, hypertriglyceridaemia and hyperglycaemia). Stepwise regression showed that serum FFA levels were an independent factor predicting advanced fibrosis (FIB-4 ≥ 1.3) in NAFLD patients. Serum FFA levels correlated with NAFLD and could be used as an indicator for predicting advanced fibrosis in NAFLD patients.
Similar content being viewed by others


Introduction
Nonalcoholic fatty liver disease (NAFLD) refers to a wide spectrum of chronic liver disorders, from simple steatosis to nonalcoholic steatohepatitis (NASH) and advanced fibrosis and cirrhosis without significant ethanol consumption1,2. Indeed, simple steatosis is generally stable and does not evolve into NASH in most cases. Only a minority of individuals, those with NASH, are prone to the risk of fibrosis and cirrhosis3. NAFLD has recently been recognised as a major public health problem, affecting as much as 20% of the general population in China over the past few decades4,5. The etiology of NAFLD reflects complex interactions between genetic, neurohumoral, metabolic and stress-related factors6,7. The liver plays a principal role in lipid metabolic pathways by taking up serum free fatty acid (FFA) and manufacturing, storing and transporting lipid metabolites8. The accumulation of lipids, mainly triacylglycerol (TAG), in hepatocytes is the hallmark feature of the pathogenesis of NAFLD9. Donnelly et al. reported that the circulating nonesterified fatty acid pool contributed to the majority of the FFA that flow to the liver and constituted the bulk of the fasting liver TAG pool10.
Metabolic syndrome (MS) is the term given to a cluster of risk factors for cardiovascular disease, including abdominal obesity, diabetes mellitus with raised fasting plasma glucose, raised blood pressure and dyslipidaemia11. Over the past two decades, a striking increase in the prevalence of MS worldwide has taken place along with the global epidemic of obesity12. This constellation of metabolic abnormalities is also becoming increasingly common in China, as shown by emerging prevalence data13. MS has been associated with an increased risk of NAFLD and cardiovascular disease morbidity and mortality, resulting in an increased economic burden on society14. The most widely accepted mechanism underlying MS is insulin resistance (IR)15. Over the past few years, an association between increased fatty acid flux and MS has been well demonstrated16,17. IR results in excessive flux of fatty acid as a result of unopposed adipose tissue lipolysis18. Accumulation of FFA can further increase IR by modulating insulin receptor expression and post-receptor signalling19.
NAFLD is considered to be the hepatic manifestation of metabolic syndrome, sharing a causative factor in IR20. The association between NAFLD and FFA level is controversial in the literature. Some studies have focused on the same lipotoxic properties of FFA, however, a recent in vitro study proposed that the cellular and metabolic effects of FFA on hepatocytes vary depending on their composition21,22,23. However, there are limited studies investigating serum FFA levels in patients with NAFLD. Serum alanine aminotransferase (ALT), aspartate aminotransferase (AST) and glutamyltransferase (GGT) are closely related to NAFLD and may act as markers for the severity of liver damage24,25. MS and inflammation are well-established risks factor for NAFLD26,27. We hypothesise that analysis of the relationship between serum FFA levels and parameters of metabolic syndrome (body mass index, BMI; systolic blood pressure, SBP; triglyceride, TG; total cholesterol, TC; fasting plasma glucose, FPG), inflammatory indexes (sialic acid, SA; high-sensitivity C-reactive protein, hsCRP; white blood cells, WBC) and markers of hepatocellular damage (ALT, AST and GGT) may indirectly lead to a further understanding of serum FFA levels and NAFLD. This cross-sectional study aimed to characterise the relationship between changes in serum FFA and NAFLD in a Chinese population.
Methods
Subjects
The study initially enrolled 920 patients diagnosed with fatty liver based on abdominal ultrasonography. Subjects who met the following criteria were excluded: (i) those with alcohol consumption > 140 g/week for men and > 70 g/week for women (n = 20); (ii) those with a history of viral hepatitis (n = 46), autoimmune hepatitis or other forms of chronic liver disease (n = 14). The remaining 840 patients with NAFLD (mean age: 46.1 ± 12.2 years; female: 239; male: 601) and 331 age- and gender-matched healthy subjects (mean age: 47.0 ± 10.7 years; female: 96; male: 235) were used in the current analyses. Informed consent was obtained from all the subjects and the study was approved by the ethics committee of the first affiliated hospital of the medical college at Zhejiang university in China.
Clinical and anthropometric parameters
The clinical examinations were conducted in the morning after an overnight fast. Weight, height and blood pressure (SBP; DBP, diastolic blood pressure) were measured and BMI was calculated as weight in kilograms divided by height in meters squared. FIB-4 index was calculated according to the following equation:  28. Liver ultrasound examinations were performed by experienced radiologists who were unaware of the clinical and laboratory data, using a Toshiba Nemio 20 sonography machine with a 3.5-MHz probe (Toshiba, Tokyo, Japan).
28. Liver ultrasound examinations were performed by experienced radiologists who were unaware of the clinical and laboratory data, using a Toshiba Nemio 20 sonography machine with a 3.5-MHz probe (Toshiba, Tokyo, Japan).
Biochemical analyses
Fasting whole blood samples were obtained from an antecubital vein and blood samples were used for the analysis of the haematological index and biochemical values. All samples were analysed by specialised clinical laboratory medical personnel. The laboratory parameters included measurement of ALT, AST, GGT, creatine kinase (CK), TG, TC, HDL-C, low-density lipoprotein cholesterol (LDL-C), uric acid (UA), FPG, haemoglobin A1c (HbA1c), homocysteine (Hcy), SA, hsCRP, WBC, pancreatic lipase (P-LIP), amylase (AMY), FFA, haemoglobin (HGB), platelets (PLT) and red blood cell distribution width (RDW). All biochemical values were measured using a Hitachi 7600 clinical analyser (Hitachi, Tokyo, Japan) and Sysmex XE-2100 auto-analyser (Sysmex, Kobe, Japan) using standard methods.
Diagnostic criteria for NAFLD and MS
Hepatic steatosis was diagnosed according to the guidelines established for the diagnosis and treatment of NAFLD issued by the Fatty Liver Disease Study Group of the Chinese Liver Disease Association29. Specifically, hepatic steatosis was diagnosed according to characteristic echo patterns, such as diffuse hyperechogenicity of the liver relative to the kidneys, ultrasound beam attenuation and poor visualisation of intrahepatic structures. The prevalence of MS differs widely in varying studies according to the definition criteria used and the population sample studied30,31. To adopt an ethnicity-specific value of waist circumference, the International Diabetes Federation (IDF) has proposed regional definitions of central obesity according to the characteristics of Chinese people. According to IDF guidelines, for a person to be defined as having MS they must have three or more of the following: central obesity (defined as a waist circumference > 90 cm for Chinese men and > 80 cm for Chinese women); BMI > 25 kg/m2; raised circulating triglyceride levels (defined as triglycerides ≥ 1.7 mmol/L) or specific treatment for this lipid abnormality; reduced HDL-C levels (defined as HDL-C < 1.03 mmol/L in male patients and < 1.29 mmol/L in female patients); raised blood pressure (defined as SBP ≥ 130 mm Hg or DBP ≥ 85 mm Hg) or treatment for previously diagnosed hypertension; and raised FPG (defined as FPG ≥ 5.6 mmol/L) or previously diagnosed type 2 diabetes.
Data and statistical analysis
Statistical analyses were performed using SPSS, version 16 (SPSS, Chicago, IL, USA). Data are presented as the mean ± standard deviation when data were found to be normally distributed or as the median if the distribution was skewed. Differences between groups were analysed using the Student's t-test or the Mann–Whitney U test. Spearman correlation analysis was used to examine the correlation between serum FFA levels and clinical and laboratory parameters. The parameters for multivariate logistic regression were selected by univariate regression analysis.
Ethics Statement
This study was approved by the Hospital Ethics Committee and was performed in accordance with the Helsinki Declaration.
Results
Characteristics of Subjects
Demographic and biochemical characteristics of study participants are summarised in Table 1. We found that patients with NAFLD had significant differences in terms of BMI, SBP, DBP, ALT, AST, GGT, CK, TG, TC, HDL-C, LDL-C, FPG, UA, HbA1C, Hcy, Fe, SA, hsCRP, WBC, P-LIP, AMY, HGB, PLT and RDW compared with controls. Specifically, the levels of these parameters were less favourable in subjects with NAFLD compared with the controls. Consistent with our hypothesis, we found that serum FFA levels were markedly higher in patients with NAFLD than in the controls (median 0.65 mmol/L vs. 0.45 mmol/L; P < 0.001). Characteristics of the NAFLD patients according to their diabetic status are presented in Table 2. The diabetic NAFLD group had higher GGT, TG, FPG, UA, HbA1C, SA and WBC levels and a lower AMY level. Notably, significantly higher FFA levels were observed in the NAFLD subjects with diabetes.
Association between serum FFA levels and NAFLD
Our results show that serum FFA levels were significantly and positively correlated with parameters of MS [body mass index (r = 0.189, P < 0.001), triglyceride (r = 0.338, P < 0.001), total cholesterol (r = 0.169, P < 0.001) and fasting plasma glucose (r = 0.205, P < 0.001)], inflammatory indexes [sialic acid (r = 0.196, P < 0.001), high-sensitivity C-reactive protein (r = 0.145, P = 0.001) and white blood cell (r = 0.177, P < 0.001)] and markers of hepatocellular damage [(alanine aminotransferase (r = 0.157, P < 0.001), aspertate aminotransferase (r = 0.182, P < 0.001) and glutamyltransferase (r = 0.179, P < 0.001)] and negatively correlated with high-density lipoprotein cholesterol levels [(r = −0.172, P < 0.001)]. MS and inflammation are two major factors that are closely associated with NAFLD23. The present observation suggest that they may act as cofactors for the link between serum FFA levels and NAFLD.
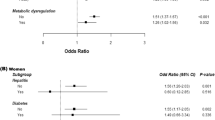
As shown in Figure 1, serum FFA levels were significantly higher in obese subjects (BMI > 25 kg/m2) than in lean subjects (BMI ≤ 25 kg/m2). However, there was no significant difference when subjects were classified according to blood pressure. The group with higher FPG levels (FPG ≥ 5.6 mmol/L) showed increased serum FFA levels. Similarly, the FFA levels were increased in the higher TG group (TG ≥ 1.7 mmol/L) compared with the lower TG group (TG < 1.7 mmol/L).

Serum FFA levels according to characteristics of metabolic syndrome.
Serum FFA levels in the group with FIB-4 ≥ 1.3 were significantly higher than those in the group with FIB-4 < 1.3 (median 0.72 mmol/L vs. 0.58 mmol/L; P < 0.001). We used univariate regression to analyze the odds and p-values (shown in Table 3) with forward selection and we subsequently considered FFA, age, gender, BMI, γ-GT, ALT, hsCRP and presence of diabetes (all p < 0.05) within the multivariate regression analysis. The results of unadjusted and adjusted multivariate logistic regression analysis models are shown in Table 4. Following adjustment for age, gender, BMI, γ-GT, ALT, hsCRP and presence of diabetes (all P < 0.05) selected by stepwise regression, showed that serum FFA levels were an independent factor predicting advanced fibrosis (FIB-4 ≥ 1.3) in NAFLD participants.
Discussion
This is one of the few studies performed to date addressing changes in blood biochemical parameters in a large cohort (n = 840) of subjects of the same ethnicity (Chinese) with NAFLD. The results suggest that serum FFA levels are strongly association with NAFLD. First, NAFLD patients had increased serum FFA levels and these levels were positively correlated with parameters of MS (BMI, TG, TC and FPG), indexes of inflammation (SA, hsCRP and WBC) and markers of hepatocellular damage (ALT, AST and GGT). Second, NAFLD subjects with diabetes had higher serum FFA levels. Third, to obtain a better understanding of the association between serum FFA levels and NAFLD, all subjects with NAFLD were classified according to components of MS. This subgroup analysis indicated elevated serum FFA levels were significantly associated with individual components of MS (obesity, hypertriglyceridaemia and hyperglycaemia). Furthermore, logistic regression analysis showed that serum FFA levels were an independent factor predicting advanced fibrosis (FIB-4 ≥ 1.3) in NAFLD subjects.
One of the possible explanations for the increased FFA levels in NAFLD patients is insulin resistance32,33. Insulin resistance is well known as a pathophysiological hallmark of NAFLD34. Fasting serum FFA primarily originate from lipolysis in adipose tissue. The human body mobilises stored fat by catalysis of hormone sensitive lipase, which hydrolyses the fat into glycerol and fatty acids in the fasted state35. Insulin induces the dephosphorylation of hormone-sensitive lipase by reducing the concentration of cyclic adenosine monophosphate (cAMP) and activating phosphoprotein phosphatase, thus inhibiting lipase activity and decreasing fat hydrolysis36. It has been extensively documented that insulin resistance results in an increased flux of FFA.
The other possible mechanism linking serum FFA with NAFLD is the impaired ability of the liver to export or utilise FFA. Besides beta oxidation, the majority of FFA entering the hepatocyte are used for the synthesis of triglyceride, which then becomes a constituent of very low density lipoprotein (VLDL) particles that are exported into the blood37. It has been demonstrated that beta oxidation of FFA and export of VLDLs in the liver are impaired in NAFLD patients38. The elevated serum levels of FFA are therefore dependent on the imbalance between its origin and use in NAFLD.
The link between serum FFA levels and NAFLD suggested that FFA could play a pivotal role in the development of NAFLD39. Increased systemic oxidative stress in patients with NAFLD has long been recognised both in animal experiments and clinical studies40,41. FFA are responsible for development of hepatocellular apoptosis and injury, acting as a strong oxidant in several pathological states such as MS or type 2 diabetes42,43. High FFA levels also attenuate the insulin-mediated suppression of endogenous glucose production and gluconeogenesis, leading to the impairment of whole-body glucose tolerance44. High serum ALT, AST and GGT levels are associated with the more severe form of NAFLD, although low serum ALT, AST or GGT levels do not rule out the possibility of an advanced stage of NAFLD45,46. The correlation between FFA and markers of hepatocellular damage in the present study indirectly confirm the hypothesis that FFA significantly correlate with hepatocellular injury. Further studies are needed to clarify the detailed mechanism by which FFAs influence the progression of NAFLD.
NAFLD is a well-known risk factor for cardiovascular disease47. The association between FFA and NAFLD may provide a possible explanation for why NAFLD is closely related with cardiovascular disease. FFA can stimulate vascular smooth muscle proliferation and induce endothelial dysfunction, which may contribute to the cardiovascular events of NAFLD48. Furthermore, FFA have been implicated in the physiological mechanism of cardiovascular disease resulting from low-grade systemic inflammatory processes49,50. On the basis of our study, we can only propose a role of FFA in the aetiology of NAFLD and inflammation from a snapshot of the circulating FFA state. However, the question of whether or not elevated serum FFA are an unrelated phenomenon, a cause, or a consequence of NAFLD could not be determined from this cross-sectional study. Traditionally, NAFLD has been viewed as a spectrum that progresses from pure fatty liver through NASH to severe fibrosis, cirrhosis and eventually hepatocellular carcinoma51. According to recent views, uncomplicated steatosis and NASH tend to be considered as potentially unrelated disorders, not only based on histological definitions but also from pathophysiological evidence52,53. The identification of differences in serum FFA between simple steatosis and NASH in further studies may be important to clarify their precise interrelationship.
This study has some limitations. First, the diagnosis of NAFLD was based on ultrasonographic examination. Ultrasonography is not sensitive enough to detect mild steatosis, but overall it significantly correlates with both liver histology and metabolic derangements54. Given the acceptable sensitivity and specificity for detecting hepatic steatosis, ultrasonography is widely used in epidemiological studies of NAFLD55. Second, postprandial serum levels of FFA have not been examined in this study. Nevertheless, fasting serum FFA constitute the majority of fatty acids delivered to the liver and contribute to liver fat metabolism and accumulation in NAFLD. Third, we used the FIB-4 index for evaluating advanced fibrosis of NAFLD according the studies of Xun YH et al.56. FIB-4, a simple non-invasive index composed of readily available routine laboratory tests, can accurately predict advanced fibrosis and cirrhosis in patients with NAFLD. However, it is not sensitive enough to identify patients with a mild degree of fibrosis who are at risk of progression57,58.
In conclusion, our results demonstrate a significant correlation between serum FFA levels and NAFLD. Further research on the involvement of FFA in NAFLD will not only enhance our understanding of the development of NAFLD, but also benefit in the eventual development of new prevention and treatment strategies for the disease.
References
Athyros, V. G., Katsiki, N. & Karagiannis, A. Comment on: Novel therapeutic targets for non-alcoholic fatty liver disease. Expert Opin Ther Targets. 17, 861–862 (2013).
Bhala, N., Jouness, R. I. & Bugianesi, E. Epidemiology and natural history of patients with NAFLD. Curr Pharm Des. 19, 5169–5176 (2013).
Lonardo, A., Sookoian, S., Chonchol, M., Loria, P. & Targher, G. Cardiovascular and systemic risk in nonalcoholic fatty liver disease - atherosclerosis as a major player in the natural course of NAFLD. Curr Pharm Des. 19, 5177–5192 (2013).
Liao, X., Cao, X., Liu, J. & Xie, X. Prevalence and features of fatty liver detected by physical examination in Guangzhou. World J Gastroenterol. 19, 5334–5339 (2013).
Li, Z. et al. Prevalence of nonalcoholic fatty liver disease in mainland of China: a meta-analysis of published studies. J Gastroenterol Hepatol. 29, 42–51 (2014).
Petta, S. et al. Glucokinase regulatory protein gene polymorphism affects liver fibrosis in non-alcoholic Fatty liver disease. PLoS One. 9, e87523 (2014).
Miele, L. et al. A case-control study on the effect of metabolic gene polymorphisms, nutrition and their interaction on the risk of non-alcoholic fatty liver disease. Genes. Nutr. 9, 383 (2014).
Musso, G., Gambino, R. & Cassader, M. Recent insights into hepatic lipid metabolismin non-alcoholic fatty liver disease (NAFLD). Prog Lipid Res. 48, 1–26 (2009).
Stanković, M. N. et al. Time-dependent Changes and Association Between Liver Free Fatty Acids, Serum Lipid Profile and Histological Features in Mice Model of Nonalcoholic Fatty Liver Disease. Arch Med Res. 45, 116–124 (2014).
Donnelly, K. L. et al. Sources of fatty acids stored in liver and secreted via lipoproteins in patients with nonalcoholic fatty liver disease. J Clin Invest. 115, 1343–1351 (2005).
Hong, S. et al. Association between cardiorespiratory fitness and the prevalence of metabolic syndrome among Korean adults: a cross sectional study. BMC Public Health. 14, 481 (2014).
Eckel, R. H., Alberti, K. G., Grundy, S. M. & Zimmet, P. Z. The metabolic syndrome. Lancet. 375, 181–183 (2010).
Xi, B., He, D., Hu, Y. & Zhou, D. Prevalence of metabolic syndrome and its influencing factors among the Chinese adults: the China Health and Nutrition Survey in 2009. Prev Med. 57, 867–871 (2013).
Chiefari, E. et al. A polymorphism of HMGA1 is associated with increased risk of metabolic syndrome and related components. Sci Rep. 3, 1491 (2013).
Haas, J. T. & Biddinger, S. B. Dissecting the role of insulin resistance in the metabolic syndrome. Curr Opin Lipidol. 20, 206–210 (2009).
Chavez-Tapia, N. C., Rosso, N. & Tiribelli, C. Effect of intracellular lipid accumulation in a new model of non-alcoholic fatty liver disease. BMC Gastroenterol. 12, 20 (2012).
Kneeman, J. M., Misdraji, J. & Corey, K. E. Secondary causes of nonalcoholic fatty liver disease. Therap Adv Gastroenterol. 5, 199–207 (2012).
Frühbeck, G., Méndez-Giménez, L., Fernández-Formoso, J. A., Fernández, S. & Rodríguez, A. Regulation of adipocyte lipolysis. Nutr Res Rev. 28, 1–31 (2014).
Ruddock, M. W. et al. Saturated fatty acids inhibit hepatic insulin action by modulating insulin receptor expression and post-receptor signalling. J Biochem. 144, 599–607 (2008).
Patton, H. M. et al. Association between metabolic syndrome and liver histology among children with nonalcoholic Fatty liver disease. Am J Gastroenterol. 105, 2093–2102 (2010).
Larter, C. Z. et al. Hepatic free fatty acids accumulate in experimental steatohepatitis: role of adaptive pathways. J Hepatol. 48, 638–647 (2008).
Bechmann, L. P. et al. Free fatty acids repress small heterodimer partner (SHP) activation and adiponectin counteracts bile acid-inducedliver injury in superobese patients with nonalcoholic steatohepatitis. Hepatology. 57, 1394–1406 (2013).
Ricchi, M. et al. Differential effect of oleic and palmitic acid on lipid accumulation and apoptosis in cultured hepatocytes. J Gastroenterol Hepatol. 24, 830–840 (2009).
Marchesini, G. et al. Aminotransferase and gamma-glutamyltranspeptidase levels in obesity are associated with insulin resistance and the metabolic syndrome. J Endocrinol Invest. 28, 333–339 (2005).
Chang, Y., Ryu, S., Sung, E. & Jang, Y. Higher concentrations of alanineamino transferase within the reference interval predict nonalcoholic fatty liver disease. Clin Chem. 53, 686–692 (2007).
Park, S. H. et al. Insulin resistance and C-reactive protein as independent risk factors for non-alcoholic fatty liver disease in non-obese Asian men. J Gastroenterol Hepatol. 19, 694–698 (2004).
Fan, J. G. et al. What are the risk factors and settings for non-alcoholic fatty liver disease in Asia-Pacific? J Gastroenterol Hepatol. 22, 794–800 (2007).
Adams, L. A. et al. Complex non-invasive fibrosis models are more accurate than simple models in non-alcoholic fatty liver disease. J Gastroenterol Hepatol. 26, 1536–1543 (2011).
Zeng, M. D. et al. Chinese National Consensus Workshop on Nonalcoholic Fatty Liver Disease. J Dig Dis. 9, 108–112 (2008).
Chen, S. H., He, F., Zhou, H. L., Wu, H. R., Xia, C. & Li, Y. M. Relationship between nonalcoholic fatty liver disease and metabolic syndrome. J Dig Dis. 12, 125–130 (2011).
Giannini, D., Kuschnir, M. C. & Szklo, M. Metabolic Syndrome in Overweight and Obese Adolescents: A Comparison of Two Different Diagnostic Criteria. Ann Nutr Metab. 64, 71–79 (2014).
Kovacs, P. & Stumvoll, M. Fatty acids and insulin resistance in muscle and liver. Best Pract Res Clin Endocrinol Metab. 19, 625–635 (2005).
Capurso, C. & Capurso, A. From excess adiposity to insulin resistance: the role of free fatty acids. Vascul Pharmacol. 57, 91–97 (2012).
Vernon, G., Baranova, A. & Younossi, Z. M. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther. 34, 274–285 (2011).
Hsiao, P. J. et al. Risk interaction of obesity, insulin resistance and hormone-sensitive lipase promoter polymorphisms (LIPE-60 C > G) in the development of fatty liver. BMC Med Genet. 14, 54 (2013).
Stralfors, P. & Honnor, R. C. Insulin-induced dephosphorylation of hormone-sensitive lipase. Correlation with lipolysis and cAMP-dependent protein kinase activity. Eur J Biochem. 182, 379–385 (1989).
Gaemers, I. C. & Groen, A. K. New insights in the pathogenesis of non-alcoholic fatty liver disease. Curr Opin Lipidol. 17, 268–273 (2006).
Musso, G., Gambino, R. & Cassader, M. Recent insights into hepatic lipid metabolism in non-alcoholic fatty liver disease (NAFLD). Prog Lipid Res. 48, 1–26 (2009).
Jacome-Sosa, M. M. & Parks, E. J. Fatty acid sources and their fluxes as they contribute to plasma triglyceride concentrations and fatty liver in humans. Curr Opin Lipidol. 25, 213–220 (2014).
Narasimhan, S. et al. Oxidative stress is independently associated with non-alcoholic fatty liver disease (NAFLD) in subjects with and without type 2 diabetes. Clin Biochem. 43, 815–821 (2010).
Xiao, J. et al. Epigallocatechin gallate attenuates fibrosis, oxidative stress and inflammation in non-alcoholic fatty liver disease rat model through TGF/SMAD, PI3 K/Akt/FoxO1 and NF-kappa B pathways. Eur J Nutr. 53, 187–199 (2014).
Pankow, J. S. et al. Fasting plasma free fatty acids and risk of type2 diabetes: the atherosclerosis risk in communities study. Diabetes Care. 27, 77–82 (2004).
Ahmed, A. & Forrest, E. H. Commentary: Physical activity and NAFLD--cause or effect? Aliment Pharmacol Ther. 36, 1097–1098 (2012).
Roden, M. et al. Effects of free fatty acid elevation on postabsorptive endogenous glucose production and gluconeogenesis in humans. Diabetes. 49, 701–717 (2000).
Mofrad, P. et al. Clinical and histologic spectrum of nonalcoholic fatty liver disease associated with normal ALT values. Hepatology. 37, 1286–1292 (2003).
Fracanzani, A. L. et al. Risk of severe liver disease in nonalcoholic fatty liver disease with normal aminotransferase levels: a role for insulin resistance and diabetes. Hepatology. 48, 792–808 (2008).
Santos, R. D. & Agewall, S. Non-alcoholic fatty liver disease and cardiovascular disease. Atherosclerosis. 224, 324–325 (2012).
Tripathy, D. et al. Elevation of free fatty acids induces inflammation and impairs vascular reactivity in healthy subjects. Diabetes. 52, 2882–2887 (2003).
Naruse, K. et al. Chemokine and free fatty acid levels in insulin-resistant state of successful pregnancy: a preliminary observation. Mediators Inflamm. 2012, 432575 (2012).
Tracy, L. M. et al. Exposure to the saturated free fatty acid palmitate alters BV-2 microglia inflammatory response. J Mol Neurosci. 51, 805–812 (2013).
Vernon, G., Baranova, A. & Younossi, Z. M. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther. 34, 274–285 (2011).
Yilmaz, Y. Review article: is non-alcoholic fatty liver disease a spectrum, or are steatosis and non-alcoholic steatohepatitis distinct conditions? Aliment Pharmacol Ther. 36, 815–823 (2012).
Fielding, C. M. & Angulo, P. Hepatic Steatosis and Steatohepatitis: Are they Really Two Distinct Entities? Curr Hepatology Rep. 13, 151–158 (2014).
Ballestri, S. et al. Ultrasonographic fatty liver indicator, a novel score which rules out NASH and is correlated with metabolic parameters in NAFLD. Liver Int. 32, 1242–1252 (2012).
Hernaez, R. et al. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: a meta-analysis. Hepatology. 54, 1082–1090 (2011).
Xun, Y. H. et al. Suboptimal performance of simple noninvasive tests for advanced fibrosis in Chinese patients with nonalcoholic fatty liver disease. J Dig Dis. 13, 588–595 (2012).
McPherson, S., Stewart, S. F., Henderson, E., Burt, A. D. & Day, C. P. Simple non-invasive fibrosis scoring systems can reliably exclude advanced fibrosis in patients with non-alcoholic fatty liver disease. Gut. 59, 1265–1269 (2010).
Sumida, Y., Yoneda, M. & Hyogo, H. Validation of the FIB4 index in a Japanese nonalcoholic fatty liver disease population. BMC Gastroenterol. 12, 2 (2012).
Acknowledgements
This study was supported by the National Natural Science Foundation of China (No. 81100278) and the Science Foundations of Health Bureau of Zhejiang Province (Nos. 2012RCA026 and 2013KYB116). The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Y.C. designed the experiments. C.F.X., Y.N.H., H.L.L. and J.P.W. performed the experiments. J.W.Z. and Y.Z. wrote the majority of the manuscript text. All authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article's Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder in order to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Zhang, J., Zhao, Y., Xu, C. et al. Association between serum free fatty acid levels and nonalcoholic fatty liver disease: a cross-sectional study. Sci Rep 4, 5832 (2014). https://doi.org/10.1038/srep05832
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep05832
This article is cited by
-
Elevated Kallistatin promotes the occurrence and progression of non-alcoholic fatty liver disease
Signal Transduction and Targeted Therapy (2024)
-
Combining albumin deficiency and acute exercise reduces hepatic lipid droplet size in mice
Lipids in Health and Disease (2023)
-
Relevance and consequence of chronic inflammation for obesity development
Molecular and Cellular Pediatrics (2023)
-
Engineered human hepatocyte organoids enable CRISPR-based target discovery and drug screening for steatosis
Nature Biotechnology (2023)
-
Non-alcoholic fatty liver disease and gut microbial dysbiosis- underlying mechanisms and gut microbiota mediated treatment strategies
Reviews in Endocrine and Metabolic Disorders (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
