
Key Points
-
Demonstrates that there were no significant socioeconomic differences in the use of specific preventive interventions among children.
-
Shows that there were socioeconomic differences in regular dental attendance among children.
-
Suggests there are socioeconomic inequalities in caries experience among children.
Abstract
Aim To assess socioeconomic inequality regarding specific preventive interventions (fissure sealants or any treatment to prevent caries) and dental visits among UK children.
Method Data were from the Children's Dental Health Survey 2003, which included participants from England, Wales, Scotland, and Northern Ireland. The number of children in the analysis was 2,286. Variables were sex, age, area of residency (for example, England), mother's education, family social class, and deprivation level. Descriptive and regression analyses were performed.
Results There were no significant socioeconomic differences in the use of preventive services. Deprivation and family social class (for example, intermediate and manual) were significantly associated with less regular dental visits (odd ratio 0.41, 95% CI [0.28, 0.63]; odd ratio 0.53, 95% CI [0.31, 0.89]; odd ratio 0.37, 95% CI [0.24, 0.58], respectively). Regular dental visits were associated with reporting preventive care for caries (odds ratio 2.25, 95% CI [1.45, 3.49]) and with the number of sealed tooth surfaces (rate ratio 1.73, 95% CI [1.16, 2.60]).
Conclusion Despite apparent socioeconomic inequalities in regular dental visits, there was no significant inequality in using specific preventive interventions by children in the UK. This finding should be interpreted with caution considering the relatively small subsample included in this analysis.
Similar content being viewed by others

Introduction
Oral health is an important public issue that affects human life. Poor oral health can lead not only to aesthetic problems but also to functional problems in adulthood, such as issues with mastication and effects on social relationships related to appearance.1 Although oral health has dramatically improved in the last few years, inequality has increased and the gap between low income and high income has increased in developed countries.2 There is also evidence on inequality in dental caries among children in Britain.2 The occurrence of caries in children was found to be inversely related to parental education and socioeconomic position, in addition to proximal risk factors, such as dietary habits, oral hygiene, and dental attendance.3
There is also inequality in the use of dental services by children, which exacerbates the socioeconomic gap in the oral health of the children.4 Earlier studies have shown that higher level parental education is related to greater dental attendance, while higher family income was related to the use of preventive interventions, such as fissure sealant.5,6 Furthermore, children from lower social classes had higher levels of dental caries than those from higher social classes.6 These findings were repeatedly confirmed in different countries using different indicators of socioeconomic position.7 Other factors associated with the better use of dental services by children included sex (females), area of residence (urban), and availability of private insurance.8
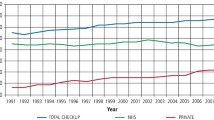
In the UK, the availability of free medical coverage provided by the NHS allegedly reduces inequalities in the use of health services. However, UK women from manual social classes were less likely to have a recent flu vaccination compared with those from non-manual social classes. Similarly, dental check-ups and eye check-ups were more common among women from non-manual social classes than women from manual social classes.9 Patients from higher social classes showed higher attendance levels of health check-ups for cardiovascular diseases than those from lower social classes. However, the disease levels were higher among those at the bottom of the social hierarchy.10,11 Furthermore, individuals with higher incomes or of a higher social status or professionals were more likely to attend preventive health services.9
In relation to the use of dental services by adults in the UK, despite the inclusion of dental care under the NHS, there appeared to be some barriers to the use of services, which could be attributed to co-payment.12,13 On the other hand, the NHS provides comprehensive dental services free of charge for all children. However, given the existence of inequalities in dental caries among children14 and the evidence related to the use of medical services, it is reasonable to hypothesise that inequality in the use of dental services by children exists in the UK. Nevertheless, the association between socioeconomic position and the use of specific preventive interventions by children in the UK has not been sufficiently studied.15
The aim of this study was to assess socioeconomic inequality in the use of dental services and to assess the determinants of the use of specific preventive interventions among children in the UK (England, Scotland, Wales, and Northern Ireland) using data from the Children's Dental Health Survey 2003. More specifically, we will assess the factors associated with provision of fissure sealants as assessed by clinicians and preventive dental care treatment (sealant and fluoride) as reported by parents.
Materials and methods
Study population
Data were from the Children's Dental Health Survey (CDHS) 2003. Although this survey has been superseded by the CDHS 2013, it was selected because it is the last survey that included information on the dental and oral health of representative data from the four nations of the UK (England, Scotland, Wales, and Northern Ireland). The number of children in CDHS 2003 was 12,658 individuals, and 10,381 individuals were examined, which achieved an 82% response rate. Children aged 5 to 15 years were included in the survey.
Measurements
The clinical examination was carried out for all selected children by trained dentists in schools. Clinical criteria used by the British Association for the Study of Community Dentistry (BASCD) was used in the screening survey.16 The criteria were agreed by a steering committee made up of representatives from the commissioning health departments, community dental services, and university dental schools. A structured questionnaire was used to collect sociodemographic characteristics, dietary habits, oral health problems, oral care practices, oral hygiene, and use of dental services. A random subsample of 5,480 examined children was selected to receive the questionnaire; however, only 3,342 questionnaires were returned by the parents (61% replied, 37% refused, and 1% did not respond).
Outcome variables
In this study, we used preventive dental procedures, namely clinically assessed fissure sealant and specific preventive interventions reported by parents as the outcome variables. Two variables for clinically assessed fissure sealants were used: 1) any sealed tooth; 2) number of sealed tooth surfaces. The variable on reported specific preventive interventions indicated whether the child had fissure sealant or fluoride application. Additionally, we used a variable indicating the type of dental visit. Dental visits were originally reported in four categories: regular dental check-ups (visited the dentist in the six months before the survey for check-up); occasional check-ups (time between visits was longer than six months); only when needed; and never. This variable was dichotomised to indicate regular check-up versus irregular or no check-ups (occasional, when needed, or never).
Explanatory variables
The National Statistics Socio-economic Classification (NS–SEC) was used in CDHS 2003 to assess socioeconomic status. In this study, the NS–SEC 3 categories version was used to measure socioeconomic status. The NS–SEC 3 variables included the following categories: managerial or professional; intermediate jobs; manual jobs; and never worked or unclassified. Mother's education was used as a second indicator of socioeconomic status. The variable included three groups of mothers who finished education before the age of 16, from 17 to 18, and over 18. The third marker of socioeconomic position indicated deprivation. Children from schools with more than 30% of children eligible for free school meals were defined as deprived.
Covariates
Other variables included in the analysis were age (8, 12, 15), sex, and country (England, Wales, Northern Ireland, and Scotland). We also included an assessment of lifetime dental caries experience expressed as the sum of decayed and filled deciduous teeth (DFT) and decayed, filled, or missing permanent teeth (DMFT).
Statistical analysis
Data were analysed using SPSS using examination weights and survey commands. Only cases with complete data were included in the analysis and children aged 5 years were excluded because we were interested in fissure sealants in permanent teeth. The number included in the analysis was 2,286. First, we assessed the distribution of all variables included in the analysis, namely, sex, age, country, type of dental visit, mother's education, family NS–SEC 3, DMFT, sum of DMFT and DFT, deprivation, treatment to prevent caries, any sealed tooth, and number of sealed tooth surfaces. Second, the distribution of dental visits, DMFT, sum of DMFT and DFT, reported preventive care, any sealed tooth, and number of sealed tooth surfaces was assessed against family NS–SEC, mother's education, and deprivation. A logistic regression model was used to assess the factors associated with regular dental visits, adjusting for sex, age, country, sum of DMFT and DFT, family NS–SEC 3, mother's education, and deprivation. Finally, two logistic regression models for each reported use of specific preventive interventions and any sealed tooth and a negative binomial regression model for the number of sealed surfaces were constructed. These three models were adjusted for sex, age, country, sum of DMFT and DFT, dental visits, family NS–SEC 3, mother's education, and deprivation.
Results
We analysed data for 2,286 children in the UK, covering four countries: 1,307 from England; 487 from Wales; 194 from Scotland; and 307 Northern Ireland. Table 1 shows the distribution of all variables included in the analysis. Overall, there were 1,159 (49.5%) boys and 1,127 (50.5%) girls; proportions that are almost the same as the gender distribution. A high percentage of the children visited the dentist regularly (86.7%). Only 24.7% of the population reported they used specific preventive interventions (treatment to prevent caries).
Table 2 shows the distribution of the type of dental visit, DMFT, and the use of specific preventive interventions by socioeconomic indicators. Children belonging to professional or managerial families had higher rates of specific preventive interventions (43.3%) compared with other groups. Children whose mothers left school over the age of 18 had higher rates of using specific preventive interventions at 25.24%, and mothers who left school between 17 and 18 were at about 23.7%, while those who left school under 16 years were at 24.6%. Children whose family social class was managerial or professional had higher rates (93.2%) of regular dental attendance than those from intermediate (87.6%), manual families (81.8), and those who never worked (73.4). The percentage of deprived children who regularly visited a dentist was 88.4% compared to 70.4% for non-deprived children. Distributions of DMFT and DFT showed that children whose parents had manual and intermediate jobs had the highest levels of caries. Children whose parents had professional or managerial jobs had more sealed teeth compared to other groups. Finally, children whose mothers had the highest level of education had more sealed teeth than children whose mothers had lower education (Table 2).
Table 3 exhibits the association between socioeconomic indicators and regular dental visits in a fully adjusted model. Only deprivation and family NS–SEC 3 were significantly associated with regular dental visits. Those at the bottom of social hierarchy were less likely to visit a dentist regularly. None of the other variables included in this fully adjusted model were statistically associated with dental visits (Table 3).
Table 4 exhibits the estimates for the association between each reported use of preventive dental care, any sealed tooth, and number of sealed surfaces with socioeconomic factors (mother's education, family NS–SEC 3, and deprivation) and dental visits. None of the three indicators of socioeconomic position were significantly associated with any of the preventive services. On the other hand, regular dental visits were significantly associated with reporting preventive care (odds ratio 2.25, 95% CI [1.45, 3.49]) and with number of sealed tooth surfaces (rate ratio 1.73, 95% CI [1.16, 2.60]; Table 4). Moreover, children in Scotland and Northern Ireland were significantly associated with reporting preventive care and use of fissure sealant compared to England. The oldest children reported more use of preventive care treatment and fissure sealant. Sex was significantly associated with reporting any sealed tooth surface and with the number of sealed tooth surfaces, but was not significant with any treatment to prevent caries. The logistic regression model was adjusted for sex, age, country, sum of DMFT and DFT, dental visits, family NS–SEC, mother's education, and deprivation.
Discussion
Overall, the result demonstrated variations in the use of fissure sealant and other treatments to prevent caries by social class. Higher percentages of children of parents in managerial or professional classes had sealed teeth and reported using preventive services than other groups. However, there was no statistically significant difference in the use of preventive services by socioeconomic status. On the other hand, rates of dental caries were higher among those at the bottom of the social hierarchy. Regular dental visits were more common among children from managerial or professional class families. There was no significant association between the use of preventive services with deprivation or the mothers' education. This finding on the use of specific preventive interventions by children in the UK was different from that observed in other countries lacking free comprehensive dental coverage for children.17
Other studies in the UK indicated the presence of socioeconomic and culture barriers in the use of dental services,12,13,18 which is consistent with our findings pertaining to regular dental check-ups. However, none of the aforementioned studies examined the association between socioeconomic status and the use of specific preventive interventions among children. To the best of our knowledge, this is the first study that used data from a national survey of England, Wales, Scotland, and Northern Ireland to assess socioeconomic inequality in the use of specific preventive interventions among children.
The cost of using dental services is a major barrier to access and to highly needed preventive intervention, particularly among the sectors of the populations with the highest levels of caries, and it exerts financial burden on individuals and communities.19 Furthermore, children are less likely to have dental insurance compared to medical insurance.20 Unsurprisingly, studies from different parts of the world demonstrated socioeconomic inequalities in dental attendance by children and subsequent inequalities in dental caries.7,17,21,26 On the other hand, the UK National Health Service includes dental services and provides free of charge comprehensive dental care for children. The findings of the current study pertaining to the lack of statistically significant socioeconomic variations in the provision of fissure sealants as assessed by clinicians and preventive dental care as reported by parents imply that the availability of free dental services for children could actually eliminate inequality. However, this finding should be interpreted with caution given the relatively small subsample included in this analysis. Perhaps more importantly, despite the apparent lack of inequalities in the use of specific preventive interventions, inequality in the severity and/or extent of dental caries experience persisted in the same population, thus highlighting other determinants of children's caries.
In the current study, deprived children and those whose parents were at the lower end of family NS–SEC 3 were significantly less likely to visit a dentist regularly. This observation highlights the indirect cost of access to dental services. Factors such as inability to take time off work to take a child to the dentist and the cost of transportation are more likely to be experienced by those at the bottom of the social hierarchy and exert an additional barrier to access to dental care despite the free availability.27 Furthermore, other factors such as ethnicity, language barriers, and anxiety could also have contributed to inequality in regular dental visits observed in this study.13
Although the CDHS 2013 was available at the time the study was conducted, we opted to use CDHS 2003 as it was the last survey that included a nationally representative sample of all four nations of the UK. Furthermore, although changes to the NHS contracts have been introduced to England and Wales in 2006, we argue that the inequality in the provision of the preventive interventions in the four nations of the UK has not been affected. Additionally, newer changes to dental contracts have been initiated after the CDHS 2013. Furthermore, the conclusion about the inequality in use of these services by children is also corroborated by evidence from other countries and from non-dental preventive interventions.5,6
There are some limitations of this study. The cross-sectional design of the study does not support temporality of relation between exposure and outcome. The relatively small size of the subsample included in the study could have influenced the findings. Finally, other factors that could have influenced the use of services, such as ethnicity, language, and anxiety were not included in the analysis.
Conclusion
Non-deprived children and those from families with managerial or professional jobs were significantly more likely to visit a dentist regularly than their less affluent counterparts. While the rates of use of specific preventive interventions were higher among more affluent children, there was no statistically significant socioeconomic difference in the use of these services. The findings imply that the availability of free dental care for children in the UK eliminates inequalities in use of preventive services. However, this should be interpreted with caution given the limitation of the sample.
References
Davis P . Culture, inequality and the pattern of dental care in New Zealand. Soc Sci Med A 1981; 15: 801–805.
Watt R, Sheiham A . Inequalities in oral health: a review of the evidence and recommendations for action. Br Dent J 1999; 187: 6–12.
Tadakamadla S K, Tadakamadla J, Tibdewal H, Duraiswamy P, Kulkarni S . Dental caries in relation to socio-behavioural factors of 6yearold school children of Udaipur district, India. Dent Res J 2012; 9: 681–687.
Darmawikarta D, Yang C, Carsley S et al. Factors associated with dental care utilization in early childhood.(Report). Paediatr 2014; 133: e1594–e1600.
Gonzalez C D, Frazier P J, LeMay W, Stenger J P, Pruhs R J . Sealant status and factors associated with sealant presence among children in Milwaukee WI. ASDC J Dent Child 1995; 62: 335–341.
Thomson W M, Poulton R, Milne B J, Caspi A, Broughton J R, Ayers K M . Socioeconomic inequalities in oral health in childhood and adulthood in a birth cohort. Community Dent Oral Epidemiol 2004; 32: 345–353.
Machry R V, Tuchtenhagen S, Agostini B A et al. Socioeconomic and psychosocial predictors of dental healthcare use among Brazilian preschool children. BMC Oral Health 2013; 13: 60.
Pavi E, Karampli E, Zavras D, Dardavesis T, Kyriopoulos J . Social determinants of dental health services utilisation of Greek adults. Community Dent Health 2010; 27: 145–150.
Patel R, Lawlor D A, Ebrahim S . Socio-economic position and the use of preventive health care in older British women: a cross-sectional study using data from the British Women's Heart and Health Study cohort. Fam Pract 2007; 24: 7–10.
Dryden R, Williams B, McCowan C, Themessl-Huber M. What do we know about who does and does not attend general health checks? Findings from a narrative scoping review. BMC Public Health 2012; 12: 723.
Zhang J, Oldenburg B F . Socioeconomic inequalities in utilisation of preventive health services in relation to cardiovascular disease and diabetes. J Behav Health 2014; 3: 87–94.
Al-Haboubi M, Klass C, Jones K, Bernabe E, Gallagher J E . Inequalities in the use of dental services among adults in inner South East London. Eur J Oral Sci 2013; 121: 176–181.
Newton J T, Thorogood N, Bhavnani V, Pitt J, Gibbons D E, Gelbier S . Barriers to the use of dental services by individuals from minority ethnic communities living in the United Kingdom: findings from focus groups. Prim Dent Care 2001; 8: 157–161.
Maliderou M, Reeves S, Noble C . The effect of social demographic factors, snack consumption and vending machine use on oral health of children living in London. Br Dent J 2006; 201: 441–444.
Tickle M, Milsom K, Blinkhorn A . Inequalities in the dental treatment provided to children: an example from the UK. Community Dent Oral Epidemiol 2002; 30: 335–341.
Pitts N B, Evans D J, Pine C M . British Association for the Study of Community Dentistry (BASCD) diagnostic criteria for caries prevalence surveys1996/97. Community Dent Health 1997; 14: 6–9.
Mejia G C, Weintraub J A, Cheng N F et al. Language and literacy relate to lack of children's dental sealant use. Community Dent Oral Epidemiol 2011; 39: 318–324.
Listl S . Income-related inequalities in dental service utilization by Europeans aged 50+. J Dent Res 2011; 90: 717–723.
Masood M, Sheiham A, Bernabe E . Household expenditure for dental care in low and middle income countries. PloS One 2015; 10: e0123075.
Kenney G M, McFeeters J R, Yee J Y . Preventive Dental Care and Unmet Dental Needs Among Low-Income Children. Am J Public Health 2005; 95: 1360–1636.
Ardenghi T M, Vargas-Ferreira F, Piovesan C, Mendes F M . Age of first dental visit and predictors for oral healthcare utilisation in preschool children. Oral Health Prev Dent 2012; 10: 17–27.
Baldani M H, Antunes J L . Inequalities in access and utilization of dental services: a cross-sectional study in an area covered by the Family Health Strategy. Cadernos de Saude Publica 2011; 27 Suppl 2: S272–S283.
Armfield J M . Socioeconomic inequalities in child oral health: a comparison of discrete and composite area-based measures. J Public Health Dent 2007; 67: 119–125.
Palencia L, Espelt A, Cornejo-Ovalle M, Borrell C . Socioeconomic inequalities in the use of dental care services in Europe: what is the role of public coverage? Community Dent Oral Epidemiol 2014; 42: 97–105.
Pinilla J, Negrín-Hernández M A, Abásolo I . Time trends in socio-economic inequalities in the lack of access to dental services among children in Spain 1987–2011. Int J Equity Health 2015; 14: 9.
Tchicaya A, Lorentz N . Socioeconomic inequalities in the non-use of dental care in Europe. Int J Equity Health 2014; 13: 7.
Percac-Lima S, Aldrich L S, Gamba G B, Bearse A M, Atlas S J . Barriers to follow-up of an abnormal Pap smear in Latina women referred for colposcopy. J Gen Intern Med 2010; 25: 1198–1204.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Shaban, R., Kassim, S. & Sabbah, W. Socioeconomic inequality in the provision of specific preventive dental interventions among children in the UK: Children's Dental Health Survey 2003. Br Dent J 222, 865–869 (2017). https://doi.org/10.1038/sj.bdj.2017.499
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2017.499
This article is cited by
-
Effects of early preventive dental visits and its associations with dental caries experience: a cross-sectional study
BMC Oral Health (2022)
-
Disparities in the geographic distribution of NHS general dental care services in England
British Dental Journal (2021)
-
Development and retention of the dental workforce: findings from a regional workforce survey and symposium in England
BMC Health Services Research (2020)
-
Effectiveness of school dental screening on dental visits and untreated caries among primary schoolchildren: study protocol for a cluster randomised controlled trial
Trials (2018)
-
Neighbourhood incidence rate of paediatric dental extractions under general anaesthetic in South West England
British Dental Journal (2018)
