
Key Points
-
Details a comparison survey among two groups of dental practitioners.
-
Provides insight into the type of post/core systems used and rationale behind their selection.
-
Shows effect of postgraduate training on provision of post/core restorations.
Abstract
A cross-sectional survey to investigate the use of intra radicular posts in clinical practice was distributed to GDPs attending continuing professional development lectures and delegates of a specialist prosthodontic conference. Fifty-six (51%) GDP's and fifty-three (49%) conference delegates responded. Forty-five percent of GDP's exclusively used metal posts in comparison to 25% of the conference delegates. The findings of this study suggest there are no differences in the use of intra-radicular posts between GDPs and conference delegates. Formal post-graduate training does appear to have a limited influence over the selection of post materials.
Similar content being viewed by others

Introduction
Restoring a broken down, endodontically treated tooth continues to be a challenging clinical situation. Traditional thinking advocated that all anterior teeth required routine reinforcement with a post and core following root canal treatment,1 as this was thought to strengthen the tooth and prevent internal stress-related root fracture.2 However, studies have shown that posts do not strengthen teeth, but can in fact weaken them.3 Current thinking advocates that posts should only be used when there is insufficient tooth tissue to retain a core of material to allow placement of an indirect restoration.4,5
Post and cores can be constructed from gold,2 titanium and platinum alloys6 and non-precious alloys such as nickel-chromium and cobalt-chrome.7 Metal posts, when subject to lateral forces, can cause root fractures.8 Non-metallic posts were developed to overcome this and provide more aesthetic restorations.9 The fibre reinforced composite (FRC) posts are prefabricated and made up of carbon fibre, quartz or glass fibres which are reinforced with a resin matrix (epoxy or methylacrylate resin) while the non-fibre reinforced composite posts can be ceramic or zirconia based.5 In FRC posts the modulus of elasticity is considered to be similar to a natural tooth, thereby reducing the stress concentration transferred to the root and the risk of root fracture.10
Although posts are still widely used, advances in adhesive technology mean they are now considered the last treatment option to retain a core.3
If a post does need to be placed, then guidelines do exist to aid post preparation.11 These include, ensuring the apical 4mm of gutta percha remains to preserve the integrity of the endodontic treatment and preserve apical health. The post should be at least as long as the crown
In addition to this, careful consideration needs to be given to the amount of remaining coronal tooth tissue. The term ferrule refers to a 360 degree collar of metal encircling parallel walls of tooth tissue which extend above the preparation margin.12 Several studies have shown that the ferrule plays an important role in the survival of the tooth and restoration as it distributes forces more evenly down the root.13,14 Studies suggest that between 1.5–2 mm of ferrule height can improve the fracture resistance of roots.15
Although such guidelines exist with regard to tooth preparation and remaining tissue, there is a dearth of evidence relating to different post materials and their indications for use.16 Clinical decision-making and reasoning is a cognitive process based upon the clinician's knowledge, experience and case contextual information.17 The clinical decision to place a particular type of post can be influenced by the available evidence base.18 Such research in this field largely comprises of in vitro laboratory studies, which have obvious shortcomings and have produced conflicting results.19 Therefore, it is not clear how and when dentists choose to place a post and what factors influence this. This can lead to the assumption that the decision is influenced by the individual clinician's knowledge, experience, training and the resources available.
A study by Morgano20 has been one of few that have looked into actual use and preference of post systems by practitioners. His findings indicate that non-clinical factors may have a greater effect on the use and selection of post systems than previously thought.20 Similarly, a cross sectional study of general dentists in Northern Ireland has investigated their opinions on the provision of posts, post materials and cementation techniques.21 The study concluded that dentists have a good understanding of the principles of restoring root filled teeth, but failed to investigate dentists' reasoning behind post selection.21
Historical studies from a decade ago showed that UK dentists seem to prefer cast posts over prefabricated ones, with precious alloy cast posts more popular than non-precious alloys (67% versus 37%).22 Regulations within the national healthcare system and limited knowledge of the advantages of prefabricated posts could explain these findings.22 However, there is no contemporary study to assess how newer techniques have been adopted in recent practice.
Aims
The primary aim of this study was to investigate the use of intra radicular posts and rationale for their selection by general dental practitioners (GDPs) and delegates attending a specialist prosthodontic conference.
The secondary aims were to investigate if any difference in the provision of post and core restorations exist amongst the two groups, the type of post and core system(s) being used, the rationale behind selection of a post system(s), and the effect of postgraduate training on the provision of post core restorations.
The null hypothesis was that there is no difference between general dental practitioners and delegates attending a specialist prosthodontics conference with regard to the use of intra-radicular posts to restore endodontically treated teeth.
Methods and materials
A twenty-two question survey was developed and piloted amongst GDPs and specialist staff in secondary care (University of Manchester Dental Hospital). Questions included demographic data, such as gender, years since graduation, type of clinical practice, postgraduate qualifications, and country of qualification. Six clinical scenarios were presented allowing participants to select their preferred post system for each given situation from a variety of options (see Table 1 for example of question and options available). The scenarios were based on teeth in the aesthetic zone and posterior segments, emulating commonly encountered clinical situations. Respondents had eight options per clinical scenario (Table 1) with a total of six scenarios (Box 1). In addition, respondents were also asked about their rationale for choosing the post systems they adopt in their clinical practice, along with cementation materials and experienced failures. Ethical approval was granted (Reference 13109) from the Research Ethics Committee of the University of Manchester.
The two groups of participants were GDPs attending monthly CPD evenings (September 2013 – November 2014) at the Manchester Dental Education Centre (MANDEC) and delegates attending the BSSPD (British Society of Prosthodontics) annual conference in 2014. All the attendees in both groups were included in the study and considered a sample of convenience. Surveys were handed out in person and no identifiable information was recorded rendering them anonymous.
Data collected was coded and entered into a statistics program (IBM SPSS version 2.0). Descriptive analysis was carried out on questions showing either percentiles or frequencies. Comparison of the two groups was carried out using a Chi-square test of independence. For cross tabulations with multiple groups, the Cramer's V result was considered. In situations where the number of cells with less than five exceeded 20%, Fisher's exact test was used. In those results that the number of cells with less than five did not exceed 20%, the Pearson Chi-squared result was considered. An alpha level of 0.05 was used for all statistical analysis.
Results
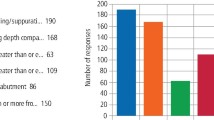
A total of 110 surveys were handed out to GDPs attending CPD seminars. Fifty-six were returned completed (there were no incomplete surveys handed in), giving a response rate of 51%. A total of 109 surveys were handed out to delegates attending the BSSPD conference and 53 were returned with a response rate of 49%. The demographic data is shown in Table 2.
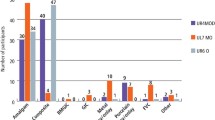
Fifty-percent of GDPs used both metal and non-metal post systems along with 72% of conference delegates in their clinical practice. Forty-five percent of GDPs exclusively used metal posts, compared to only 25% of conference delegates. Thirty-six percent of the GDPs placed posts on a monthly basis whilst 34% of conference delegates did the same (Figs 1 and 2)

Type of post system used

Frequency of post placment
In four out of six clinical scenarios, both groups preferred the use of cast metal post systems as the choice to restore the teeth. In the scenario involving a molar tooth, the majority of both groups selected Nayyar core technique as the preferred method of restoration (38% of GDPs and 44% of conference delegates). The only scenario in which the most popular selection differed was for the upper central incisor with a 4mm ferrule remaining. Thirty-nine percent of GDPs selected cast metal posts as the most preferred option to restore this tooth, whilst 31% of conference delegates preferred not to place a post.
There was no significant difference between the two groups with respect to post selection in any of the other clinical scenarios.
Analysis of responses to rationale behind post selection
GDPs selected ease of use and experience from previous clinical outcomes as the most common reasons to choose a particular post system. Conference delegates stated that experience from previous clinical outcomes was the primary reason for selecting a post system. Those that selected 'other' stated that the post system in use was the only system available in their clinical practice.
There was no statistically significant difference between the two groups with regard to the rationale behind selecting a post system.
Analysis on the effect of postgraduate training on use and selection of posts
The combined number of participants in both groups was 109; 36.7% had one or more postgraduate qualifications in dentistry whilst 63.3% did not. To assess if postgraduate training affected post use and selection, chi-squared test of independence was carried out with the following outcomes:
-
The relationship between these two groups regarding the preference of type of post system (that is, metal, non-metal or both) were significant with a P value of 0.009. This may indicate that postgraduate qualifications could have an impact on the selection of the post system material
-
The relationship between the two groups and post selection for different clinical scenarios showed a statistically significant difference in scenario 4 with a P value of 0.041, whilst the remaining scenarios did not indicate a significant difference.
Discussion
The results suggest there is no difference between the two groups with respect to their use and rationale for selecting post systems. The traditional metal systems still appear to be commonly used in this cohort despite the proposed advantages of non-metal systems.
The thought process behind post selection is relatively unknown. There was no statistically significant difference between the two groups for any reason for using a post. It was thought that cost or ease of use may have been important factors; given the demographics of the types of practices the two groups are in. The raw data however, does highlight that GDPs (who are predominately in mixed general practices) selected ease of use as the most popular reason for the post selection. The conference delegates (who are predominately in hospital practice) selected previous clinical experience as the most popular reason
The additional analysis on the effect of postgraduate education did yield a statistical difference. Whilst there appears to be a statistically significant relationship between the type of post system used and postgraduate qualification, it does not extend to the reasons behind the use of post systems. One clinical scenario involving an upper premolar tooth showed a significant difference but not the remaining five scenarios. Those that engage in postgraduate learning may show a difference in their post system and material choices. This is interesting, as a greater depth of knowledge can influence decision-making. It also highlights the importance of further education and keeping up to date with current concepts, particularly in light of Morgano's Kuwaiti based survey,23 which found most dentists, including specialists, were still adhering to outdated concepts.
It was noted that 25% of conference delegates were foundation trainees. This group of dentists, although present at the conference, usually attend as a part of their foundation training and may lack the experience to fully answer all the questions. A separate analysis without any foundation trainees, however, did not change the statistical outcome.
The sample population chosen may be a limitation in this study. The numbers of potential participants were dependent on the number of dentists attending both events. The potential variety of participants at each group was an unknown factor, as there was an unexpectedly high number of foundation trainees attending the BSSPD conference.
A survey with a larger sample size and more defined comparison groups may yield a more conclusive outcome. This could directly compare those on a prosthodontic, endodontic or restorative specialist list with general dental practitioners. A larger sample size can potentially be achieved by mailing out surveys to the groups of dentists using either electronic means or traditional postal methods. The effect of non-clinical factors such as age, geography, postgraduate qualifications and specialists training on post selection and use should be investigated further.
Conclusions
Within the limitations of this study it can be concluded that there is no difference between a sample of GDPs and delegates of a specialist prosthodontic conference regarding their use and rationale for post selection. Postgraduate qualifications appear to have an influence on the post selection.
References
Perel M L, Muroff F I . Clinical criteria for posts and cores. J Prosthet Dent 1972; 28: 405–411.
Chan R W, Bryant R W . Post-core foundations for endodontically treated posterior teeth. J Prosthet Dent 1982; 48: 401–406.
Ross I F . Fracture susceptibility of endodontically treated teeth. J Endod 1980; 6: 560–565.
Schwartz R S, Robbins J W . Post Placement and restoration of endodontically treated teeth: A literature review. J Endod 2004; 30: 289–301.
Goracci C, Ferrari M . Current perspectives on post systems: A literature review. Aust Dent J 2011; 56 (1 Suppl): 77–83.
Meyenberg K H, Lüthy H, Schärer P . Zirconia posts: a new all-ceramic concept for nonvital abutment teeth. J Esthet Dent 1995; 7: 73–80.
Rosenthiel S, Land M, Fujimoto J . Contemporary fixed prosthodontics. Mosby, 2001.
Bateman G, Ricketts D N J, Saunders W P . Fibre-based post systems: a review. Br Dent J 2003 195: 43–48.
Stewardson D . Non-metal post systems. Dent Update 2001; 28: 326–336.
Sidoli G E, King P A, Setchell D J . 1997. An in vitro evaluation of a carbon fiber-based post and core system. J Prosthet Dent 1997; 78: 5–9.
Sorensen J A, Martinoff J T . Clinically significant factors in dowel design. J Prosthet Dent 1984; 52: 28–35.
Sorensen J A, Engelman M J . Ferrule design and fracture resistance of endodontically treated teeth. J Prosthet Dent 1990; 63: 529–536.
Morgano S M . Restoration of pulpless teeth: Application of traditional principles in present and future contexts. J Prosthet Dent 1996 75: 375–380.
Eraslan O, Aykent F, Yücel M, Tolga, Akman S. The finite element analysis of the effect of ferrule height on stress distribution at post-and-core-restored all-ceramic anterior crowns. Clin Oral Investig 2009 13: 223–227.
Fokkinga W A, Kreulen C M, Bronkhorst E M, Creugers N H J . Up to 17 year controlled clinical study on post and cores and covering crowns. J Dent 2007; 35: 778–786.
Barfeie A, Thomas M B M, Watts A, Rees J . Failure mechanisms of fibre posts: a literature review. Euro J Prosthod Rest Dent 2015; 23: 3.
Groves M, Scott I, Alexander H . Assessing clinical reasoning: a method to monitor its development in a PBL curriculum. Med Teach 2002; 24: 507–515.
Soares C J, Valdivia A D, Silva G R D, Santana F R, Menezes Mde S . Longitudinal clinical evaluation of post systems: a literature review. Braz Dent J 2012; 23: 135–740.
Baba N Z, Golden G, Goodacre C J . Nonmetallic Prefabricated dowels: a review of compositions, properties, laboratory, and clinical test results. J Prosthodont 2009; 18: 527–536.
Morgano S M, Hashem A F, Fotoohi K, Rose L . A nationwide survey of contemporary philosophies and techniques of restoring endodontically treated teeth. J Prosthet Dent 1994; 72: 259–267.
Hussey D L, Killough S A . A survey of general dental practitioners' approach to the restoration of root-filled teeth. Int Endod J 1995; 28: 91–94.
Morgano S M, Bowley J F, Thalib L, Abdulkarim E . A survey of contemporary philosophies and techniques of restoring endodontically treated teeth in Kuwait. Med Princip Pract 2001; 10: 14–22.
Brunton P A, Christensen G J, Cheung S W, Burke F J T, Wilson N H F . Contemporary dental practice in the UK: indirect restorations and fixed prosthodontics. Br Dent J 2005; 198: 99–103.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Weerapperuma, I., Taylor, C. & Satterthwaite, J. A survey to compare the use and rationale for selection of intra-radicular posts among dental practitioners. Br Dent J 221, 635–638 (2016). https://doi.org/10.1038/sj.bdj.2016.861
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2016.861
