
Key Points
-
The prevalence of caries in children in England Wales and Northern Ireland has continued to decrease over the last decade.
-
Severe caries is increasingly concentrated in a minority of the population.
-
Living in Wales or Northern Ireland, being deprived, not attending for check-ups and drinking sugary drinks four or more times per day all increased the risk of having severe caries.
Abstract
Background The 2013 Children's Dental Health Survey is the fifth in a series of national surveys.
Aims To describe caries prevalence and severity and factors affecting these, in children in England, Wales and Northern Ireland in 2013.
Methodology A representative sample of children (aged 5, 8, 12 and 15 years) in England, Wales and Northern Ireland were invited to participate in dental examinations. Caries was measured at both the dentine ('obvious caries') and dentine plus enamel ('clinical caries') levels and analysis included identifying those with indicators of significant burden of caries and identifying predictive factors.
Results In 5-year-olds, 40% had obvious caries experience increasing to 56% when enamel lesions were included. In 15-year-olds, the respective figures were 46% and 63%. Fourteen percent of 5-year-olds and 15% of 15-year-olds had a least one indicator of significant levels of caries and those from deprived backgrounds were more likely to fall into this group.
Conclusions Overall, the prevalence of caries in children is continuing to decrease, but the rate is slowing. The level of disease for those with disease is much higher than the average values might suggest and there remain a sizeable minority with a significant burden of caries, associated with deprivation. This complex picture poses significant clinical and public health challenges.
Similar content being viewed by others


Introduction
The 2013 Children's Dental Health Survey (CDHS), is the fifth in a series of national surveys of children's oral health that have been carried out in the UK since 1973. The surveys have measured both clinical findings through a dental examination as well as behavioural and attitudinal information through a linked questionnaire. In 2013, 5-, 8-, 12- and 15-year-olds were included as with all previous surveys except 1973, when further age groups were also included. The 1983, 1993 and 2003 surveys included all four of the 'home nations' of the United Kingdom but for 2013 only England, Wales and Northern Ireland took part.
The decennial surveys are complementary to the UK-wide BASCD-coordinated NHS Epidemiology Programme of surveys (in England, the Public Health England, Dental Public Health Intelligence Programme - formerly the NHS Dental Epidemiology Programme) which occur with greater frequency and use larger samples but which, in any given survey, cover one individual age group and fewer conditions.1 The added value of the decennial surveys is in securing data from examinations and questionnaires of several age groups in one year across multiple conditions linked to behavioural and attitudinal data.
This paper examines one aspect of the clinical examination, caries. The clinical examination of the state of the dentition has formed a core through all of the surveys as caries is the most prevalent dental disease in childhood. The epidemiological investigation of caries in the UK remains important for policy makers, commissioners, dental public health practitioners and practising dentists in planning, delivering and evaluating dental services and public health interventions. The aim of this paper is to describe caries prevalence and severity in children in England, Wales and Northern Ireland, as well as factors influencing these, using data from the 2013 Child Dental Health Survey.
Methodology
Full details of sampling, response, examination protocols and statistical methods can be found elsewhere.2 The 2013 survey was based on a representative sample of children aged 5, 8, 12 and 15 years, attending government maintained and independent schools in the England, Wales and Northern Ireland. The survey involved 559 primary schools and 130 secondary schools. A total of 13,628 children were sampled within participating schools and asked to take part in a dental examination. In total 9,866 children were examined, a response rate of 70% for 5-year-olds, 65% for 8-year-olds, 83% for 12-year-olds and 74% for 15-year-olds. Twelve- and 15-year-olds were also asked to complete a questionnaire at the time of the survey and 99.6% did. Questionnaires were also sent to parents of examined children in all age cohorts and the response rate was 49% for parents of 5 and 8-year-olds, 39% for 12-year-olds, 34% for 15-year-olds, giving an overall response rate of 43%.
Clinical examinations
The main aspect of the methodology of interest to this paper is the examination of tooth status. Examinations were undertaken in school settings by 75 calibrated dentists.3 Consent was opt-in with parents opting children aged 5 and 8 years into the survey in advance of the examination day with opt-out for the child possible on the day and 12- and 15-year-olds opting in on the day with the possibility for parental opt-out in advance of the examination day. The examination was undertaken in a reclining chair using standardised dental epidemiological lighting, drying with cotton wool and visual examination, radiographs were not used. Dental nurses recorded the results of the examination on standardised forms.
Ethical approval
The survey was ethically reviewed (University College London, Project ID: 2000/003) following changes made as a consequence of piloting and it received a favourable ethical opinion.
Data analysis
In view of the complexity of the sampling design and resultant weighting procedures, sampling errors were quantified using the statistics programme STATA,4 and were calculated using a design factor (deft) to take account of the complex sampling and weighting procedures. The statistical significances of differences in means and percentages between sub groups were tested by calculating the confidence interval for the differences observed, based on the standard errors calculated using the design factor. This ensured that sampling error was taken into account in the testing procedure. Where statistically significant differences between groups are reported, the 5% threshold (p <0.05) was used.
Level of caries recorded
Typically in caries epidemiology in the UK, 'obvious' decay experience has been recorded, that is, caries into dentine. In the 1993 CDHS and previously, cavitated dentine lesions were recorded with the addition of non-cavitated dentine lesions (that is, shadowing) in 2003. In this 2013 survey, changes in enamel due to caries were also recorded both at a visual and cavitated level, termed 'clinical' decay experience (this is more in line with a clinical examination undertaken to plan individual patient treatment as it includes all grades of severity plus, in addition, initial stage decay for example, white spot lesions). This development in methodology is consistent with international developments in epidemiology over the last decade coordinated by the ICDAS Foundation5 and reflects the increasing emphasis of prevention at this level of disease. The different levels of recording now possible are illustrated in Figure 1 and clinical photographs of examples are shown in Figure 2. In essence, this means data can be reported at four hierarchical levels:
-
1
Obvious decay excluding visual caries (cavitated dentine caries)
-
2
Obvious decay including visual caries (cavitated and non-cavitated dentine caries)
-
3
Clinical decay excluding visual caries (cavitated enamel and/or cavitated and non-cavitated dentine caries)
-
4
Clinical decay including visual caries (cavitated and non-cavitated enamel and/or dentine caries).


Clinical photographs showing examples of the different levels of decay recorded (a) obvious decay excluding visual dentine caries, (b) obvious decay including visual dentine caries, (c) clinical decay excluding visual enamel caries, (d) clinical decay including visual enamel caries
For simplicity and to align with modern caries management, options 2 and 4 above are used most frequently. Where the term 'experience' is used, this includes currently decayed and unrestored teeth, restored teeth and for permanent teeth, teeth missing due to caries (that is, DMFT). Decay noted without the term 'experience' refers to the d/D component only. In line with previous surveys, examiners were not asked to determine the reasons for primary tooth loss and so teeth missing due to caries had to be determined as part of the analysis. For the published reports, all missing primary teeth were excluded from analysis and so caries experience figures were based on decayed and filled teeth (that is, dft). For this paper, further analysis has been undertaken and for 5-year-olds all missing primary teeth were counted as extracted due to caries to also give dmft results. For 8-year-olds, missing primary molars were counted as missing due to caries with primary incisors and canines assumed to have exfoliated. In both groups these widely used epidemiological assumptions are likely to produce a slight overestimate of caries.
Reporting of trends
Methodological differences between the surveys undertaken in each decade complicate the reporting of trends. Firstly, as outlined previously, the level of caries recorded has changed from survey to survey meaning that no trends can be reported in clinical decay experience and for obvious decay experience, trends back to 1993 or earlier will only include cavitated decay into dentine (trends from 2003-2013 are possible to compute for obvious decay including non-cavitated dentinal decay). Secondly, there were variations in the countries who took part in the surveys (1983, 1993 and 2003 surveys included England, Scotland, Wales and Northern Ireland; in 1973 and 2013 Scotland did not take part). This challenge has been managed in trend reporting by recalculating data from 2003 and before without Scotland.
However, the greatest difficulty in reporting trend data is, as has already been noted, related to the unavoidable changes required for consent in epidemiological surveys due to changing legal conventions and advice over the decades concerned. The consent for this survey was opt-in (or positive) whereas for previous decades the consent was opt-out (or negative). This has inevitably decreased the response rate for the examination phases, especially for 5- and 8-year-old groups where positive consent was required in advance from parents. It is very likely that this has introduced response bias, in that those not consenting may, for example, have a different and perhaps higher level of caries experience.6 It is not possible to determine the characteristics of those parents who did not consent, which in turn means that it is impossible to correct for these changes. This is more of a problem in the 5- and 8-year-old group and experience in other national dental epidemiology suggests that it is in primary teeth where the biggest effect of the bias is observed.7 Therefore, in the present survey trends can be reported for the permanent dentition of 12- and 15-year-olds (although some caution should be exercised in interpreting these) but are not reported for either the primary dentition of 5- and 8-year-olds or for the permanent dentition of 8-year-olds. For a fuller outline of the explanation of the discussion around the reliability of trend data, readers are referred elsewhere.3
Results
Decay experience in permanent teeth
Decay experience in 2013
Table 1 illustrates decay experience in permanent teeth in England, Wales and Northern Ireland in 2013. Almost two thirds of 15-year-olds and over half of 12-year-olds had clinical decay experience (that is, caries in enamel or dentine at both visual and cavitated levels, restorations or teeth missing due to caries). If only obvious decay experience (visual and cavitated caries into dentine, restorations or teeth missing due to caries) is considered, just under one half of 15-year-olds and one third of 12-year-olds were affected. The individual components of experience for 15-year-olds were: 21% had untreated decay (at obvious, or dentine level including visual and cavitated); 35% had restorations; 6% had missing teeth due to caries.
The mean number of teeth affected at the clinical decay experience threshold (including visual enamel caries) was 2.9 in 15-year-olds and 2.0 in 12-year-olds. At the obvious decay experience threshold (including visual dentine caries), this reduced to 1.4 and 0.8 respectively.
Overall 23% of 15-year-olds had sealants present. Mean numbers of teeth with obvious decay experience (including visual dentine caries) were 1.1 in children with sealants versus 1.4 in those without in England. In Wales the means were 1.9 versus 2.3 and in Northern Ireland 2.6 versus 3.7 respectively. These differences were statistically significant in Wales and Northern Ireland (p <0.05). In 15-year-olds, girls were statistically significantly more likely than boys to have obvious decay experience (49% contrasted with 43%) and those eligible for free school meals (a proxy for deprivation) were also statistically significantly more likely at both 12 and 15 years to have obvious decay experience (46% versus 30% at age 12 and 59% versus 43% at age 15) (p <0.05).
Obvious decay experience – trends in permanent teeth 1983–2013
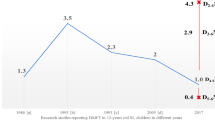
The trends in obvious decay (excluding visual dentine caries that is, cavitated dentine caries only) are illustrated in Figure 3 also showing the difference of including or excluding Scotland in 2003. It can be seen that for both 12- and 15-year-olds there has been a downwards trend in prevalence from 1983 to 2013 but that the rate of reduction has slowed considerably over the last decade. The difference in prevalence for obvious decay experience between 12- and 15-year-olds which has been a feature since 1983 has remained almost constant over the last decade at 15% in 2003 and 14% in 2013.

Percentage of 12- and 15-year-olds with obvious decay excluding visual dentine caries in permanent teeth (United Kingdom 1983 and 1993; England, Wales and Northern Ireland 2003-2013) reproduced from Pitts, Chadwick, Anderson2
In terms of mean number of teeth affected, for 15-year-olds, the figures for obvious decay experience (including visual dentine caries) were 1.4 in 2013 compared with 1.9 in 2003, for untreated dentine decay (visual and cavitated) 0.5 in 2013 and 0.8 in 2003, for restored teeth 0.8 in 2013 and 1.1 in 2003 and for missing due to decay 0.1 in both 2013 and 2003. This gives a restorative index (mean no. of restored teeth divided by mean no. of teeth with obvious decay experience) of 57% in 2013 compared with 58% in 2003.
The burden of decay and associated factors
With the reducing prevalence of caries, the caries burden is concentrated in a smaller proportion of the population. This means that those with no detectable signs of obvious decay (including visual dentine caries), ie DMFT = 0, skew the mean number teeth affected. It is therefore useful to look at mean numbers of teeth in those with caries (that is, DMFT >0). Table 2 shows mean numbers of teeth affected both for the whole sample and for those with DMFT >0, illustrating, for example, that for 15-year-olds those with DMFT >0 had a mean number of teeth with obvious decay experience (including visual dentine caries) of 3.1 compared to 1.4 in the whole sample.
In this survey children with a severe or extensive caries burden have been defined as those who exhibit one or more of five specific conditions:
-
Five or more teeth with obvious decay experience (DMFT >5)
-
Three or more teeth with untreated dentine caries (D >3)
-
Any severely carious teeth that are deemed to be involving the pulp
-
Any evidence of sepsis using the PUFA examination (open pulp, ulceration related to sepsis, fistula, abscess)
-
Loss of any permanent tooth due to caries.
For 15-year-olds, 15% had at least one of these conditions. Table 3 reports the percentage with each of the conditions and also considers these by sex and eligibility for free school meals. There was little difference by sex, but among those eligible for free school meals children were at least twice as likely to present with one or more of the conditions.
In addition a logistic regression model was constructed to investigate associations of having one or more of the severe caries burden markers with behaviours identified from self-completion questionnaires. The following variables were included: sex, country of residence (England, Wales or Northern Ireland), eligibility for free school meals, Output Area Classification (OAC - This classification groups small areas based on similarities across a variety of 2011 census indicators covering demographic composition, household composition, housing, socio-economic status and employment8), frequency of tooth brushing, pattern of dental attendance, frequency of consuming sugary drinks, frequency of consuming fruit juice and smoothies, frequency of consuming water, experience of smoking and experience of drinking alcohol. The final model showed that the following factors were all associated with increased risk of having one or more markers of severe decay (odds ratios in parentheses): living in Wales or Northern Ireland (1.87, 3.91); being eligible for free school meals (1.99); never attending the dentist (2.55) or only attending when in trouble (2.99); consumption of sugary drinks four or more times per day (2.13); whereas consuming water four times or more per day reduced the risk (0.59). The full details of the model and results are reported elsewhere9.
Decay experience in primary teeth
Decay experience in 2013
Table 4 illustrates decay experience in primary teeth in England, Wales and Northern Ireland in 2013. Over one half of 5- and 8-year-olds had clinical decay experience (that is, caries in enamel or dentine at both visual and cavitated levels or restorations or teeth missing due to caries). For obvious decay experience (visual and cavitated caries into dentine or restorations or teeth missing due to caries), 40% of 5-year-olds and just under one half of 8-year-olds were affected. The individual components of experience for 5-year-olds were 28% had untreated decay (at obvious, or dentine level including visual and cavitated), 8% had restorations and 13% had teeth missing due to decay.
The mean number of teeth affected at the clinical decay experience threshold (including visual enamel caries) was 2.0 in 5-year-olds and 2.1 in 8-year-olds. At the obvious decay experience threshold (including visual dentine caries), this reduced to 1.2 and 1.5 respectively. In 5- and 8-year-olds, there was no significant difference in obvious decay experience between boys and girls but those eligible for free school meals (a proxy for deprivation) were significantly more likely to have obvious decay experience at both 5 (52% versus 37% of those not eligible) and 8 years(64% versus 46% of those not eligible). The restorative index in 5-year-olds was 16.7%.
The burden of decay and associated factors
The mean number of teeth with obvious caries experience (decay into dentine, both visual and cavitated but excluding missing teeth) in those with any obvious caries experience (that is, dft >0) was 3.0 at both 5- and 8-years-old. The mean number of teeth with untreated caries (at dentine level including visual and cavitated) in this group at 5 years old was 2.6, with the mean number of restored teeth being 0.4.
As with permanent teeth, the survey identified those with a high burden of caries by looking at children with at least one of four specific conditions (loss of any permanent tooth was not included). For 5-year-olds, 14% had at least one of these conditions. Table 5 reports the percentage with each of the conditions and also considers these by sex and eligibility for free school meals. It can be seen that boys and those eligible for free school meals were just under twice as likely to have one or more of the conditions.
Discussion
This survey provides a unique opportunity to look at oral health and disease of children in the UK over several decades and link clinical data to behavioural and attitudinal data. This paper has focused on one disease, caries. Unavoidable changes in methodology relating to consent mean that trends cannot be reliably described for caries in the primary dentition but trends have been explored for the permanent dentition of both 12- and 15-year-olds. Relating to caries, the major new development for the 2013 survey was the inclusion of enamel caries in the examination process, a development which reflects changes in practice towards increasingly preventive intervention for such disease. However, this change has not precluded the presentation of results at different thresholds to allow restorative need to be described and to allow comparison of trends where earlier surveys used less sensitive levels of caries severity.
Although it is very encouraging to see a continued overall decrease in the mean prevalence of caries in all age groups, the rate of decline has slowed considerably. In addition, although the burden of caries in those with caries has decreased, the reduction has been small, there are many children and young people with caries and the survey has identified, for the first time, a group of around 15% of the sample, with a very significant burden of caries. Unsurprisingly, associations were observed between having significant burden of caries and deprivation (as described by eligibility for free school meals), as well as irregular dental attendance, sugary drink consumption and living in Wales and Northern Ireland (who have traditionally experienced higher levels of caries than England). There was also an association between having sealants and a lower mean number of teeth with caries experience in Northern Ireland and Wales. This effect may not be apparent in England due to the lower prevalence of decay and mean number of teeth affected.
The results pose several challenges for the profession. Firstly we must ensure we have appropriate systems to clinically manage those with a significant level of disease. There are questions over how such levels of disease should be managed, where they should be managed and by whom. Secondly, reducing the size of this potentially 'resistant' residual group with a high burden is a difficult problem that will require a coordinated public health approach as well as individual tailored preventive interventions. Finally, we should not forget the significant number with very early levels of caries (two thirds of 15-year-olds have caries into at least enamel) and the other challenges in terms of how to keep these children and those who have no caries detectable in this survey healthy and ensure that initial-stage caries does not progress. In trying to address these problems, the biggest challenge may be ensuring that inequalities do not increase further if those already doing well respond better to any interventions than those who have higher disease burdens.
Conclusions
The 2013 Child Dental Health Survey shows that prevalence of caries of children in England, Wales and Northern Ireland is continuing to decrease but the rate is slowing. Due to the shift in the distribution of caries in the population, the level of disease for those with disease is much higher than the average values might suggest. There also remain a sizeable minority with a significant burden of caries and unsurprisingly, deprivation is associated with this group. There are significant challenges both at clinical and public health level in terms of maintaining the healthy and addressing those with significant burdens of this largely preventable disease.
References
Public Health England. Dental Public Health Intelligence Programme, 2015. Available at http://www.nwph.net/dentalhealth/ (accessed October 2015).
Pitts N B, Chadwick B, Anderson T . Children's Dental Health Survey 2013. Report 2: Dental Disease and Damage in Children England, Wales and Northern Ireland. London: Health and Social Care Information Centre, 2015.
Anderson T, Thomas C, Ryan R, Dennes M, Fuller E . Children's Dental Health Survey 2013 Technical Report England, Wales and Northern Ireland. London: Health and Social Care Information Centre, 2015.
StataCorp. Stata Statistical Software: Release 11. 11th ed. College Station, TX StataCorp LP, 2009.
Pitts N B, Ekstrand K R . International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS) methods for staging of the caries process and enabling dentists to manage caries. Community Dent Oral Epidemiol 2013; 41: e41–e52.
Monaghan N P, Jones S J, Morgan M Z . Do parents of children with caries choose to opt out of positive consent dental surveys in Wales? Br Dent J 2011; 210: E1.
National Health Service (General Dental Services Contracts) Regulations, Stat. 3361 (1 January 2006).
Office for National Statistics. 2011 Area Classifications, 2011. Available at: http://webarchive.nationalarchives.gov.uk/20160105160709/http://www.ons.gov.uk/ons/guide-method/geography/products/area-classifications/ns-area-classifications/ns-2011-area-classifications/index.html (accessed July 2015).
Steele J G, White D, Rolland S L, Fuller E . Children's Dental Health Survey 2013 Report 4: The Burden of Dental Disease in Children England, Wales and Northern Ireland. London: Health and Social Care Information Centre, 2015.
Pitts N . 'ICDAS'an international system for caries detection and assessment being developed to facilitate caries epidemiology, research and appropriate clinical management. Community Dent Health 2004; 21: 193–198.
Pitts N B, Harker R . Obvious decay experience: Children's Dental Health in the United Kingdom 2003. London: Office of National Statistics, 2005.
Selwitz R H, Ismail A I, Pitts N B . Dental caries. Lancet 2007; 369: 51–59.
Acknowledgements
The authors wish to thank the children and young people who took part in the research as well as their parents and guardians. In addition the authors express gratitude to the dental examining teams, field workers from the Office for National Statistics, staff in the schools visited and the individuals involved in the consortium for their invaluable contributions. The 2013 CDHS was commissioned by the Health and Social Care Information Centre (HSCIC) and the research was carried out by a consortium led by the Office for National Statistics. We particularly extend our thanks to Tom Anderson of the ONS Social Survey Division and the wider ONS research team. CRV was funded by a Clinical Lecturership and subsequently a Clinician Scientist award both supported by the National Institute for Health Research during this independent research. The views expressed in this publication are those of the authors and not necessarily those of supporting organisations.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Vernazza, C., Rolland, S., Chadwick, B. et al. Caries experience, the caries burden and associated factors in children in England, Wales and Northern Ireland 2013. Br Dent J 221, 315–320 (2016). https://doi.org/10.1038/sj.bdj.2016.682
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2016.682
This article is cited by
-
Knowledge and attitudes toward evidence-based cariology and restorative dentistry among Egyptian dental practitioners: a cross-sectional survey
BMC Oral Health (2023)
-
Trends in dental caries of deciduous teeth in Iran: a systematic analysis of the national and sub-national data from 1990 to 2017
BMC Oral Health (2022)
-
Dental caries at enamel and dentine level among European adolescents – a systematic review and meta-analysis
BMC Oral Health (2022)
-
Unmet need in Sierra Leone: a national oral health survey of schoolchildren
BDJ Open (2022)
-
Dental caries thresholds among adolescents in England, Wales, and Northern Ireland, 2013 at 12, and 15 years: implications for epidemiology and clinical care
BMC Oral Health (2021)
