
Key Points
-
Suggests that dental practice should be the prime location for clinical dental research.
-
Discusses patients concerns regarding which dental materials are used.
-
Demonstrates that patients care strongly that the materials are of a high quality and have been thoroughly researched.
Abstract
Aims It is the aim of this study to determine, by means of a questionnaire completed by patients attending ten UK dental practices, patients' level of knowledge on dental materials and techniques.
Materials and methods Members of The PREP (Product Research and Evaluation by Practitioners) Panel were asked to recruit patients to participate in a questionnaire-based assessment of their knowledge of dental materials.
Results Two hundred and forty-nine patients took part in the questionnaire. Sixty-three percent (n = 157) of the respondents were female and 92% (n = 229) of the respondents stated they were regular attenders at the dental practice. The respondents were asked how important the quality of dental materials used in their mouth was, and on a Visual Analogue Scale (VAS) where 1 = not important and 10 = very important, the result was 9.6. The same score was recorded when they were asked how important it was that the materials used in their mouth were supported with relevant clinical research evidence and long term data of the success of the material. They were also questioned on the subjects of price, manufacturer, source or material and type of filling material. A significant amount of respondents demonstrated that they had concerns over the use of amalgam.
Conclusions Respondents expressed strong views that the materials used on their teeth should have a robust evidence base and they care about the materials that are used in their mouths.
Similar content being viewed by others

Introduction
Practice-based research
A majority of research into the effectiveness of dental materials is carried out in dental hospitals or other academic institutions, rather than in general dental practice, even though this is where the majority of dental treatment is performed, worldwide. Reasons for this divergence include the potential cost, given that practices are geared to the efficient treatment of patients rather than research. The training of general practitioners in research methods may also be incomplete. However, there are many reasons why dental practice increasingly should become the prime location for clinical dental research. Principal among these is that dental practice is the real world.
Patients have also been found to be approving of practitioner involvement in research, with the practice and practitioner's professional image being enhanced.1
A UK-based group of practice-based researchers is the PREP (Product Research and Evaluation by Practitioners) Panel. This group was established in 1993 with six general dental practitioners, and has grown to contain 33 dental practitioners located across the UK and one in mainland Europe. It has completed over 60 projects – 'handling' evaluations of materials and techniques, and more recently, clinical evaluations (n = 9) of between one year and 5 years.2
Patient knowledge
Where do patients find information on dental materials and techniques? It could be considered that, in order of decreasing reliability, patients may glean information from the following sources:
-
from members of the dental team either by word of mouth; from patient information leaflets written by the dentist and available in the practice; from the dental practice web site; or from instructional videos made by the practice
-
from the media (some newspapers run regular features on health, including dental health)
-
from the Internet (which is certainly not peer reviewed).
However, there appears to be a paucity of information on whether patients actually have any knowledge of the materials that their dentist is using in their mouth. It is, therefore, the purpose of this study to determine, by means of a questionnaire administered to patients who are attending for a dental examination or treatment, the level of knowledge that a group of regularly attending patients have regarding dental materials and techniques.
Materials and methods
Selection of clinicians
All members of the PREP Panel (n = 33), each of whom have previous experience in practice-based research, were asked, by means of an explanatory letter, if they would be prepared to recruit 25 patients to participate in a questionnaire-based assessment of patients' knowledge of dental materials. Of those who responded positively (n = 22), ten members were selected.
Questionnaire design
A questionnaire was designed to determine the views of patients who elect to participate, with the questionnaire following the guidelines set out in the Total Design Theory by Don Dillman3 which has been considered to produce meaningful results. This, along with the protocol, were sent to the PREP Panel participants for their comments, and amendments made according to their suggestions.
Selection of patients
The participating dentists, along with their staff (in particular, the practice receptionist and nurses), were asked to advertise that they were carrying out a study on patients' knowledge of dental materials and techniques. In this regard, participating practices were provided with a practice information leaflet (principally advising that completion of the questionnaire would take no longer than five minutes of their time) and an advertisement which they were asked to display in the reception area. Those who indicated an availability to take part were provided with an information leaflet and were asked to sign a consent form. They were given the questionnaire to complete in the waiting room following their treatment visit. Participating patients were reimbursed with a £5 high street voucher plus a 'goody bag' containing oral healthcare products.
Ethical standards
The protocol was sent to the Chair of a local ethics committee (West Midlands), who considered that application for full ethical approval was not indicated. Informed written consent was, nevertheless, obtained from all patients before registration for participation in the evaluation.
Results
The practices which were selected to participate were situated in Birmingham, Buxton, Portishead, Stockport, Southampton, Stourbridge & Wilmslow (all England), Coleraine and Holywood (both N Ireland), and Kyle of Lochalsh (Scotland).
A total of 249 satisfactorily completed questionnaires were received. It should be noted that, as a result of incomplete responses to some questions, the responses do not always total 249.
Demographic data
The results regarding demographic data were as follows:
-
63% (n = 157) of the respondents were female.
-
92% (n = 229) of the respondents stated they were regular attenders.
The age distribution of the respondents was as follows:
-
Less than 20 years – 9 respondents (4%)
-
21-35 years – 23 respondents (9%)
-
36-50 years – 71 respondents (28%)
-
51-65 years – 91 respondents (37%)
-
Over 65 years – 55 respondents (22%)
Patients' views
Results in relation to patients' views on dental materials are as follows, with the inclusion of unsolicited comments which were considered relevant:
When the respondents were asked how important the quality of dental materials used in their mouth was, on a VAS where 1 = not important and 10 = very important, the result was 9.6.
The respondents were asked how important it was that the materials used in their mouth were supported with relevant clinical research evidence and long term data of the success of the material, on a VAS where 1 = not important and 10 = very important, with the result being 9.6.
When the respondents were asked to state, on a VAS where 1 = not important and 10 = very important, how important it was that your front teeth looked good, the result was 9.5
The respondents were then asked how important it was, on a VAS where 1 = not important and 10 = very important, that they had tooth-coloured fillings in their back teeth, with the result being 7.6.
When asked if their dentist gave the patient a choice of materials when having a procedure carried out, 64% of respondents (n = 157) stated that they were and 36% (n = 89) said that they were not.
The respondents were asked if they expected the dentist to use the same dental product on NHS and private patients, with 56% (n = 137) stating 'Yes' and 44% (n = 108) answering 'No'.
The respondents who replied 'No' to the above question were then asked if they expected the products used on NHS patients to be cheaper than those used on private patients, with 91% (n = 98) answering 'Yes' and 9% (n = 10) answering 'No'
When the respondents were asked if they expected the filling materials used by the dentist to have clinical research data to support their use as a dental product 99% (n = 240) answered 'Yes' and 1% (n = 2) answered 'No'.
Comment: 'No research on animals'
The respondents were asked if they expected the filling materials used by the dentist to come from a manufacturer experienced in the development and manufacture of dental products, with 99.5% (n = 242) answering 'Yes' and 0.5% (n = 1) answering 'No'.
When the respondents were asked if they would be happy for their dentist to use 'own label' products, (in the same way that some supermarket chains sell their 'own label' beans, for example) not made by a recognised manufacturer of dental filling materials,
43% (n = 102) answered 'Yes' and 57% (n = 138) answered 'No'.
Comment:
-
'Yes – if own label materials identical'
-
'Unsure – depends on quality'
-
'Only if supported by research evidence'
The respondents were asked if they were concerned about the source of the dental filling materials used on them, with 48% (n = 117) answering 'Yes' and 52% (n = 126) answering 'No'.
When the respondents were asked if they trusted the dentist to purchase the best products for use on their teeth, 98% (n = 240) answered 'Yes' and 2% (n = 5) answered 'No'.
The data were divided into two groups in order to assess whether differences were apparent in males vs females and older vs younger patients. These results are presented in Tables 1 and 2.
Regarding male vs female, males:
-
were not so concerned about tooth coloured fillings in back teeth
-
had a greater expectation of NHS materials being cheaper
-
seemed more concerned about the source of materials
-
had fewer anxieties about the use of amalgam
Regarding age, the patients were subdivided into <50 years and 51+ years. It was apparent that: there were more regular attenders in the over 51 age group; the 51+ age group rated importance of tooth coloured fillings in back teeth slightly higher; and the 51+ age group was less happy to have their dentist use 'own brand' materials, while the <50 group was less concerned about the source of these materials. There was no difference about the source of knowledge, although the younger group appeared happier to use the internet.
Finally, the respondents were asked if they had any anxieties concerning the use of amalgam (silver fillings) in their teeth, with the following result 31% (n = 74) answering 'Yes' and 69% (n = 163) answering 'No'.
Comments made by those with concerns essentially fell into two groups, namely, (a) on health grounds (a total of 46 comments) and (b) on cosmetic grounds (n = 18).
(a) Some health-related comments:
-
'Implications on other health aspects' (17)
-
'Mercury – heavy metal' (2)
-
'I presume white fillings safer'
-
'I presume amalgam may contain hazardous material'
-
'I suffer from migraines and it doesn't help'
-
'Mercury content not healthy' (3)
-
'I would not have amalgams in mine or my children's teeth – not anxiety just a refusal'
-
'Chemicals in the product'
-
'Concern over toxic elements, ie Mercury' (3)
-
'Not happy to have amalgam'
-
'Unpleasant taste' (2)
-
'Negative health implications reported in the press? Alzeimah's' (sic)
-
'Leaks mercury into my body' (3)
-
'Don't want it in my mouth'
-
'Concerns with links to long term memory loss'
-
'Unnecessary to use'
-
'Harmful – I use organic products as much as possible'
-
'Not known for sure what is in silver fillings, there could be other metals which over time damage your mouth'
(b) Some cosmetic-oriented comments:
-
'They look awful/appearance' (9)
-
'Look ugly'
-
'Don't want silver fillings' (2)
-
'They look obvious'
-
'Do not look attractive' (2)
-
'Rather have a white filling' (6)
The respondents were asked to tick the name of dental material/equipment manufacturers that they had heard of, with the results presented in Table 3.
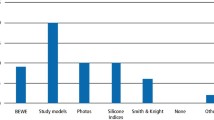
If the respondent knew any of the names mentioned in Table 3, they were then asked to indicate the source of their knowledge from the list as presented in Table 4. Final comments included:
-
'I trust my dentist & expect him to advise on all matters in this survey' (14 similar)
-
'Very pleased that my practice is taking part in research – this shows an innovative practice – Well done'
-
'Would like fillings that don't fall out'
-
'I am more concerned about the quality of materials used than frequency of check-ups'
-
'I rely on British products which have been well tested & suitable for purpose'
-
'Interesting survey'
Discussion
This paper presents work on patients' knowledge of dental materials and techniques, which may be considered relevant as we move toward an era of patient centred care. To the authors' knowledge, such work has not been previously been carried out on a UK-wide scale. The results indicate that the patients in the survey had well-considered views on the quality of materials that they expected from their clinicians, perhaps not what many might have believed, with the overwhelming majority expecting their dentist to use good, evidence-based materials for their treatment. This would appear to indicate patient trust in their dentists and in the profession as a whole.
The results also indicated that patients considered that it was important that their anterior teeth looked good, not a surprise when the impact of so-called aesthetic (or cosmetic) dentistry today is considered. On a VAS scale, the importance of good aesthetics of anterior teeth scored 9.6 out of 10.0, while the importance of good aesthetics of posterior teeth scored 7.6. Given that we have no baseline for comparison from the past, it is not known whether this figure is higher than it would have been in the past. However, in 2004, the growth in tooth-coloured restorations for posterior teeth was noted in a study of materials used worldwide4 and it could be considered surprising if this trend had not continued until the time of the present study. It may also be considered surprising that the 51+ age group rated importance of tooth coloured fillings in back teeth slightly higher than in younger patients, especially in light of the 1991 study by Burgersdijk and colleagues5 in which older patients were less aware of the treatments which their dentist could carry out to improve the appearance of their teeth. However, it might be that opinion has changed since the publication of that study.
Regarding whether they were offered any choice of material for the restoration of their teeth, 64% of respondents responded that they were (that is, 36% were not) – perhaps surprising in this age of increasing patient empowerment. It was also interesting to note that, when asked if they expected the dentist to use the same dental product on NHS and private patients, 56% responded 'Yes'. Herein lies the ethical dilemma for the practicing clinician who has to balance the need to make a 'profit' to pay his/her salary and that of his staff within the fee structure within which (s)he is operating. In this regard, it is interesting to note that, of the respondents who did not expect their dentist to use the same material for NHS and private patients, 91% expected the products used on NHS patients to be cheaper than those used on private patients.
Overwhelmingly, the respondents expected their dentist to purchase the best products for use on their teeth, and, similarly, the respondents expected the filling materials used by the dentist to come from a manufacturer experienced in the development and manufacture of dental products, with only one respondent not considering that this was necessary and only two not expecting the filling materials used by the dentist to have clinical research data to support their use. It could be considered that the patient respondents to this survey displayed an excellent insight into the concept of evidence-based dentistry: what is not known is the source of this knowledge, but it could be considered likely that their dentist had discussed this concept with the patients, a refreshing notion. Patients also expressed a strong opinion on whether they considered that 'own label' versions of dental materials should be used on their teeth, with 43% of patient respondents considering that they would not wish an 'own label' product, not made by a recognised manufacturer of dental filling materials, to be used on their teeth. This appears to validate comments made in the past concerning the use of such materials.6,7,8 Patients would not necessarily be aware of the fact that such 'own label' products are bereft of an evidence base for their effectiveness9,10 and the fact that a material researched and developed by a reputable manufacturer is more likely to have an evidence base.2
Regarding amalgam restorations in posterior teeth, 31% of the patient respondents expressed anxiety regarding the use of amalgam fillings in their teeth. Comments were made by 66 patients, principally those who had worries regarding amalgams on health grounds. Where these comments arose from is not apparent from the present work, but it places patients outwith current thinking regarding the safety of dental amalgam which has been demonstrated to be satisfactory in an extensive review by Wahl,11,12 in which it is apparent that the literature does not support worries that the use of dental amalgam may lead to diseases such as multiple sclerosis, Alzheimers disease, and others. However, despite these expressed worries, patients should be reassured that a reduction in use of dental amalgam use is under way, having been part of the Minamata Convention, signed by 147 countries, including the UK, in October 2013.
It is gratifying to note that the respondents' dentists were the second rated source of knowledge, following advertising, and that, given that almost all patient respondents knew the name of two toothpaste brands, it may be assumed that it was those that they were thinking of when they rated advertising as the premier source of dental information. It is apparent that some companies are better at promoting their brand than others, with the best being the toothpaste manufacturers, unsurprising since their products are principally sold in shops, pharmacies and supermarkets, in contrast to dental materials. It could be considered, however, that is the advertisers' job. On the other hand, is it not also the dentists' job too?
Does the study present a view of the 'typical' patient in the UK? Perhaps, perhaps not! The majority of respondents were a convenience sample of regular attenders, who could, therefore, be considered to be well motivated towards maintaining their oral health. The work does, however, present an initial view on the degree of knowledge that patients have concerning dental materials and what they expect from their dental clinician.
Finally, the results of this study indicate that more consumer research is indicated if the dental profession is going to rise to the challenge of shifting to patient-centred care. The question could be asked – how does what a patient needs to know differ from what a dentist needs to know? It is apparent, from the results of this survey, that patients wish their treatment to be evidence-based, something with which clinicians would concur. However, there are occasions, with a newly introduced material of technique, where there will be no clinical evidence base for that material. The dentist then has to assess whatever laboratory data which is available and make an informed decision, or even a 'leap of faith.' In this regard, if dentist and patient were to be totally evidence-based, then neither would ever accept a novel treatment. Ninety-eight percent of patient respondents trusted their dentist to purchase the best products for their teeth, something that a dental professional would be expected to do. However, the principal disconnect related to the results of the present work is that 99.5% of patient respondents wanted their materials to be from a manufacturer experienced in dental manufacturing, yet only 48% of respondents stated that they were concerned about the source of the dental filling materials used on them and 43% being content to have 'own label' materials used for their treatment, despite these having, at best, a scant evidence base.9,10 This is apparently an area in which the patients responding to this survey were not well versed.
Conclusions
Patients responding to a questionnaire expressed strong views that the materials used on their teeth should have a robust evidence base, expecting their dentist to use materials that were produced by a manufacturer with experience in the field. They do appear to care about the materials that we use in their mouths. Almost half did not wish 'own label' materials to be used in their mouths and one third of respondents expressed anxieties regarding the use of amalgam in their teeth.
Commentary
In developing and providing patient-centred care, it is important, among other requirements, to understand the attitudes, expectations and anxieties of patients.
The practice-based assessment reported by Burke and Crisp provides what is considered to be first in the literature 'consumer' data on dental materials and restorative approaches. These data were collected by means of a questionnaire administered by ten PREP (Product Research and Evaluation Practitioners) members with a wide geographic distribution across the UK. The findings are based on responses included in 249 completed questionnaires.
Notwithstanding the acknowledged limitations of the relatively limited assessment, involving a 'convenience sample of regular (dental) attenders', the findings indicate that patients may be found to have well-considered views on the quality of the materials they expect to be used in the provision of their dental treatment. All but a few respondents indicated that they expect, or possibly trust their dentist to use 'good quality, evidence-based materials' produced by reputable manufacturers with recognised credibility in the field. Almost half of the respondents indicated that they would not wish 'own brand' materials placed in their mouths. Also, one third of the respondents – more females than males – expressed one or more largely unfounded anxieties about the possibility of dental amalgam being used as a restorative material in their mouth. Otherwise, differences in responses from male and female respondents, and respondents in different age groups (<50+ >51+ years of age) were small – some interesting, others possibly surprising. The source of the respondents' knowledge of dental materials and manufacturers of dental materials was principally advertising, followed by their dentist. Dental manufacturers with over the counter products were found to be best known among the respondents.
Burke and Crisp suggest that 'more consumer research is indicated if the dental profession is going to rise to the challenge of shifting to patient-centred care', posing the question: 'How does what a patient needs to know differ from what a dentist needs to know?' In addressing this question, directed at both the profession and dental industry, manufacturers of dental materials may have to consider greatly increasing marketing to patients, and dentists may need to find ways to reassure patients that they will be using the best materials for proposed treatments.
N. H. F. Wilson Professor of Dentistry King's College London Dental Institute, King's College London
Author questions and answers
1. Why did we undertake this research?
This research was undertaken because there was a dearth of information regarding patient attitudes to, and knowledge of, the materials that their dentists used for their treatment. In this era of increasing patient autonomy, it seemed relevant to discover whether patients actually had opinions on and knowledge of the materials that were being used in their treatment.
2. What would we like to do next?
The present work was carried out on a sample which consisted principally of regularly attending patients, with the results indicating a high degree of interest in the materials that were used, with the volume of health-related comments being a surprise to the authors. It would be interesting to continue this work with a larger sample, perhaps not consisting of regular attendees, or to interview a number of patients in an effort to tease out the reasons for the responses that they made.
References
Burke F J T, McCord J F . Research in dental practice – problems and solutions. Br Dent J 1993; 175: 396–398.
Burke F J T, Crisp R J . Twenty years of handling evaluations and practice-based research by the PREP Panel. Dent Update 2013; 40: 339–341.
Dillman D A . Effects of questionnaire length, respondent-friendly design and a difficult question on response rates for occupant-addressed census mail surveys. Pub Opin Quart 1993; 57: 289–304.
Burke F J T . Amalgam to tooth-coloured materials – implications for clinical practice and dental education: governmental restrictions and amalgam-usage survey results. J Dent 2004; 32: 343–350.
Burgersdijk R, Truin G-T, Kalsbeek H, van'Hof M, Mulder J . Objective & subjective need for cosmetic dentistry in the Dutch population. Comm Dent.Oral Epidemiol 1991; 19: 61–63.
Burke F J T . Me too. Dent Update 2010; 37: 137.
Burke F J T . Me too 2. Dent Update 2011; 38: 586–592.
Christensen G J . Are you using “grey market” or counterfeit dental products? J Am Dent Assoc 2010; 141: 712–713.
Mickenautsch S . How well are current GIC product labels related to current systematic review evidence? Dent Update 2011; 38: 634–644.
Burke F J T . The evidence base for “own label” resin-based dental restoratives. Dent Update 2013; 40: 5–6.
Wahl M J . Amalgam – resurrection and redemption. Part 1: The clinical and legal mythology of anti-amalgam. Quintessence Int 2001; 32: 525–535.
Wahl M J . Amalgam – resurection and redemption. Part 2: The medical mythology of anti-amalgam. Quintessence Int 2001; 32: 696–710.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Burke, F., Crisp, R. A practice-based assessment of patients' knowledge of dental materials. Br Dent J 219, 577–582 (2015). https://doi.org/10.1038/sj.bdj.2015.956
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2015.956
