
Key Points
-
Explores the working patterns of male and female specialist orthodontists in the United Kingdom.
-
Outlines various factors which may influence their working patterns.
-
Discusses potential significance this may have for future workforce planning.
Abstract
Objective To describe factors which influence the current working patterns of orthodontists in the United Kingdom.
Design and setting A cross-sectional postal questionnaire to orthodontic specialists in the United Kingdom.
Subjects All those on the specialist list in orthodontics held by the General Dental Council in 2006-2007.
Materials and methods The data gathered included demographic details (gender, ethnicity, age, professional status and number of children), calendar year of achieving professional qualifications and current working patterns, together with details of any career breaks taken and geographical location of work.
Results The response rate was 81.5%. Male and female orthodontists were seen to have different working patterns. The difference was statistically significant with male orthodontists undertaking clinical work on average 1.5 sessions more per week than their female colleagues. The calendar year of completion of undergraduate studies and the number of children an orthodontist has can significantly affect the number of clinical sessions they work each week. In recent years it has been observed that there is greater ethnic diversity among the workforce but ethnic origin appeared to have a minimal effect on the number of clinical sessions worked each week. The amount and length of career breaks taken by female orthodontists was greater than their male colleagues. In addition, there continues to be an uneven distribution of orthodontists throughout the United Kingdom.
Conclusion Many factors influence the current working patterns of orthodontists in the United Kingdom. However, it may be the inequitable regional distribution of orthodontists throughout the United Kingdom which is of greatest significance to orthodontic workforce planning for the future.
Similar content being viewed by others

Introduction
The provision of an optimal orthodontic service depends on achieving a balance between the needs and demands of the population and the supply of workforce personnel.1 However, this is not straightforward as there continues to be a growing demand for orthodontic treatment while the workforce supply depends not only on the number of orthodontists entering and leaving the workforce but also on current working patterns.2,3
Many factors are believed to affect working patterns4 and it is evident that having children can impact on the number of hours a clinician spends at work.2,3,4,5,6,7 In addition it is known that more female dental practitioners work part-time2,4,5 and take career breaks2,3 than their male colleagues. Thus it is speculated that 'feminisation' of the dental8,9 and orthodontic10 workforces may affect service provision in the future. However, it has been highlighted that the working patterns of female general dental practitioners and specialist orthodontists may differ.10,11
In addition, various reports in the United Kingdom have drawn attention to the increased ethnic diversity that is now seen among both the workforce12,13 and those applying and accepting places at dental schools.14,15,16 Yet there is little evidence to suggest whether ethnic origin and cultural beliefs impact on current working patterns.
The aims of this study were to examine current working patterns of orthodontists in both the NHS and private sector and assess what factors influence their working patterns. In addition the study assessed the effect of career breaks and examined the geographical distribution of orthodontists throughout the United Kingdom.
Materials and methods
Following receipt of ethical approval from the Joint Research and Ethics Committee of the University College London/University College London Hospitals (Reference 06/Q0505/17), a questionnaire was circulated to all of those on the specialist list in orthodontics held by the General Dental Council on the 31 October 2006. At that time there were 1,155 registered orthodontists, however anyone registered with an address outside the United Kingdom was excluded from the study. This resulted in a final target population of 1,088 registrants.
Questionnaire development
The researchers involved in the study held a number of focus groups to ascertain the themes of interest. Following this a pilot questionnaire was developed and distributed to 32 orthodontists (94% response rate) of various levels of seniority and geographic locations in the United Kingdom in order to check ease of completion, acceptability and validity. Following some minor wording changes, the final questionnaire was produced for distribution.
The data collected included:
-
1
Demographic details: gender, ethnicity, current age, number of children and calendar year in which professional qualifications were achieved
-
2
Present working patterns in both the National Health Service (NHS) and private sector together with details of any career breaks taken
-
3
Professional status and location of work place.
Procedure for mailing
The initial mailing was conducted in November 2006 and each registrant was sent a cover letter, a questionnaire and a stamped addressed return envelope. Every effort was made to adopt the principles of the Tailored Design Method17 for postal surveys in an attempt to enhance the response rate. Two further mailings, in January and February 2007, were sent to those who had not responded to the previous mailings.
Statistical analysis
Descriptive statistics were used to summarise the demographics of the workforce. Statistical analysis was carried out using SPSS version 14.0 for Windows (SPSS UK Ltd., Woking, Surrey) and Stata Version 9.2 (Stata, College Station, Texas, USA). ArcView GIS 3.2 (Environmental Systems Research Institute, Inc) geographical mapping software was used to construct the thematic maps. Since various factors may influence the number of sessions worked each week or the length of career breaks taken, multiple regression analyses were undertaken. This allowed assessment of the simultaneous effect of the explanatory variables (gender, calendar year of undergraduate qualification, ethnicity, number of children) on the dependant variables (number of sessions worked each week and duration of career breaks taken).
The distribution of all respondents was categorised according to the location of their primary place of work. The geographical boundaries were formed by the ten strategic health authorities (SHAs) in England as well as the other three United Kingdom countries: Scotland, Wales and Northern Ireland. It was useful to use the strategic health authorities in England as they are responsible for planning health services within their own region.
In order to establish ratios of regional population to whole time equivalent (WTE) orthodontist (one WTE orthodontist corresponds to 10 clinical sessions per week), the number of children aged 10-14 years in each SHA/country was sourced from the United Kingdom mid-2005 population estimates.18 It was deemed that estimates of child to WTE orthodontist ratios based on the number of children aged 10-14 years were more useful to this study than the population as a whole. This is similar to the method used by other researchers.11 In the data analysis the number of respondents was adjusted for non-response to provide the best possible estimate of children aged 10-14 years to WTE orthodontist ratios in each region.
Results
The overall response rate was 81.5% (887/1,088) and no response bias could be found in relation to the gender and calendar year of undergraduate qualification of respondents and non-respondents. In the majority of cases all questions were answered, but occasionally, due to some questions remaining unanswered, the total number of responses in some sections was less than the total number of replies received. Despite the high response rate achieved in this study it must be remembered that 18.5% of the workforce did not respond to the survey and this should be borne in mind when conclusions are made.
Demographics
Sixty percent of respondents were male and the mean age of respondents was 46.12 years (SD 9.91 years). Three-quarters of the workforce had children (75.7%) and the majority of respondents described their ethnicity as White British (71.4%). The next largest group was White 'Other', followed by Asian Indian (6.8%) and White Irish (4.8%). The demographics of the workforce in terms of gender and ethnicity varied with increasing age.
Number of clinical sessions worked per week
A clinical session was defined within the questionnaire as equal to 3.5 to 4 hours (that is, a half day). Male respondents undertake clinical work for, on average, 8.27 (SD 2.68) sessions each week, while the figure for females is an average of 6.99 (SD 2.72) sessions each week. The smooth fit graph in Figure 1 shows the number of clinical sessions worked on average by each gender in relation to time since undergraduate qualification. The graph shows that males, on average, work more clinical sessions per week than females throughout their careers and tend to follow a linear working pattern until retirement, unlike their female colleagues who demonstrate a more variable pattern.

Smooth fit graph of the current number of sessions worked by males and females in relation to time since undergraduate qualification
In order to examine the number of clinical sessions worked each week more closely, a multiple regression analysis was conducted to control for the fact that the demographics of the respondents, in terms of gender and ethnicity, vary with age. This confirmed that male and female orthodontists do have different working patterns, and this difference was statistically significant, with male orthodontists working, on average, 1.5 clinical sessions more per week than their female colleagues (p >0.001) (Table 1). Ethnicity appeared to have a minimal effect on the number of clinical sessions worked each week (Table 1), as did the calendar year of undergraduate qualification (which acts as a proxy for age). The number of children an orthodontist has significantly affected the number of sessions worked (Tables 1, 2, 3). For each child a male orthodontist has, this results on average in a slight increase in the number of clinical sessions worked per week, while the opposite is true for female orthodontists.
Career breaks
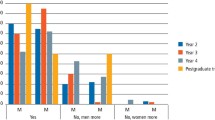
The mean duration of total breaks taken by male and female orthodontists was 10.77 months (SD 10.82 months). However, a much greater proportion of female than male respondents took career breaks (Table 4). Females take individual breaks of around 4-6 months longer, on average, than the breaks taken by males (p <0.001). The majority of female respondents reported 'maternity leave' as the primary reason for taking a career break, while males most frequently reported 'other' reasons such as travelling or further postgraduate study.
Geographical distribution
The ratio of 10-14-year-old children18 to WTE orthodontists in each region showed an uneven distribution throughout the United Kingdom. This is represented geographically in Figures 2, 3, 4 where the data are divided into quintiles and colour coded depending on the level of provision in each SHA/country. It appears that London, the South East of England and Wales have the best ratio of 10-14-year-old children to WTE specialist orthodontist (NHS and private combined) while Scotland and the East Midlands have the most unfavourable ratio (Fig. 2). The highest provision of private orthodontic care was in London and the South of England, while the North East of England and Scotland had the lowest provision. This is well illustrated in Figure 4 where a clear gradient can be seen extending from the South of England, through England and Wales, to Scotland.

Number of 10-14-year-old children per WTE specialist practitioner (NHS and private) (adjusted for non-response)

Number of 10-14-year-old children per WTE NHS specialist practitioner (adjusted for non-response)

Number of 10-14-year-old children per WTE private specialist practitioner (adjusted for non-response)
Discussion
Gender effects
This study confirms that male and female orthodontists have different working patterns and the smooth fit graph (Fig. 1) shows the diversity which exists. Males tend to work at a constant level throughout their careers while females have a more dynamic working pattern. This may be partly explained by the fact that some females take maternity leave shortly after entering the workforce, while the second trough in the graph may be due to females having additional children or due to those in the hospital sector, who have undergone further training, taking their maternity leave at a later stage in their careers. The greatest peak in clinical sessions worked by female respondents occurs approximately 27 to 29 years post-undergraduate qualification, which may be due to their children growing up and thus being able to increase the number of hours they spend at work. This is in agreement with previous reports.4,5 Interestingly, females appear to reduce their workload slightly earlier than males which may have consequences in the future as the number of females in the older age groups increases. However, in this study there were a relatively small number of female orthodontists in this section of the graph so these findings should be treated with some caution.
The multiple regression analysis provides more detailed evidence that gender has an effect on the number of clinical sessions worked per week. The difference found was relatively small, therefore this 'feminisation' might not have as significant an effect as suggested, but still needs to be carefully monitored.
Presently, 37% of the United Kingdom orthodontic workforce is female, however this study found that if a 50:50 gender split in the workforce is ever achieved, only a small additional number of orthodontists would be required to maintain current levels of service (Table 5). Based on all respondents, it was calculated that 898 orthodontists (449 males and 449 females) would be necessary (that is, an increase of 11 practitioners: 898 - 887) to maintain current outputs, which is equivalent to a 1.24% increase in personnel. However, it is important to note that this calculation is based only on those who responded to this study and on the assumption that need and demand for treatment do not change and current working patterns remain the same.
The chances of this happening appear doubtful due to increasing birth rates19 and the growing demand for orthodontic treatment, particularly in the adult population. Recent and proposed legislative changes20,21 may also affect the working patterns of both males and females in the future,22 hence this conclusion should be treated with caution.
Effect of having children
Three-quarters of respondents in this study had one or more children, therefore it was deemed appropriate to examine any potential effect this may have on working patterns. The findings are similar to previous reports, in that having a family tends to increase the number of hours males spend at work while the opposite effect occurs for females.2,4,7 It may be that males must work longer hours in order to support their families or conceivably they may choose to do so! In contrast, females appear to be making an effort to balance their family and working life4 and as their families increase in size, their clinical sessions decrease. The United Kingdom Government, through the Childcare Act,23 aims to increase the availability and enhance the quality of childcare to help parents return to work, but female orthodontists may decide to spend more time at home, especially if their partner is also a professional with a relatively good salary.7
Interestingly the proportion of females who took at least one career break (56.5%) was similar to a previous study examining career breaks taken by male and female dental practitioners.3 Female orthodontists take significantly longer breaks throughout their careers than males but the mean duration of total career breaks taken by all orthodontists in this study was shorter (10.77 months, SD 10.82) than that by dental practitioners (15.81 months, SD 27.56).3 This finding supports the hypothesis of Robinson et al.11 that females who have spent a considerable amount of time in specialist training may be less inclined than general practitioners to decrease their workload. Another explanation may lie in the difficulty that specialists have in securing locum cover for career breaks in many parts of the country. This may force orthodontists to return to work sooner than they would otherwise have wished. The longitudinal nature of orthodontic treatment, as opposed to work in general practice, can also make it more difficult for specialists to take lengthy breaks.
Effects of ethnic differences
The proportion of those from non-White ethnic groups (15.7%) in the orthodontic workforce is double that of the United Kingdom general population (7.9%), while the proportion of those from Asian Indian backgrounds (6.8%) is almost four times that of the general population (1.8%).24 The multiple regression analysis showed that ethnicity had little effect on the number of sessions worked per week or career breaks taken by males or females (Table 1). Therefore, it can be deduced from this study that any changes in ethnic trends that may occur seem unlikely to have a significant impact on workforce planning in the future.
Geographical distribution of orthodontists
In examining the geographical distribution of orthodontists it is important to remember that the geographical boundaries (SHAs in England and Scotland, Wales and Northern Ireland) only provide an overview of the situation in each region and do not reflect the difficulties or ease that individual patients may have in accessing treatment at a local level.
It was obvious that there continues to be an inequitable distribution of orthodontists throughout the United Kingdom11 (Figs 2, 3, 4) and perhaps this is the real issue for workforce planners, in the light of this study showing that gender, calendar year of undergraduate qualification, family size and ethnicity have a relatively small impact on the number of sessions worked each week by orthodontists.
Previous researchers have found a link between place of postgraduate study and current place of work.13,25 Therefore in order to alter this imbalance, strategies which could be considered include changing the current distribution of postgraduate training places throughout the United Kingdom.11,25 An alternative solution may be creating contractual agreements with trainees to determine their location of work upon qualification, which is similar to a model in place in the Republic of Ireland,26 or creating incentive schemes to encourage orthodontists to relocate to areas of poor orthodontic provision. Other initiatives to consider include international and European recruitment programmes, similar to those organized by the United Kingdom Department of Health to attract general dental practitioners to work in the United Kingdom.27,28 This may lead to a workforce deficiency elsewhere, but it is known that some countries have a plentiful supply of orthodontists.29 Therefore, communication between all member states of the European Union may be the way forward to ensure there is an adequate supply of orthodontists for the future.
Conclusion
Many factors, such as gender or family size, influence working patterns. However, a significant disparity persists in the regional distribution of orthodontists throughout the United Kingdom and it may be this factor which is of most importance to orthodontic workforce planning for the future.
References
Department of Health. Report of the primary care dental workforce review. London: Department of Health, 2004. http://www.dh.gov.uk/en/Publicationsandstatistics/ Publications/PublicationsPolicyAndGuidance/DH_4086050 (accessed 10 January 2009).
Newton J T, Thorogood N, Gibbons D . The work patterns of male and female dental practitioners in the United Kingdom. Int Dent J 2000; 50: 61–68.
Newton J T, Buck D, Gibbons D E. Workforce planning in dentistry: the impact of shorter and more varied career patterns Community Dent Health 2001; 18: 236–241.
Brennan D S, Spencer A J . Differences in time devoted to practice by male and female dentists. Br Dent J 1992 172: 348–349.
Matthews R W, Scully C . Working patterns of male and female dentists in the UK. Br Dent J 1994; 176: 463–466.
Seward M. Better opportunities for women dentists - a review of the contribution of women dentists to the workforce. London: Department of Health, 2001. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/ PublicationsPolicyAndGuidance/DH_4005429 (accessed 10 January 2009).
Blasius J J, Pae E K . Work-pattern differences between male and female orthodontists. Am J Orthod Dentofacial Orthop 2005; 128: 283–290.
Duguid R, Drummond J R . The admission of students to UK dental school - recent trends (1983–1998). Eur J Dent Educ 2000; 4: 71–76.
Universities and Colleges Admissions Service. Qualifications/subject dataset 2000–2006. Cheltenham: UCAS, 2007.
Murphy T C, Parkin N A, Willmot D R, Robinson P G . The feminisation of the orthodontic workforce. Br Dent J 2006; 201: 355–357.
Robinson P, Willmot D R, Parkin N A, Hall A C . Report of the orthodontic workforce survey of the United Kingdom, February 2005. Sheffield: The University of Sheffield, 2005. http://www.bos.org.uk/publicationslinks/workforcesurvey.htm (accessed 10 January 2009).
Newton J T, Gibbons D E The ethnicity of dental practitioners in the United Kingdom. Int Dent J 2001; 51: 49–51.
Collins J M, Hunt N P, Moles D R, Galloway J, Cunningham S J . Changes in the gender and ethnicity of the United Kingdom orthodontic workforce. Br Dent J 2008; 205: E12.
Bedi R, Gilthorpe M S . Ethnic and gender variations in university applicants to United Kingdom medical and dental schools Br Dent J 2000; 189: 212–215.
Stewart F M J, Drummond J R, Carson L, Hoad Reddick G . The future of the profession - a survey of dental school applicants. Br Dent J 2004; 197: 569–573.
Gallagher J E, Patel R, Donaldson N, Wilson N . The emerging dental workforce: why dentistry? A quantitative study of final year dental students' views on their professional career. BMC Oral Health 2007; 7: 7. DOI:10.1186/1472-6831-7-7.
Dillman D A. Mail and internet surveys: the tailored design method. 2nd ed. Chapters 1-5. New York: John Wiley and Sons, 2000. ISBN 0 471 32354 3.
Office for National Statistics. Mid-2005 population estimates: quinary age groups and sex for local authorities in the United Kingdom. London: Office for National Statistics, 2006. http://www.statistics.gov.uk/statbase/Expodata/Spreadsheets/D9395.xls (accessed 10 January 2009).
Office for National Statistics. Live births. Fertility highest for 34 years. London: Office for National Statistics, 2008. http://www.statistics.gov.uk/CCI/ nugget.asp?ID=369&Pos=1&ColRank=2&Rank=1000 (accessed 10 January 2009).
Work and Families Act 2006 Chapter 18. London: The Stationery Office, 2006. ISBN 0 10 541 806 4. http://www.opsi.gov.uk/ACTS/acts2006/20060018.htm (accessed 10 January 2009).
Department of Trade and Industry. Work and families: additional paternity leave and pay administration consultation. May 2007. London: Department of Trade and Industry, 2007. http://www.dti.gov.uk/files/file39396.pdf (accessed 10 January 2009).
Newton J T . Comment on 'Career hopes of dental school applicants'. Br Dent J 2005; 198: 697–698.
Childcare Act 2006 Chapter 21. London: The Stationery Office, 2006. ISBN 0 10 542 106 5. http://www.opsi.gov.uk/acts/acts2006/ukpga_20060021_en.pdf (accessed 10 January 2009).
Office for National Statistics. United Kingdom population census 2001: ethnicity. London: Office for National Statistics, 2001. http://www.statistics.gov.uk/CCI/ nugget.asp?ID=764&Pos=4&ColRank=2&Rank=448 (accessed 10 January 2009).
O'Brien K D, Roberts C . An analysis of the effects of place of childhood, undergraduate and postgraduate education upon the regional distribution of specialist orthodontic practitioners. Br Dent J 1991; 171: 280–282.
Irish Health Service Executive. Orthodontic review group report. Chapter 4: training. Dublin: Irish Health Service Executive, 2006.
Department of Health. NHS dentistry: delivering change. Report by the Chief Dental Officer (England) July 2004. London: Department of Health, 2004. http://www.dh.gov.uk/assetRoot/04/08/59/75/04085975.pdf (accessed 10 January 2009).
Department of Health. More dentists now, more dentists later [news release]. London: Department of Health, 2005. http://www.dh.gov.uk/en/Publicationsandstatistics/Pressreleases/DH_4122769 (accessed 10 January 2009).
Van der Linden F P, Schmiedel W J, Bijlstra R J . European orthodontic specialists in 2002. Prog Orthod 2004; 5: 126–140.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Collins, J., Cunningham, S., Moles, D. et al. Factors which influence working patterns of orthodontists in the United Kingdom. Br Dent J 207, E1 (2009). https://doi.org/10.1038/sj.bdj.2009.571
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2009.571
This article is cited by
-
Dental specialist workforce and distribution in the United Kingdom: a specialist map
British Dental Journal (2021)
-
Why dentists should consider a career in orthodontic academia
British Dental Journal (2019)
-
High job satisfaction among orthodontic therapists: a UK workforce survey
British Dental Journal (2018)
-
High job satisfaction among orthodontic therapists
BDJ Team (2018)
-
Career satisfaction and work-life balance of specialist orthodontists within the UK/ROI
British Dental Journal (2017)
