
Abstract
Background:
Pulmonary embolism (PE) is a significant cause of morbidity and mortality in patients with spinal cord injury (SCI). Prophylactic anticoagulation is associated with a reduction in mortality rates, but there is limited evidence regarding the incidence rate of PE following cessation of anticoagulation after the first 3 months of injury.
Study design:
Single-centre retrospective study.
Objective:
To estimate the incidence rate of PE after 90 days of SCI.
Setting:
The National Spinal Injuries Centre at Stoke Mandeville Hospital, Aylesbury, UK.
Methods:
The study includes 640 new-onset SCI patients. All computer tomography pulmonary angiograms (CTPAs) or ventilation-perfusion lung scans between 2008 and 2013 were identified. Medical notes and scans were reviewed and clinical outcomes and radiological findings were recorded.
Results:
A total of 91 patients with a new-onset SCI had a CTPA or a perfusion lung scan. PE was detected in a total of 8 patients. The incidence of PE was 1.25%; 95% confidence interval (0.39–2.11) over a 6-year period. The duration of injury at the time of PE was 7 months.
Conclusion:
The incidence rate of PE post 3 months of SCI remains significant, though much lower than immediately post injury.
Similar content being viewed by others

Introduction
Background
Pulmonary embolism (PE) is a potentially life threatening condition and a significant cause of morbidity and mortality in patients with spinal cord injury (SCI).1 Diagnosing PE in SCI patients can be challenging as usual clinical signs and symptoms of pulmonary emboli may be obscured.2
Diagnostic imaging of PE first involves a chest X-ray to rule out any conditions that mimic PE, including lobar pneumonia or pneumothorax. More definitive imaging investigations include computed tomography pulmonary angiography (CTPA)3 and less commonly, ventilation-perfusion scintigraphy.4 Multislice CTPA has become the principal modality for diagnosis as it is both highly sensitive and specific.3
In the acute phase of SCI (up to 90 days post injury) the incidence of PE has been reported as 4.5% with a mortality rate of 3.5%.5 The introduction of prophylactic anticoagulation therapy in the first 3 months was associated with a reduction in mortality rates.6 Anticoagulation is usually ceased after 3 months post injury, based on autopsy evidence of rare incidences of PE in this period.7, 8 However, the incidence of PE after the initial 3 months post injury is poorly reported in literature.9 In this study, over a 6-year period we examine the incidence rates of PE in SCI patients after anticoagulation was stopped.
Methods
Study design
This is a single-centre retrospective study of SCI. The study reviewed all patients with suspected PE who had a CTPA or ventilation-perfusion lung scan.
Setting
The study setting is the National Spinal Injuries Centre (NSIC) at Stoke Mandeville Hospital, Aylesbury, UK.
Participants
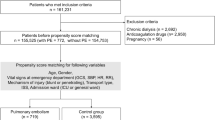
We included all new-onset SCI patients admitted between 2008 and 2013. We excluded children (under 18 years).
Outcomes
Primary outcome
Incidence of PE after 90 days post SCI.
Secondary outcomes.
-
1
Duration of injury associated with PE.
-
2
Extent of paralysis associated with PE.
-
3
Clinical presentation of PE in SCI.
Data sources and management
All CTPA and perfusion scans were identified via Centricity Radiology Information Systems. All images were reviewed by an experienced consultant radiologist. The medical notes of patients with a suspected PE were reviewed and clinical outcomes and radiological findings were recorded. Microsoft Excel software (Microsoft Excel 2013, Redmond, WA, USA) was used to input admission information and collect data. Statistical analyses were performed using IBM SPSS (Version 22.0, Armonk, NY, USA) software.
Statistical methods
Incidence rate
Incidence rates post 90 days of SCI were calculated by dividing the number of new PEs by the number of new admissions in a year.
Follow-up
The follow-up of each individual patient lasted for the inpatient period only. Patients were not followed up after discharge.
Results
This study includes 640 patients with new-onet SCI. The mean injury to NSIC admission duration was 54 days; 95% confidence interval (CI) (50–57). The mean length of hospital stay was 150 days; 95% CI (144–155). The population baseline characteristics are found in Table 1.
During the years from 2008 to 2013, 91 patients had a clinical suspicion for PE and subsequently had a CTPA or perfusion lung scan conducted. Eight patients had a confirmed PE 90 days post SCI. The mean duration of injury at the time of PE was 226 days; 95% CI (138.3–314.9).
The incidence of PE after 90 days post SCI was 1.25%; 95% CI (0.39–2.11) (Table 2).
Four patients of the eight patients diagnosed with PE had tetrapelgia. Five patients had a complete injury (Table 3).
The most common clinical presentations of PE were dyspnoea, chest pain, hypoxia, tachycardia and haemoptysis. Other presentations included atrial fibrillation, respiratory failure and cardiac arrest.
Discussion
Our analysis of pulmonary embolisms 90 days after SCI identified an incidence rate of 1.25%. The duration of SCI at the time of PE was 7 months.
The incidence of PE after 90 days post SCI is lower than the 5–12% incidence rate during the acute phase (first 3 months) as reported in the literature.1, 5 However, it is significantly higher than the PE risk in the general population (0.06% per year).10
Patients with a complete injury AIS A had a slightly higher rate of PE. There was no difference in PE rates between individuals with tetraplegia or paraplegia.
Conclusion
The risk of pulmonary embolism 90 days post SCI remains significant.
Limitations
This is a retrospective analysis of available SCI data at the National Spinal Injuries Centre. To be able to calculate an accurate incidence rate, a prospective multicentre cohort study would be more appropriate. It was beyond the scope of this study to determine correlation of pulmonary embolism with level of injury.
Data archiving
There were no data to deposit.
References
Geerts WH, Bergqvist D, Pineo GF, Heit JA, Samama CM, Lassen MR et al. Prevention of venous thromboembolism: American College of Chest Physicians evidence-based clinical practice guidelines (8th edition). Chest 2008; 133: 381S–453S.
Field-Fote E Spinal Cord Injury Rehabilitation F.A. Davis, Philadelphia, PA, USA 2009.
Stein PD, Fowler SE, Goodman LR, Gottschalk A, Hales CA, Hull RD et al. Multidetector computed tomography for acute pulmonary embolism. N Engl J Med 2006; 354: 2317–2327.
Gottschalk A, Juni JE, Sostman HD, Coleman RE, Thrall J, McKusick KA et al. Ventilation-perfusion scintigraphy in the PIOPED study. Part I. Data collection and tabulation. J Nucl Med 1993; 34: 1109–1118.
Aito S, Pieri A, D’Andrea M, Marcelli F, Cominelli E . Primary prevention of deep venous thrombosis and pulmonary embolism in acute spinal cord injured patients. Spinal Cord 2002; 40: 300–303.
DeVivo MJ, Krause JS, Lammertse DP . Recent trends in mortality and causes of death among persons with spinal cord injury. Arch Phys Med Rehabil 1999; 80: 1411–1419.
Wolman L . The neuropathology of traumatic paraplegia. A critical historical review. Paraplegia 1964; 1: 233–251.
Tribe CR . Causes of death in the early and late stages of paraplegia. Paraplegia 1963; 1: 19–47.
Frisbie JH, Sharma GV . The prevalence of pulmonary embolism in chronically paralyzed subjects: a review of available evidence. Spinal Cord 2012; 50: 400–403.
Oger E . Incidence of venous thromboembolism: a community-based study in Western France. EPI-GETBP Study Group. Groupe d’Etude de la Thrombose de Bretagne Occidentale. Thromb Haemost 2000; 83: 657–660.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Alabed, S., de Heredia, L., Naidoo, A. et al. Incidence of pulmonary embolism after the first 3 months of spinal cord injury. Spinal Cord 53, 835–837 (2015). https://doi.org/10.1038/sc.2015.105
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2015.105
This article is cited by
-
Impact of complications at admission to rehabilitation on the functional status of patients with spinal cord lesion
Spinal Cord (2020)
-
Re: Incidence of pulmonary embolism after the first 3 months of spinal cord injury
Spinal Cord (2016)
-
Dopamine D1 receptor agonist A-68930 inhibits NLRP3 inflammasome activation and protects rats from spinal cord injury-induced acute lung injury
Spinal Cord (2016)
-
Behandlungs- und Rehabilitationskonzepte bei traumatischer Paraplegie und Tetraplegie
Trauma und Berufskrankheit (2016)
