
Abstract
Study design:
Evidence-based review.
Objective:
To determine the effectiveness and acceptability of transanal irrigation in children and young people with neurogenic bowel.
Setting:
International literature.
Methods:
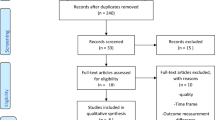
Electronic databases were searched supported by hand-searching strategies to conduct a comprehensive literature review in accordance with Centre for Reviews and Dissemination procedures guidelines. Sixteen studies were selected for inclusion.
Results:
The studies indicate that transanal irrigation can be an effective treatment for children and young people with constipation or faecal incontinence as a result of neurogenic bowel (90%, n=346 children). Transanal irrigation is reported as improving quality of life and family’s satisfaction with their bowel management, although the procedure is invasive, time consuming and can impact negatively on child, parent and family life.
Conclusion:
Transanal irrigation may be considered as a first line treatment option for children and young people with neurogenic bowel but further research is required to prove the efficacy and acceptability of this procedure.
Similar content being viewed by others


Introduction
Transanal irrigation involves the physical placement of an irrigation catheter or cone device safely into the rectum to allow the administration of irrigation fluid. The aim of irrigation is to washout stool from the rectum and lower end of the descending colon in order to facilitate a period of faecal continence and/or alleviate constipation. Transanal irrigation is not a new technique but is regaining popularity as a treatment option in the management of neurogenic bowel following the advent of new and improved irrigation systems. Transanal irrigation is a prescribed regime, which should only be started or considered as a treatment after assessment by suitably qualified or experienced health professional. Neurogenic bowel often occurs in children or young people as a result of neurological antenatal development, such as spina bifida, childhood spinal cord injury or acute viral illness such as transverse myellitus. Although there is an evidence that transanal irrigation is a useful management approach in adult patients with neurogenic bowel,1, 2 there is less published research on the use of this approach with children and young people. This review aimed to systematically examine the current literature relating to the use of transanal irrigation in children and young people with neurogenic bowel.
Review question
A review was carried out to assess whether transanal irrigation is an effective and acceptable long-term treatment for children and young people with neurogenic bowel.
Review methods
The review has been informed by the Centre for Reviews and Dissemination procedures3 and aimed to follow a rigorous approach to comprehensively identify the literature addressing the review question.
Study selection (inclusion and exclusion criteria; methods)
-
Inclusion criteria
-
•Collection of empirical data
-
•Study of children aged <18 years of age
-
•Children and young people using transanal irrigation as a long-term management regime for neurogenic bowel
-
Exclusion criteria
-
•Young people aged >18 years old
-
•Transanal irrigation for one off treatment of impaction, pre-operative bowel preparation or radiological investigation
-
•Review, opinion or editorial pieces
Identification of studies
A comprehensive search of the following databases, Medline via Pubmed, CINAHL, EMBASE and PsychINFO was carried out in 2011 and re-run in 2012. The following terms were entered into the above databases:-
Transanal irrigation, rectal irrigation, anal irrigation, peristeen, rectal enema, retrograde enema, transanal colonic irrigation and retrograde rectal irrigation. These were combined through the use of Boolean operator AND to child*, adolescent*, young people, young person, teenager, pre-school, infant, babies and paediatric. Mesh terms were used where available. This resulted in 182 papers being identified.
Hand searching of reference lists from relevant studies, key journals and conference proceedings was also carried out along with citation searching and entering the key search terms into wider internet search engines (Google) to identify any informally published research studies. No further studies or papers resulted from this search. Titles and abstracts were reviewed to ascertain their relevance to the inclusion criteria and this was followed by screening of the full papers identified as possibly relevant in the initial search. To avoid selection bias, selection and data extraction was conducted by both authors.

The search was not restricted to any specified dates and covered the range 1981 to November 2011 (date of review). The search was also not limited to include or exclude specific outcome measures as the review sought to investigate what outcome measures were being used within this field. Studies that included a mixed population (adults and children), without clearly reporting the outcomes and results of children as a separate subgroup were excluded from the review. Two papers that included children and reported some data distinctly were excluded as they did not fulfil the inclusion criteria of reporting empirical data. Some papers included small numbers of children with a primary diagnosis other than neurogenic bowel, that is, imperforate anus; these studies were included if the majority of children and young people included had a diagnosis of neurogenic bowel.
Data extraction
Data were extracted into an electronic proforma, variables included authors, aim, study design, sample, follow-up of patients, definition of continence/incontinence, data collection methods, analysis and findings (effectiveness and acceptability). Data extraction was conducted independently by the two authors to support the process being unbiased and reliable,3 no discrepancies were encountered. The authors of two papers were contacted to clarify the missing or ambiguous information from the papers. No response was received from one author.
Quality assessment
As the review identified a poor base of evidence and a lack of rigorous studies (randomised controlled trials and controlled trials) from the higher points of the hierarchy of evidence, all the studies that fulfilled the inclusion criteria were included in the review, including case reports and case series. By including all studies relevant to the inclusion criteria, the review aimed to identify any gaps in the current evidence base. Inadequate reporting of important aspects of methodological quality was a common occurrence in the studies relevant to the review. Owing to the lack of papers addressing the review question and the general poor quality of the studies within this field, the review did not exclude the studies that failed to report aspects of the research procedures.
Data synthesis
Results were compared both within and between studies but formal meta-analysis was not conducted due to the heterogeneity of the sample populations, follow-up, prescribed irrigation regime, assessment tools and outcome measurements. As formal statistical techniques were not appropriate for this review, a narrative approach was taken to synthesise the studies.
Results of the review
Sixteen studies were included in the review (Table 1).
Details of the included and excluded studies
All the studies were case series either reporting the collection of retrospective or prospective data with convenient samples of children who were using transanal irrigation within a single centre. Some of the studies administered questionnaires to collect data on reported clinical symptoms,4, 5, 6, 7, 8, 9 Neurogenic Bowel Dysfunction Scale,10, 11 quality of life5, 10, 11 and patient satisfaction Likert scales.5, 10, 12 Only the Neurogenic Bowel Dysfunction Scale is a validated instrument (in adult patients), the other questionnaires used in the reported studies were locally developed and non-validated. There was a general lack of information within the papers on who completed the questionnaires. The majority of questionnaires appeared to be completed by parents either within the clinical setting as part of the child’s normal health care follow-up9, 10, 11 or over the telephone.4, 5, 12, 13 Several of the studies reported data collected retrospectively from medical case notes6, 13, 14 or reported findings based on data without it being stated how data had been obtained.6, 15, 16, 17, 18
The follow-up of children after initiation of transanal irrigation varied widely both within and across the studies. Where detailed, follow-up and data collection occurred from 3 months,10 4 months,8, 17 12 months,4 33 months,14 64 months6 to 96 months.8
Findings of the review
This evidence-based narrative review aimed to explore how effective and acceptable transanal irrigation is within this population and the findings are discussed within these two sections.
Effectiveness of transanal irrigation in children
The papers that investigated the use of transanal irrigation in children reported incidences of constipation and faecal incontinence as separate subgroups, whereas in other studies these were reported as a generic group. The definitions used to define continence/incontinence and constipation varied between studies. Definitions and criteria to judge incontinence varied from any episodes or incidences of staining, soiling or faecal incontinence,4, 6, 9, 11, 12, 19 soiling once a month,10 soiling three times a month,16 not needing to wear pads for stool incontinence13 to no information being supplied on how the studies had characterised continence or incontinence.5, 14, 15, 17, 18
This review has correlated with the studies, whose report rates of continence were achieved. In order to combine the findings, a successful outcome of transanal irrigation is defined in this narrative review as an increased level of continence in those children still using transanal irrigation at the point of follow-up. Transanal irrigation was reported as improving the continence in 346 from 383 (90%) children using transanal irrigation at the point of follow-up in the various studies.4, 6, 9, 10, 11, 14, 16, 17, 19 The reports of continence achieved within this figure ranged from 66%14 to 100%11, 16 (Table 2).
Two studies describe the outcomes of children with constipation and faecal incontinence separately, Pena et al.12, 15 reports that 41 out of 45 children with constipation (91%) and 112 out of 128 (88%) children with faecal incontinence demonstrated improvements to their continence using transanal irrigation. The study by Liptak and Revell12 at 18-month follow-up indicates that 5 out of 25 (20%) children reported difficulties with constipation, this decreased further at the 30-month follow-up with 2 out of 16 children reporting the passage of hard stool as problematic. The use of irrigation improved continence in 18 children out of 25 (72%) at 18-month follow-up with a further improvement noted at the 30-month follow-up in 15 out of 16 (94%) children. Some studies do not report rates of faecal continence achieved7 and report outcomes as those satisfied with the regime,5 those still using the procedure at the point of follow-up18 or improved bladder function.13
Saline (either isotonic or made by families within the home) was used to irrigate the bowel in 8 of the 17 studies,4, 7, 12, 15, 16, 17, 18, 19 which included 495 children. Tap water was used in 7 of the studies,5, 6, 8, 9, 10, 11, 14 which in total included 270 children. One paper did not report the type of solution used to irrigate the bowel.13 Different volumes of solution, timings and temperatures were used in the different studies depending on patient preference, faecal result and efficacy. Owing to the variability of design, outcomes assessed and reported and the quality of the studies, it is not possible to statistically analyse if the type of solution used influenced the effectiveness of transanal irrigation.
Acceptability of transanal irrigation to children, parents and families
The studies examining the satisfaction of parents and children with transanal irrigation generally reported medium to high levels of satisfaction with the regime. Owing to the variability of scales used and the different outcomes reported, this review does not attempt to correlate the findings from the different studies. Sixty parents reported their satisfaction with their child’s continence as improving from 3.0, before using transanal irrigation, to 7.7 after using transanal irrigation (on a scale of 0–10), a statistically significant finding (P<0.001).10 All parents (100%, n=43) of children using transanal irrigation reported over the telephone that they were satisfied with the regime (scale 1–3), although 29 (60%) of these complained that the regime impacted on their social life.5 Thirty five parents rated their child’s quality of life and grade of satisfaction (on one joint scale from 0–10, 0=great reduction, 10=great improvement) as improved (mean 7.3) after using transanal irrigation.11 Another questionnaire study reported that 35 out of 40 parents found transanal irrigation satisfactory (although no information is provided on the scale used) and reported positive improvements in their child’s wellbeing (open comments at the end of the questionnaire).8 All of these 35 parents reported the regime as time consuming.
From forty-one parents, 63% (n=28) stated they were very satisfied with the transanal irrigation regime and 37% (n=15) stated they were just satisfied with the regime, although no details are provided as to the questionnaire used to collect data.14 From these parents, 51% (n=21) identified that the regime took time and energy to do and 39% (n=16) identified the regime as a daily burden on the family. Some papers have reported the procedure as satisfactory for most families, and it enables children to feel in control of their lives with no information being provided on what evidence this conclusion is been based on.18
Judging the acceptability of the procedure to the children and parents who use transanal irrigation was a secondary outcome in some of the reported papers. The papers refer to the satisfaction5, 10, 11, 12, 14 and quality of life,5, 10, 11 both of which in the majority of cases are assessed on Likert Scales ranging from 0–3,5 1–4,12 0–5 (Cazamier et al.5) or 0–10.10, 11 In most cases it is the parent who has completed these scales and it could be argued that it is difficult to gain an understanding of the subjective experience of administering an invasive procedure on your child or on the child themselves from a single numerical scale. Many papers report the number of children who continue to use transanal irrigation at the point of follow-up and some provide details on those who no longer use the procedure due to clinical reasons, the regime causing the child to become upset, the family or child being uncompliant4 or unmotivated to continue;17 this information could also be seen to provide data on how acceptable the procedure is to be judged by families.
Discussion
The majority of the papers included in this review are case series and case reports with no control or matched groups and as such are more susceptible to bias than experimental studies.3 Only a few of the studies reviewed use validated questionnaires, data was in many cases collected retrospectively and in many studies there were limited follow-up. Therefore, the conclusions that can be made from this review are tentative, limited and focus more on highlighting areas for further research.3
The findings indicate that transanal irrigation can increase levels of faecal continence in children with neurogenic bowel. Currently transanal irrigation is often not proposed until families have journeyed through the use of many different regimens to treat their child’s constipation or faecal incontinence. The data in this review suggest that transanal irrigation should be considered by clinicians as a first line treatment for children with neurogenic bowel with faecal incontinence or constipation, but further quality research is needed to support the use of this simple and effective treatment. There are documented risks associated with transanal irrigation which include systemic reactions to irrigation solutions and rectal perforation, although these were not the key findings within this review. Health professionals and parents should be made aware of these potential risks, although the incidence is reported as low and should be weighed up against the improvement to continence which transanal irrigation can offer. The recommendation of using transanal irrigation is cognisant that there can be a tension between a regime being effective and parents having to carry out an invasive procedure on their child. The single scale numerical ratings of satisfaction and quality of life may not be sensitive enough to judge how this procedure impacts on parents and children’s lives, and further work is needed to develop measurement tools that can be used in this context to reliably assess the physical, emotional and psychosocial aspects of managing a long-term bowel condition. This review highlights the lack of evidence-based criteria to determine when transanal irrigation should be considered as a management option or to assess the effectiveness of treatment for children and young people. Improving the quality of professional, parent and young people training and educational materials and access to information as well as investing in undertaking rigorous research will impact on both clinical care and also scientific outcome data.
Longitudinal data regarding transanal irrigation use is limited. The transition from parents’ co-ordinating and administering irrigation to children or young people becoming independent warrants further study. The barriers to children and young people mastering early independence with irrigation need to be investigated along with the reasons behind why young people who were using irrigation successfully decide to abandon this approach.
Conclusion
Although irrigation can be described as an effective procedure in improving continence, it can be disruptive to a child and family’s life and more rigorous research is needed in this field to determine the efficacy of this treatment and the acceptability and quality of life of children, young people and parents involved in using transanal irrigation as a long-term treatment for neurogenic bowel.
References
Christensen P, Bazzochi G, Coggrave M, Abel R, Hulting C, Krough K et al. Randomized controlled trial of transanal irrigation versus conservative bowel management in spinal cord-injured patients. Gastroenterology 2006; 131: 738–747.
Christensen P, Bazzochi G, Coggrave M, Abel R, Hulting C, Krough K et al. Outcome of transanal irrigation for bowel dysfunction in patients with spinal cord injury. J Spinal Cord Med 2008; 31: 560–567.
Centre for Reviews and Dissemination Systematic Reviews. CRD’s guidance for undertaking reviews in healthcare. University of York. 2008.
Blair GK, Djonlic K, Fraser GC, Arnold WD, Murphy JJ, Irwin B . The bowel management tube: an effective means for controlling fecal incontinence. J Pediatr Surg 1992; 27: 1269–1272.
Cazemier M, Felt-Bersma RJF, Mulder C . Anal plugs and retrograde colonic irrigation are helpful in fecal incontinence or constipation. World J Gastroenterol 2007; 14: 3101–3105.
Matsuno D, Yamazaki Y, Shiroyanagi Y, Ueda N, Suzuki M, Nishi M et al. The role of the retrograde colonic enema in children with spina bifida: is it inferior to the antegrade continence enema? Ped Surg Int 2010; 26: 529–533.
Marshall D, Connolly L, Kelly E . A survey of bowel washout practice in children with neuropathic bowel in the UK and Ireland. Cerebrospinal Fluid Res 2009. Available Online www.cerebrospinalfluidresearch.com/content/6/S2/S30 (Accessed September 2011)..
Mattsson S, Gladh G . Tap-water enema for children with myelomeningocele and neurogenic bowel dysfunction. Acta Paediatricia 2006; 95: 269–274.
Vande VS, Van Biervliet S, van Renterghem K, van Laecke E, Hoebeke P, van Winckel M . Achieving fecal continence in patients with spina bifida: a descriptive cohort study. J Urol 2007; 178: 2640–2644.
Ausili E, Focarelli B, Tabacco F, Murolo D, Sigismondi M, Gasbarrini A et al. Transanal irrigation in myelomeningocele children: an alternative. Safe and valid approach for neurogenic constipation. Spinal Cord 2010; 48: 560–565.
Lopez-Pereria P, Salvador OP, Arcas JA, Urrutia MJM, Romera RL, Monereo EJ . Transanal irrigation for the treatment of neuropathic bowel dysfunction. J Pediatr Urol 2010; 6: 134–138.
Liptak GS, Revell GM . Management of bowel dysfunction in children with spinal cord disease or injury by means of the enema continence catheter. J Pediatr 1992; 120: 190–194.
Neel KF . Total endoscopic and anal irrigation management approach to noncompliant neuropathic bladder in children: a good alternative. J Urol 2010; 84: 315–318.
Scholler-Gyere M, Nesselaar C, Van Wieringen H, van Gool JD . Treatment of defecation disorders by colonic enemas in children with spina bifida. Eur J Ped Surg, Supp 1996; 1: 32–34.
Pena A, Guardino K, Tovilla JM, Levitt MA, Rodriguez G, Torres R . Bowel management for fecal incontinence in patients with anorectal malformations. J Pediatr Surg 1998; 33: 133–137.
Shandling B, Gilmour RF . The enema continence catheter in spina bifida: successful bowel management. J Pediatr Surg 1987; 22: 271–273.
Walker J, Webster P . Successful management of faecal incontinence using the enema continence catheter. Z Kinderchir 1989; 44: 44–45.
Willis RA . Faecal incontinence—Willis Home Bowel Washout Programme. Z KInderchir 1989; 44: 46–47.
Eire PF, Cives RV, Gago MC . Faecal incontinence in children with spina bifida: the best conservative treatment. Spinal Cord 1998; 36: 774–776.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Bray, L., Sanders, C. An evidence-based review of the use of transanal irrigation in children and young people with neurogenic bowel. Spinal Cord 51, 88–93 (2013). https://doi.org/10.1038/sc.2012.146
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2012.146
Keywords
This article is cited by
-
Neurogenic Bowel in the Pediatric Patient—Management from Childhood to Adulthood
Current Bladder Dysfunction Reports (2021)
-
How to establish a successful bowel management programme in children: a tertiary paediatric centre experience
Irish Journal of Medical Science (1971 -) (2019)
-
Transanal irrigation is effective in functional fecal incontinence
European Journal of Pediatrics (2017)
-
Prospective evaluation of transanal irrigation for fecal incontinence and constipation
Techniques in Coloproctology (2017)
-
Impact of the Bowel Management Program on the quality of life in children with fecal incontinence
Pediatric Surgery International (2016)
