
Abstract
Study design:
Retrospective analysis of research data collected over >18 years at our center.
Objectives:
Examine results of repeated semen retrievals in men with spinal cord injury (SCI) who were initially found to be azoospermic.
Setting:
Major university medical center.
Methods:
Three different groups were analyzed in this study. Group 1 (n=15) consisted of patients who were found to be azoospermic after the first ejaculation obtained by penile vibratory stimulation (PVS) and who had subsequent ejaculates obtained by PVS. Group 2 (n=8) consisted of patients who were found to be azoospermic after the first ejaculation obtained by PVS and who had subsequent ejaculates obtained by electroejaculation (EEJ). Group 3 (n=18) consisted of patients who were found to be azoospermic after the first ejaculation obtained by EEJ and who had subsequent ejaculates obtained by EEJ.
Results:
In group 1 (PVS–PVS), the second ejaculate contained sperm in none of the 15 patients. In group 2 (PVS–EEJ), the second ejaculate contained sperm in three of eight patients. In group 3 (EEJ–EEJ), the second EEJ resulted in semen with sperm in 6 of 18 patients. In the 388 study subjects, the overall prevalence of azoospermia was 7.0%.
Conclusion:
In a study of a large group of subjects with SCI, the vast majority had normal sperm concentrations. In the minority who were azoospermic on their first ejaculate, and who were past the acute phase of injury, obtaining a second ejaculate by EEJ versus PVS may be a reasonable step before proceeding to surgical sperm retrieval.
Similar content being viewed by others

Introduction
Infertility is one of the most devastating complications of spinal cord injury (SCI) in male patients. This problem is mainly caused by anejaculation and/or semen abnormalities.1 Modern techniques of semen retrieval, namely penile vibratory stimulation (PVS) and electroejaculation (EEJ), are highly effective in inducing ejaculation in most men with SCI. It is generally accepted that if PVS with one or two high amplitude vibrators is not effective, then EEJ should be tried.2 According to our experience, application of this algorithm results in ejaculation in 97% of SCI patients.3
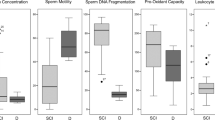
The quality of semen obtained from men with SCI is usually poor. Low sperm motility and low sperm viability are the most common abnormalities.1 Although most men with SCI have normal sperm concentrations, a minority are azoospermic.4 This relatively small group of SCI patients represents a major clinical challenge. In men with SCI, management of anejaculation has been thoroughly studied; however, the consensus management strategy for azoospermia in these patients remains to be established. For example, in able-bodied men, at least two semen analyses are recommended before diagnosing azoospermia.5 It is not known whether this recommendation is valid for azoospermic patients with SCI. It is also not known whether azoospermia resulting from one method, such as PVS, will also result with an alternative method, such as EEJ.
To address these issues, we performed a retrospective analysis of research data collected over >18 years in our center. The purpose of this study was to examine subsequent ejaculates in SCI patients whose first ejaculate was found to be azoospermic.
Materials and methods
The subjects were men with SCI enrolled in the Male Fertility Research Program of the Miami Project to Cure Paralysis at the University of Miami Miller School of Medicine (Miami, FL, USA). Each subject signed an informed consent. The study was approved by the institutional review board. A retrospective review was performed of research data collected between January 1991 and September 2009.
Semen specimens were obtained by PVS or EEJ. PVS was performed as previously described6 using the FERTI CARE personal vibrator (Multicept A/S, Albertslund, Denmark). EEJ was performed as previously described using the Seager model 14 EEJ unit (Dalzell USA Medical Systems, The Plains, VA, USA).7
Our algorithm of sperm retrieval in patients with SCI has been previously described.3 In brief, patients who were unable to ejaculate with masturbation were administered a trial of PVS with one vibrator. Failures with one vibrator were administered a trial with two vibrators (that is, the ‘sandwich’ technique) unless: (1) their level of injury was T11 or caudal or (2) they had complete absence of somatic responses, that is, absence of muscle contractions below the level of injury. These cases proceeded to EEJ.
After 15–20 min of liquefaction, neat antegrade semen specimens were analyzed using disposable semen analysis chambers (Cell-VU; Millennium Sciences, New York, NY, USA). Retrograde semen specimens were obtained by draining and lavaging the contents of the bladder after PVS and EEJ procedures. Azoospermia was confirmed by centrifuging antegrade or retrograde semen specimens at 500 g for 10 min, and examining the pellet for sperm.
Our database as of September 2009 consisted of 506 subjects who received a total of 3235 semen retrieval trials. The subjects included in this study were those who underwent at least two procedures that resulted in ejaculation (that is, appearance of semen), but who had no sperm in the first ejaculate. We have observed over the years that efforts at assisted ejaculation may not be consistently successful for up to 18 months after injury (NL Brackett, unpublished data). To control for this inconsistency, the only procedures included in this study were those performed ⩾18 months after injury. Considering all inclusion criteria, a total of 37 subjects were included in the study. Depending on the outcomes of their semen retrieval trials, subjects were assigned to the following groups.
Group 1 (PVS–PVS): Subjects who were found to be azoospermic after the first ejaculation obtained by PVS and who had subsequent ejaculates obtained by PVS. In all, 15 subjects met the criteria for group 1.
Group 2 (PVS–EEJ): Subjects who were found to be azoospermic after the first ejaculation obtained by PVS and who had subsequent ejaculates obtained by EEJ. In all, eight subjects met the criteria for group 2.
Group 3 (EEJ–EEJ): Subjects who were found to be azoospermic after the first ejaculation obtained by EEJ and who had subsequent ejaculates obtained by EEJ. In all, 18 subjects met the criteria for group 3.
Of the 37 subjects, two subjects overlapped in groups 1 and 2. One subject overlapped in groups 1–3.
The serum levels of testosterone, luteinizing hormone, follicle-stimulating hormone and prolactin were assessed for the majority (n=32) of subjects in groups 1–3.
Statement of ethics
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Statistical analysis
Values were expressed as mean±s.d.. Statistical analysis was performed using the Mann–Whitney U test or Kruskal–Wallis analysis of variance as appropriate. If the latter test showed statistically significant differences between groups, it was followed by multiple comparisons of mean ranks post hoc tests. Computer software Statistica 8.0 (StatSoft Inc., Tulsa, OK, USA) for Windows was used for all statistical analyses with P<0.05 considered statistically significant.
Results
The characteristics of subjects from groups 1–3 are presented in Table 1. The age at the time of injury in group 1 (19.2±6.7 years) was significantly lower than that of group 3 (26.9±7.1 years, P=0.004). No other statistically significant differences were found between groups with regard to: age at the time of first semen analysis, age at the time of injury, duration of injury or the interval between ejaculation trials.
The level of injury of subjects in groups 1–3 is also shown in Table 1. Data regarding completeness of injury are not presented because the method of its assessment changed several times over the years of the study. As a result, our data in this respect are not consistent.
In group 1 (PVS–PVS), the second ejaculate contained sperm in none of the 15 subjects. Some men wished to pursue additional trials of PVS (8 patients had 3 trials of PVS and 4 patients had 4 trials of PVS). In one of these men, sperm (13.1 million per ml) were obtained on the third trial of PVS. In this man, ejaculation occurred only when PVS was combined with abdominal electrical stimulation.8 In a second subject, sperm (4.3 million per ml) were obtained on his fourth trial of PVS. In the remaining subjects in group 1, none had sperm in subsequent ejaculates.
In group 2 (PVS–EEJ), of the eight subjects who had no sperm when their initial ejaculates were obtained by PVS, three had sperm on their first attempt with EEJ.
In group 3 (EEJ–EEJ), the second EEJ resulted in semen with sperm in 6 out of 18 subjects. In the remaining 12 subjects, further EEJ trials (third trial in 3 subjects and fourth trial in 2 subjects) did not result in semen with sperm. The mean interval between EEJs did not differ in subjects who were and were not found to be azoospermic on the second trial (0.47±0.60 vs 0.22±0.20 years, P=0.49).
The overall prevalence of azoospermia was 7.0% (27 of 388 subjects). Specifically, 27 subjects were found to be azoospermic in ⩾2 semen samples and 361 subjects had sperm in their semen.
The prevalence of hormone outliers was 51.6% for all subjects in groups 1–3 combined (Table 2). A common abnormality was elevated follicle-stimulating hormone (12.5% of outliers). Another common abnormality was elevated follicle stimulating-hormone combined with elevated luteinizing hormone (12.5% of outliers). No particular endocrine patterns were shown to be characteristic of men who did versus men who did not have sperm in subsequent ejaculates.
Five subjects consented to have transrectal ultrasound performed. In all of them, prostate size was normal for their age. Their seminal vesicles appeared normal in size and there was no evidence of ejaculatory duct obstruction.
Discussion
It is estimated that in the United States, >10 000 SCIs occur annually, with the majority occurring to men aged between 18 and 35 years.9 In addition to ejaculatory and erectile dysfunction, most of these men have poor semen quality and some are azoospermic. In this study, we tried to take a closer look at the small group of SCI patients who were azoospermic.
Our results indicate that the probability of finding any sperm in subsequent ejaculates of patients who were found to be azoospermic in their first ejaculate was relatively higher if EEJ versus PVS was used as a method of semen retrieval. In these cases, sperm were present in the second ejaculate in approximately one-third of patients.
In the general population, the prevalence of azoospermia is approximately 1%10 and, among infertile men, it ranges between 10 and 15%.11 Our study demonstrates that the prevalence of azoospermia in patients with SCI is comparable to those in the general population of infertile men.
Traditionally, the causes of azoospermia are divided into three main categories: pre-testicular (endocrine abnormalities), testicular (primary disorders of spermatogenesis) and post-testicular (obstruction or ejaculatory dysfunction).5 Although all of these causes could be present in men with SCI, their relative prevalence and significance may be different from the general population.
The role of testicular failure (either primary or secondary) in the pathogenesis of semen abnormalities in men with SCI remains a controversial subject. Although some earlier studies showed a significant prevalence of severe impairment of spermatogenesis in this group of patients,12, 13, 14 these results have not been supported by more recent data.15, 16 For example, Elliott et al.16 reported testis biopsy results in 50 men with SCI. Of these, 43 had mature sperm on histological examination of the testicular tissue. Interestingly, in the study by these researchers, the prevalence of mature sperm on histological examination was the same in patients with azoospermia as it was in patients with oligozoospermia. Maturation arrest was rare, and the Sertoli-cell-only syndrome was not found in this series.
Severe testicular abnormalities are often reflected by elevation in serum levels of follicle-stimulating hormone.17 Results of endocrine evaluation, however, were not useful in predicting the appearance of sperm in subsequent ejaculations in our study.
Ejaculatory dysfunction, which is a rare cause of azoospermia in neurologically intact men,5 is a much more probable cause of this abnormality in men with SCI. Our study found that of the 15 patients who were azoospermic when their first ejaculate was obtained by PVS, all were azoospermic when their second ejaculate was obtained by PVS. In contrast, of the eight patients in group 2 (PVS–EEJ) who were azoospermic when their first ejaculate was obtained by PVS, three had sperm when their second ejaculate was obtained by EEJ.
A possible explanation for the improved success rate of second trials of EEJ versus second trials of PVS is that PVS and EEJ stimulate ejaculation via different mechanisms. PVS is presumed to recruit the ejaculatory reflex by stimulating the dorsal penile nerve that enters the spinal cord via the pudendal nerve at S2–S4. A lidocaine block of the dorsal penile nerve inhibits PVS-induced ejaculation in men with SCI.18 Ejaculates obtained by PVS versus EEJ typically have more antegrade volume and a greater percentage of sperm in antegrade versus retrograde fractions.19 In our experience, a majority of ejaculates obtained by PVS have few sperm in the retrograde fraction. Taken together, these observations imply that, with PVS versus EEJ, there is greater coordination among the various components of ejaculation. Our subjects were typically tested with a vibrator optimized for inducing ejaculation in men with SCI. The frequency and amplitude of the vibrator head were well controlled and reproducible. It stands to reason that the ejaculatory responses of the subjects should also be reproducible, and in fact they are, for responders as well as non-responders.20
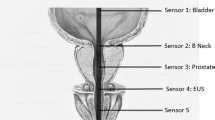
In contrast to PVS, EEJ is performed by placing a probe containing electrodes into the patient's rectum and delivering electrical stimulation until semen is released. EEJ relies, at least in part, on direct stimulation and contraction of the accessory glands to release stored fluid and spermatozoa. This mode of stimulation could account for the positive second response by EEJ that occurred in three of eight subjects in group 2.
There were a significant number of patients who were azoospermic when their first ejaculate was obtained by EEJ, but who had sperm when their second ejaculate was obtained by EEJ (6 of 18 patients). Appearance of sperm in the EEJ–EEJ group is more difficult to explain. One possible explanation is that, given the small amount of current used to produce the ejaculate, the nerve stimulation of the accessory glands was somehow different between the first and second ejaculates, that is, deficient in the first EEJ and present in the second EEJ. It is possible, and in fact quite probable, that placement of the probe, as well as its contact with the rectal wall and its distance from the end organs, varied from one trial to another. Furthermore, the conductivity of the tissues involved may have been variable. All or some of these differences may be important in this small group of patients with respect to the appearance or not of sperm in the ejaculate, although the usual somatic responses (which typically occur at lower currents and involve somatic myelinated nerves) were seen in all the subjects in this study.
Another possible explanation is that the first and second trials of EEJ were significantly farther apart in patients who were not versus those who were azoospermic on their second EEJ, possibly allowing for recovery of sluggish testicular function. An analysis of the mean interval between EEJs, however, showed no significant difference between patients who were not versus patients who were azoospermic on the second trial of EEJ.
Another possible explanation is that the six patients who had sperm on the second ejaculate had their first procedure aborted prematurely because of pain, autonomic dysreflexia or other reasons. A close inspection of the records, however, revealed no prematurely aborted EEJ procedures. The level of injury of these 6 patients (T1–T10 in 3 and T10–L2 in 3) was not significantly different from the other 12 (cervical in 1, T1–T10 in 8 and T10–L1 in 3).
The immediate management implications of our findings are limited because of the small number of patients included in the analysis. Nevertheless, our data provide evidence that in patients who are azoospermic past the first 18 months after injury, a trial of EEJ may be a reasonable step before proceeding to surgical sperm retrieval. Repeated trials of PVS (>2) may be considered if the patient's transrectal ultrasound shows no evidence of obstruction, and if the patient refuses EEJ.
The retrospective design of our study is a limitation. We did not have consistent data regarding other information necessary for diagnosing azoospermia, such as testis biopsy results. Nevertheless, we believe that our data provide a small but valuable contribution to practitioners who manage infertility in men with SCI.
References
Brackett NL, Lynne CM, Ibrahim E, Ohl DA, Sonksen J . Treatment of infertility in men with spinal cord injury. Nat Rev Urol 2010; 7: 162–172.
Ohl DA, Quallich SA, Sonksen J, Brackett NL, Lynne CM . Anejaculation: an electrifying approach. Semin Reprod Med 2009; 27: 179–185.
Brackett NL, Ibrahim E, Iremashvili V, Aballa TC, Lynne CM . Treatment of ejaculatory dysfunction in men with spinal cord injury: an 18-year single center experience. J Urol 2010; 183: 2304–2308.
Kafetsoulis A, Brackett NL, Ibrahim E, Attia GR, Lynne CM . Current trends in the treatment of infertility in men with spinal cord injury. Fertil Steril 2006; 86: 781–789.
Practice Committee of American Society for Reproductive Medicine in collaboration with Society for Male Reproduction and Urology. Evaluation of the azoospermic male. Fertil Steril 2008; 90 (Suppl 5): S74–S77.
Brackett NL . Semen retrieval by penile vibratory stimulation in men with spinal cord injury. Hum Reprod Update 1999; 5: 216–222.
Brackett NL, Ead DN, Aballa TC, Ferrell SM, Lynne CM . Semen retrieval in men with spinal cord injury is improved by interrupting current delivery during electroejaculation. J Urol 2002; 167: 201–203.
Kafetsoulis A, Ibrahim E, Aballa TC, Goetz LL, Lynne CM, Brackett NL . Abdominal electrical stimulation rescues failures to penile vibratory stimulation in men with spinal cord injury: a report of two cases. Urology 2006; 68: 9–11.
National SCI Statistical Center. Spinal Cord Injury—Facts and Figures at a Glance 2009. Available at http://www.spinalcord.uab.edu/show.asp?durki=119513&site=4716&return=19775. Accessed 1 February 2010.
Stephen EH, Chandra A . Declining estimates of infertility in the United States: 1982–2002. Fertil Steril 2006; 86: 516–523.
Jarow JP, Espeland MA, Lipshultz LI . Evaluation of the azoospermic patient. J Urol 1989; 142: 62–65.
Stemmermann GN, Weiss L . A study of the germinal epithelium in male paraplegics. Am J Clin Pathol 1950; 20: 24–34.
Bors E, Engle ET, Rosenquist RC, Holliger VH . Fertility in paraplegic males: a preliminary report of endocrine studies. J Clin Endocrinol Metab 1950; 10: 381–398.
Leriche A, Berard E, Vauzelle JL, Minaire P, Girard R, Archimbaud JP et al. Histological and hormonal testicular changes in spinal cord patients. Paraplegia 1977; 15: 274–279.
Perkash I, Martin DE, Warner H, Blank MS, Collins DC . Reproductive biology of paraplegics: results of semen collection, testicular biopsy and serum hormone evaluation. J Urol 1985; 134: 284–288.
Elliott SP, Orejuela F, Hirsch IH, Lipshultz LI, Lamb DJ, Kim ED . Testis biopsy findings in the spinal cord injured patient. J Urol 2000; 163: 792–795.
Foresta C, Ferlin A, Bettella A, Rossato M, Varotto A . Diagnostic and clinical features in azoospermia. Clin Endocrinol (Oxf) 1995; 43: 537–543.
Wieder JA, Brackett NL, Lynne CM, Green JT, Aballa TC . Anesthetic block of the dorsal penile nerve inhibits vibratory-induced ejaculation in men with spinal cord injuries. Urology 2000; 55: 915–917.
Brackett NL, Lynne CM . The method of assisted ejaculation affects the outcome of semen quality studies in men with spinal cord injury: a review. NeuroRehabilitation 2000; 15: 89–100.
Brackett NL, Ferrell SM, Aballa TC, Amador MJ, Padron OF, Sonksen J et al. An analysis of 653 trials of penile vibratory stimulation in men with spinal cord injury. J Urol 1998; 159: 1931–1934.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Iremashvili, V., Brackett, N., Ibrahim, E. et al. The choice of assisted ejaculation method is relevant for the diagnosis of azoospermia in men with spinal cord injuries. Spinal Cord 49, 55–59 (2011). https://doi.org/10.1038/sc.2010.91
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.91
Keywords
This article is cited by
-
Sexual Health in the Neurogenic Patient
Current Bladder Dysfunction Reports (2020)
-
A step-wise approach to sperm retrieval in men with neurogenic anejaculation
Nature Reviews Urology (2015)
-
Management of ejaculatory disorders in infertile men
Asian Journal of Andrology (2012)
-
Male sexual dysfunction and infertility associated with neurological disorders
Asian Journal of Andrology (2012)
